
Abstract
Uninsured primary care patients tend to experience barriers to autonomy in clinical decision-making due to limited choices of healthcare facilities and low health literacy. This study examined whether certain factors, including the component of patient-centeredness, are associated with patient autonomy among these populations and contribute to reducing disparities in healthcare. This was a cross-sectional study using a convenience sample of free clinic patients aged 18 years and older who spoke English and/or Spanish. Multiple regression analyses were performed to understand factors associated with Ideal Patient's Autonomy. Data were collected from September to December 2019. Findings conclude that Spanish-speaking patients at the free clinic have a stronger belief in a paternalist model of the provider–patient relationship (P < .01). Better communication between patients and providers results in higher levels of autonomy (P < .01). Higher levels of educational attainment and better communication partnership were associated with higher levels of a free clinic patient's understanding of treatment risks (P < .01). This research study found that components of patient-centeredness are important considerations for improving patient autonomy among free clinic patients.
Introduction
According to the self-determination theory, autonomy is one of the fundamental human rights. 1 Autonomous decision-making results in more consistent behavior and overall better well-being. 2 Patient autonomy is a core principle in the healthcare system, and centers on a patient's right to experience independent freedom of choice about their health and medical treatment without their care provider unduly influencing the decision. 3 Patient autonomy in clinical settings can lead to more successful outcomes and increases in patient levels of satisfaction with healthcare. 4 Therefore, healthcare providers are encouraged to be supportive of patient autonomy in practicing decision-making regarding their treatment that matches their value. 5
Research has shown that patients who have limited autonomy may not feel empowered to ask questions or advocate for themselves and may have worse health outcomes overall. 6 Additionally, these disparities in healthcare can perpetuate inequalities, as those with limited access to healthcare and autonomy in decision-making may be at greater risk for poor health outcomes.
Patient autonomy is a critical component of shared decision-making (SDM) in healthcare. When patients are given the opportunity to make informed decisions about their care, they are more likely to have better health outcomes. Shared decision-making involves a collaborative process in which healthcare providers and patients work together to make healthcare decisions based on the patient's values, preferences, and medical evidence.7,8
According to Norman Cousins, patient participation in decision-making may improve patients’ quality of life; however, this notion may not apply to all populations as people may not have equal self-confidence. 9 For example, privileged middle-class people have higher access to resources and may have higher confidence when it comes to their participation in clinical settings, leading to better health outcomes. Existing literature indicates that many factors contribute to the amount of autonomy a patient exhibits in making medical decisions. 10
Uninsured primary care patients tend to experience barriers to autonomy in clinical decision-making. These barriers may include limited access to healthcare resources, low health literacy, and cultural or linguistic barriers. Additionally, uninsured patients may face challenges communicating with their healthcare providers and understanding complex medical information. These barriers can impact patients’ ability to participate actively in SDM and make informed choices about their care. Factors associated with patient autonomy among uninsured populations is an important but understudied topic due to limited choices regarding access to providers, specialty care, and healthcare facilities among these populations. This study will fill that gap and contribute to reducing disparities in healthcare evaluating and describing the level of free clinic patients’ agreement to ideal patient autonomy.
The purpose of this study is to examine the factors associated with levels of autonomy among free clinic patients. More specifically, we examined whether certain factors, including the component of patient-centeredness, are associated with patient autonomy. Communication and partnership with healthcare providers can enhance patient autonomy by facilitating informed decision-making, empowering patients to express their needs and preferences, and supporting patients in navigating the healthcare system. Studies have shown that economically disadvantaged people and ethnic minorities have less autonomy and worse health than their counterparts. 11 The British epidemiologist Michael Marmot has argued that individuals in the lower levels of the social hierarchy have less autonomy regarding their health. 12 Therefore, having a lower socioeconomic status correlates with worse health outcomes due to decreased autonomy. Because higher levels of patient involvement are associated with increased patient-centered care levels, it is important for providers to involve patients in treatment, diagnosis, and medication instructions. 13
The value of this study lies in its contribution to the understanding of factors associated with patient autonomy and reducing disparities in healthcare for uninsured primary care patients. Thus, we hypothesized that higher levels of patient-centered care are associated with higher levels of patient autonomy.
Methodology
Setting
This cross-sectional study was approved by the Institutional Review Board. Free clinics are a suitable setting as they are often the only source of healthcare for uninsured individuals, making them an important setting for studying the healthcare needs and experiences of this population. This study was conducted at one of the free clinics located in the metropolitan area in the Intermountain West of the United States. The clinic has been open since 2005 and has been providing primary and preventative services, including adult family medicine, diabetes specialty care, and healthy living classes. The clinic provides care to uninsured individuals who are not receiving Medicare, Medicaid, or employer-sponsored health insurance. In addition, uninsured individuals need to have a household income less than 200% of the federal poverty line to be eligible to enroll as a patient of the clinic.
Data Collection
Self-administrative paper surveys were collected in the clinic's waiting room area among 559 participants. Data were collected from September to December 2019. Participants were clinic patients 18 years or older who could speak English and/or Spanish. All survey materials, including a consent letter and survey instrument, were available in both English and Spanish. All English materials were prepared using the forward translation into Spanish and a second translator conducted the back translation. In addition, a third translator checked for the accuracy of the translated survey. Within the study period, a research assistant approached and recruited eligible participants during clinic hours in the designated waiting room area of the clinic before they are called to visit the healthcare provider. The consent cover letter and the survey instrument were handed to participants who exhibited an interest in taking the survey. Consent was obtained from each participant and their identity remained anonymous. Upon completion of the survey, each participant received a small compensation (eg, hygiene/sanitary product) for their participation.
Measures
Consultation Care Measure
The consultation care measure scale has been tested for validity and reliability and measures an individual patient's perceptions of patient-centered care during their most recent visit with a primary care or family physician. 14 The original questionnaire contained 5 subscales, however, in this study, we only used the first 2 domains of communication and partnership (11 items) and personal relationship (3 items) due to participants’ limited time and burden. Both subscales from the consultation care measure instrument use a 5-point Likert scale ranging from (1 = strongly disagree to 5 = strongly agree). Higher scores for both subscales indicate the more a doctor is interested in the patient's outcome and their needs. For the aspect of data analysis, the grand mean was computed as a total score for each domain. Each subscale had been tested for reliability. The Cronbach alpha for communication and partnership is .96 and Cronbach alpha for personal relationship is .89.
Ideal Patient Autonomy Scale
The Ideal Patient Autonomy Scale (IPAS) instrument has been tested for validity and reliability and is measured based on 14 normative questions. 15 The IPAS instrument is inspired by 4 different domains about ideals of patient autonomy and can be assessed among both patients and providers. The 4 domains are defined as “Doctors Know Best Scale,” “Patient Should Decide Scale,” “Obligatory Risk Information Scale,” and “Right to Nonparticipation Scale.” All statements use a 5-point Likert scale ranging from (1 = strongly disagree to 5 = strongly agree). For data analysis, the grand mean was calculated for each of the subscales. For each subscale, the higher score indicates the highest level of patient's agreement to the statements. The Cronbach alpha level for each of the subscales of “Doctors Know Best,” “Patient Should Decide,” “Right to Nonparticipation,” and “Obligatory Risk Information” were 0.83, 0.63, 0.66, and 0.63, respectively.
Sociodemographic Covariates
On the self-reported survey instrument, each patient reported age, gender, place of birth, race/ethnicity, educational attainment, employment status, marital status, self-reported general, country of origin, length of years living in the United States (for non-U.S.-born participants), and how long a participant had been a patient at the clinic.
Statistical Analysis
Data were analyzed using Rstudio, version 1.4.1717. Descriptive statistics were used to describe the study participant characteristics and present the summary distribution of the variables. Means and standard deviations (SDs) were used to summarize continuous variables, while frequency distributions were used to summarize discrete outcomes. Participants were classified and analyzed into 3 groups of U.S.-born English speakers, non-U.S.-born English speakers, and Spanish speakers, using analysis of variance. Multicollinearity was tested using variance inflation factor, and there was no significant multicollinearity among the variables.
Multivariable regression was performed using the 4 ideals autonomy scale domains including “Doctors Knows Best,” “Patient Should Decide,” “Right to Nonparticipation,” and “Obligatory Risk Information” as an outcome. The 2 subscales of consultation care scale, including “Communication and Partnership” and “Personal Relationship,” were used as the main independent variables. The 3 study groups of U.S.-born English speaker, non-U.S.-born English speaker, and Spanish speakers were also used as independent variables. The following sociodemographic variables were included as covariates: age, race, ethnicity, gender (male = 1, female = 2), whether participants were born in the United States or not (U.S.-born = 1, non-U.S.-born = 0), whether the participant was a patient of the clinic for more than 2 years or not (less than 2 years = 1; 2 years or longer = 2), self-reported general health ranging from (excellent = 1 to poor = 5), educational attainment, employment status, and marital status.
Results
Table 1 indicates the descriptive summary measures of the free clinic participants’ sociodemographic characteristics (total N = 559, U.S.-born English speaker n = 92; non-U.S.-born English speaker n = 140; Spanish speaker n = 327). Approximately 71% of the total participants were females. The total number of participants who were self-identified as Hispanic/Latino/Latina was more than 70% (n = 401, 71.7%, P > .01) and more than 67% of U.S.-born English speakers were White-non-Hispanic (n = 62, 67.4%, P > .01).
Sociodemographic Characteristics of Participants and Descriptive Statistics.a
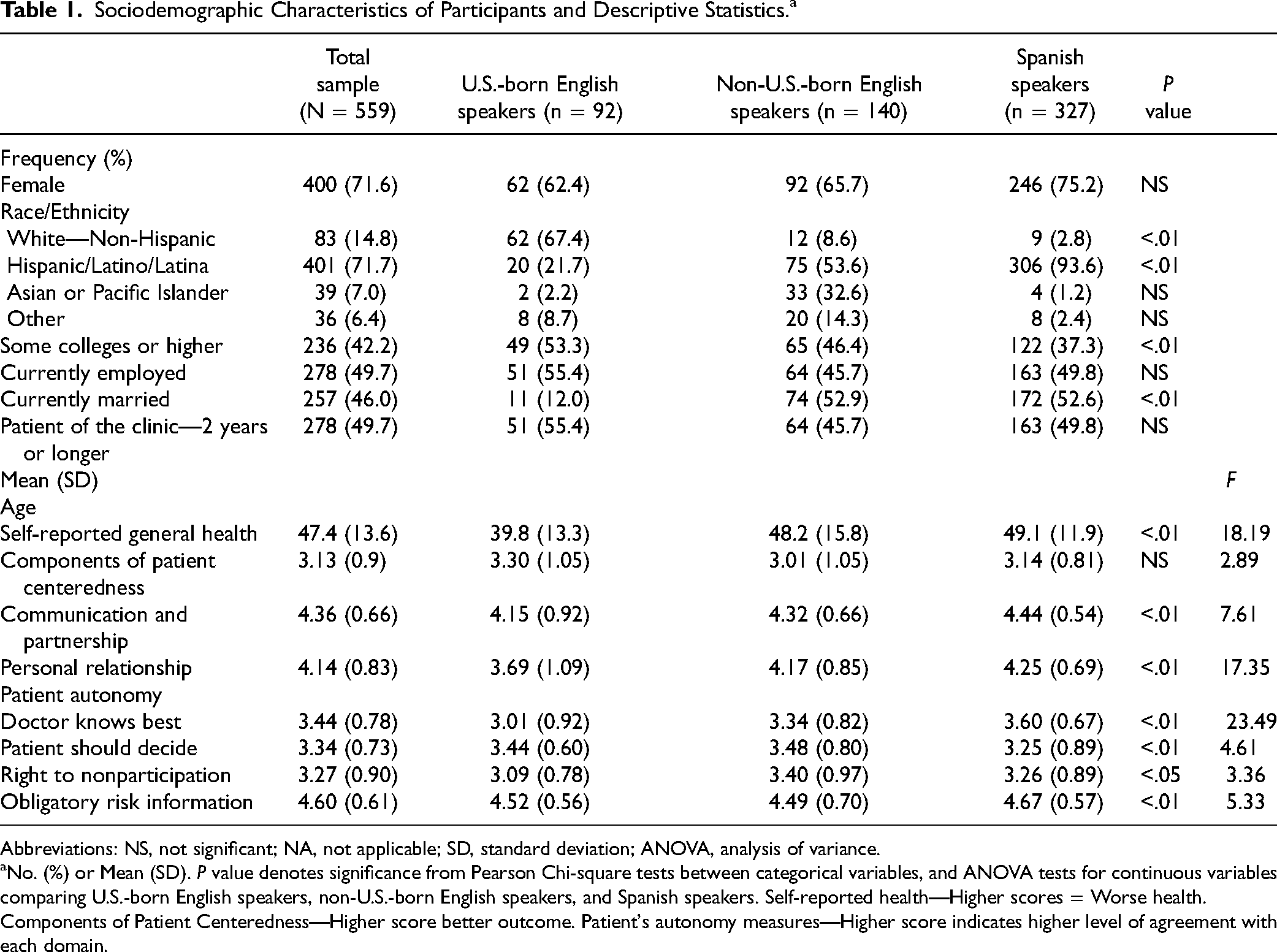
Abbreviations: NS, not significant; NA, not applicable; SD, standard deviation; ANOVA, analysis of variance.
No. (%) or Mean (SD). P value denotes significance from Pearson Chi-square tests between categorical variables, and ANOVA tests for continuous variables comparing U.S.-born English speakers, non-U.S.-born English speakers, and Spanish speakers. Self-reported health—Higher scores = Worse health. Components of Patient Centeredness—Higher score better outcome. Patient's autonomy measures—Higher score indicates higher level of agreement with each domain.
Among the 3 study groups, more than 40% reported to have at least some college as their educational attainment (n = 236, 42.2%, P < .01). U.S.-born English speakers had the highest percentage of educational attainment at the level of some college or higher (n = 49, 53.3%) compared to other study groups. Approximately 50% of the participants reported being employed (n = 278, 49.7%). Among the total sample, more than 45% of the participants reported being currently married (n = 257, 46%, P < .01). More than 45% of the participants reported being a patient of the free clinic for 2 years or longer (n = 278, 49.7%).
The average age of all participants was 47.5 (SD = 13.6) with U.S.-born English speakers being the youngest (39.8 [SD = 13.3]; P < .01). On average, non-U.S.-born English speakers reported having the worst health (3 [SD = 1.05]) compared to U.S.-born English speakers (3.30 [SD = 1.05]) and Spanish speakers (3.14 [SD = 0.81]).
As for the components of patient-centeredness, on average Spanish-speaking patients reported the highest level of communication and partnership and personal relationship with their provider compared to the comparison group (4.44 [SD = 0.54]; P < .01) and (4.25 [SD = 0.69]; P < .01), respectively. In addition, on average U.S.-born English speakers reported having the lowest level of communication and partnership and personal relationship with their provider (4.15 [SD = 0.92]; P < .01) and (3.69 [SD = 1.09]: P < .01), respectively. On the domain of Patient Autonomy, on average Spanish-speaking patients were the highest reporting that they believed their providers are the experts and know the best (3.60 [SD = 0.67]; P < .01), and they were also the highest in reporting that they received all the obligatory risk information regarding their treatment compared to others in the study groups (4.67 [SD = 0.57]); P < .01). On the other 2 main domains of patient autonomy, on average, the non-U.S.-born English speakers’ group was the highest in reporting that patients should decide, and physicians should respect patients’ decisions (3.48 [SD = 0.80]; P < .01) compared to the total participants (3.34 [SD = 0.73]; P < .01). Interestingly, non-U.S.-born English speakers were also the highest in reporting their right to nonparticipation (3.40 [SD = 0.97], P < .05) compared to the total participants (3.27 [SD = 0.90]; P < .05).
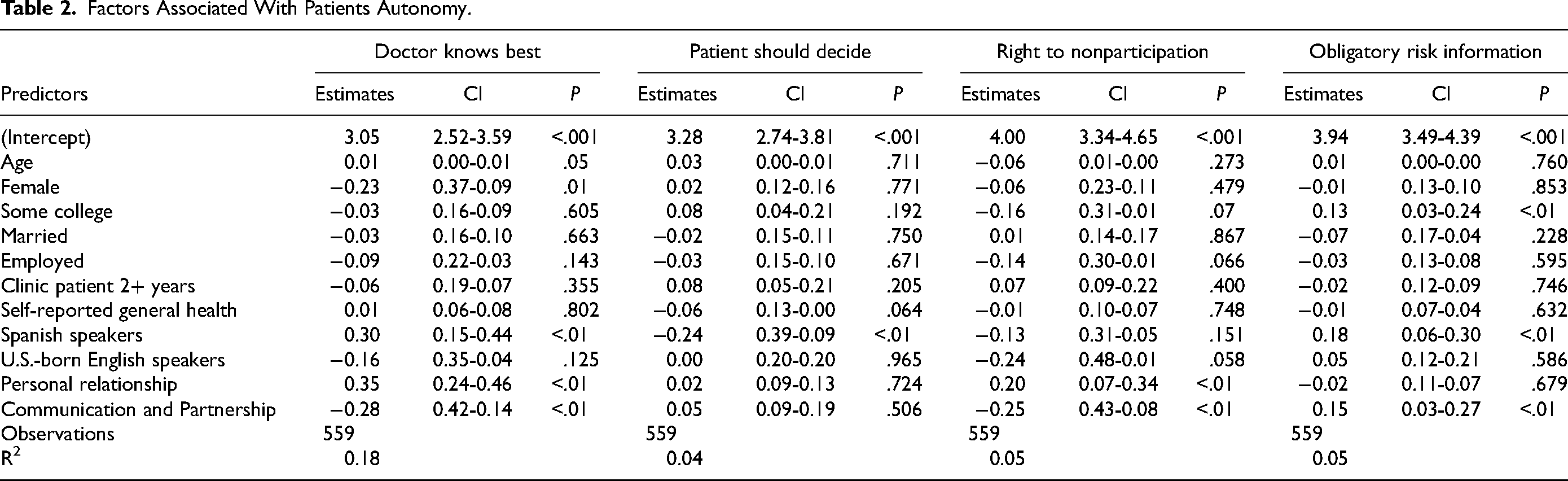
Table 2 presents factors associated with Ideal Patient's Autonomy. The multivariable linear regression results shows the following outcomes associated with 4 domains of patient autonomy. First, with each additional year of age, individuals had a higher level of agreement with “Doctors Know Best” (P < .05). In addition, being female and having a higher level of communication and partnership with a provider was negatively associated with levels of agreement to “Doctors Know Best” (P < .01). Lastly, speaking Spanish and having a better personal relationship with the provider was associated with a higher level of agreement to “Doctors Know Best” (P < .01). Second, the level of agreement to “Patient Should Decide” was negatively associated with Spanish-speaking patients (P < .01). Third, factors associated with a higher level of agreement with patients’ “Rights to Nonparticipation” was associated with higher levels of patient–provider personal relationship (P < .01); however, a higher level of communication and partnership was negatively associated with the level of agreement to “Right to Nonparticipation” including rights in decision-making (P < .01). Fourth, factors associated with higher levels of agreement with “Obligatory Risk Information” (that patients should be fully informed regarding risks) were associated with higher levels of patient–provider communication and partnership (P < .01), Spanish speakers (P < .01), and higher levels of educational attainment (P < .01).
Factors Associated With Patients Autonomy.
Discussion
This study examined the association between free clinic patients’ level of autonomy, components of patient-centeredness, self-reported health, and sociodemographic characteristics, resulting in 3 main findings. First, being a Spanish-speaking patient at the free clinic was associated with a stronger belief that doctors are the experts when it comes to decision-making about a treatment and that the patients should trust the doctor's expertise with less collaborative process, indicating less autonomy in this population. However, Spanish speakers were still in a position in which they wanted to receive all the risk information regarding their treatment. Second, better communication between patients and providers was associated with a higher level of autonomy (less belief in doctors know the best and patient's nonparticipation). Third, factors associated with a higher level of agreement with patients’ “Obligatory Risk Information” were related to higher levels of patient–provider communication and partnership and higher levels of educational attainment.
First, this result is consistent with a previous study, that when it comes to a sense of autonomy among Hispanic populations, they choose paternalism in their provider–patient relationship 16 . One of the reasons Hispanic populations prefer to have a high degree of paternalism in their relationships with their doctors and not participate in the process of decision-making is because of the great degree of intimacy they experience with their provider, especially their primary care doctors 17 . It is known that Hispanic populations are less likely to have a participatory relationship with their provider compared to other ethnic groups18,19. A qualitative research study among Hispanic and non-Hispanic whites also supports the result of this study, concluding that Hispanic patients, especially those with lower socioeconomic status, prefer to have their provider play the dominant role in making decisions about treatment and that they rely on the word of their physician to make their decision20,21. Therefore, since the majority of the free clinic patients in this study were self-identified as Hispanic, it is possible that they do have high trust and intimacy with their provider due to their culture and socioeconomic status, and that this is leading them to believe that their doctor knows the best; however, these patients still wish to be informed of all the risks associated with treatment.
Second, patient–provider communications are interactive and reciprocal, and as the provider role is important, patients are also responsible to be engaged, contribute, and communicate about their needs and preferences 22 . Patient–provider communications are the core clinical skills that encompass providers’ ability to gather more information on their patient and establish a relationship with them, resulting in increased patient participation 23 . Our result represents that better communication between patient and provider is associated with less belief among patients that doctors know the best.
In addition, the results of this study also indicate that better communication between patient and provider results in more patient participation in decision-making. Consistent with prior literatures, increased patient participation in a patient–provider communication promotes patients’ autonomy, resulting in better treatment adherence for the patient 24 . A previous research study has shown that the more providers use communication skills and a participatory decision-making style, the more patients are satisfied with the care, resulting in better patient outcomes 25 . Another study has also indicated that a provider communication style using supportive talk and cultivating a partnership with their patient is an important factor in patients’ involvement in care 26 . These results indicate that higher levels of patient autonomy are associated with patient-centeredness, including patient–provider communication partnership and SDM.
Third, informing patients regarding risk has been one of the major challenges in patient–provider relationships. Prior research supports the results of this study that receiving guidance from providers improves patients’ understanding of risks and, therefore, results in a satisfactory care outcome 27 . Therefore, higher levels of education are associated with better understanding of risks corresponding with a treatment.
Lastly, the findings of this study help inform interventions with the aim of improving patient autonomy among uninsured patients by emphasizing the importance of patient-centeredness, effective communication, and cultural sensitivity.
Limitations
Although this study is the first to contribute to knowledge regarding predictive factors associated with patient autonomy among uninsured patients, it has several noteworthy limitations. This study was designed using a cross-sectional methodology; therefore, causal direction between variables cannot be assessed. However, the result of this study discovered predictive factors which can be implemented in future longitudinal study. Data for this study were collected at one clinic and would be generalizable to other clinics with patients with similar characteristics but may not be generalizable to the general population. This study was only conducted among patients of the free clinic who speak English or Spanish; future studies are needed to explore a more diverse demographic among free clinic patients.
Conclusion
These results have significant implications for supporting free clinic motivations to facilitate better health outcomes, increase patient satisfaction, and support informed healthcare decision-making. This study highlights the importance of patient-centeredness and communication in promoting patient autonomy among this population. The finding that Spanish-speaking patients at the free clinic have a stronger belief in a paternalist model of the provider–patient relationship underscores the need for culturally sensitive and tailored interventions to address these beliefs and promote patient autonomy. We recommend free clinic providers to spend more time with patients by listening to them by providing them with reasonable alternative when it comes to decision-making. Future studies focusing on a longitudinal approach will help with understanding the causal relationship between the domains of patients’ autonomy and components of patient-centeredness.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231179041 - Supplemental material for The Impact of Patient Autonomy Among Uninsured Free Clinic Patients
Supplemental material, sj-docx-1-jpx-10.1177_23743735231179041 for The Impact of Patient Autonomy Among Uninsured Free Clinic Patients by Samin Panahi, Brenda Spearman, Justine Sundrud, Mason Lunceford and Akiko Kamimura in Journal of Patient Experience
Footnotes
Authors’ Note
This project was approved by the Institutional Review Board of the University of Utah.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.