
Abstract
Older adults and caregivers play an essential role in medication safety; however, self-perception of their and health professionals’ roles in medication safety is not well-understood. The objective of our study was to identify the roles of patients, providers, and pharmacists in medication safety from the perspective of older adults. Semi-structured qualitative interviews were held with 28 community-dwelling older adults over 65 years who took five or more prescription medications daily. Results suggest that older adults’ self-perceptions of their role in medication safety varied widely. Older adults perceived that self-learning about their medications and securing them are critical to avoiding medication-related harm. Primary care providers were perceived as coordinators between older adults and specialists. Older adults expected pharmacists to inform them of any changes in the characteristics of medications to ensure medications were taken correctly. Our findings provide an in-depth analysis of older adults’ perceptions and expectations of their providers’ specific roles in medication safety. Educating providers and pharmacists about the role expectations of this population with complex needs can ultimately improve medication safety.
Keywords
Introduction
Older adults’ views of their roles and professionals’ roles in medication safety are not well-understood to reduce preventable medication-related harms, resulting in over 700,000 emergency department (ED) visits annually (1). Older adults are more likely to visit the ED for medication-related harm than any other age group (2). Researchers found that over 65% of older adults in one study used more than five prescribed medications, which increased their risks for medication-related harm in terms of drug–drug interactions and medication use challenges at home (3). For example, nearly 100,000 ED visits are attributed to insulin-related hypoglycemia and other diabetes management errors each year, commonly due to reduced food intake and improper insulin administration at home (4). Such studies highlighted the need to understand the critical roles of patients in preventing medication-related harms. One national retrospective study found significant variations in patient reports of the communication about medicines across U.S. hospitals by location and access to health information technology (5). However, the level of support for using patient evaluations to manage medication safely in outpatient and community settings is highly variable and very limited.
Older adults and caregivers play an essential role in medication safety in community settings compared to acute care settings. Picking up prescriptions, preparing pillboxes, reading drug instructions, and accurately taking medications are among the tasks older adults perform to self-manage medications (6). Medication safety in the outpatient setting may be driven by how older adults view their roles. Older adults may have strong views of their abilities to manage their medications based on their experiences (7). They may also have strong opinions on the roles of prescribers and pharmacists (8). Community-dwelling older adults may prefer to speak with pharmacists rather than primary care providers (PCPs) for medication advice and education (9, 10).
A shared understanding of each person's role in medication safety is necessary for shared decision-making among older adults and health providers (11, 12). Such knowledge is also essential to embody the “coproduction model” of health services, in which patients and health providers form a partnership during the production of health care (13). We set out to discover how community-dwelling older adults taking five or more prescription medications perceived their roles and those of pharmacists and providers in medication safety.
Methods
We used a phenomenological method to obtain perspectives of community-dwelling older adults by conducting semi-structured interviews (14). With Institutional Review Board approval, Spanish and English-speaking individuals 65 years or older were invited to participate with the following inclusion and exclusion criteria: reporting five or more prescription medications, living independently or with a caregiver in the community, and not self-identified as having impaired decision-making capacity. No cognitive screening tools were used. Recruitment occurred at three sites using purposive sampling: a retirement community (independent living) and two-family medicine clinics in an urban area. We also encouraged caregivers to join the interviews.
Recruitment
Recruitment flyers and a project video briefing on the internal residential television channel were used at the retirement community. To improve transferability of study results (14), we informed all retirement community residents (approximately 200 residents) about study participation opportunities through the community's closed-circuit television. At the two clinics, healthcare providers were encouraged to identify all potential older adults who fell into recruitment inclusion-exclusion criteria and permitted to be contacted by the study personnel. Prospective older adults were screened for eligibility and were contacted by study personnel for written consent and time preference for an interview.
Data Collection
The data were collected from a semi-structured interview guide with 12 questions (see Supplemental material). These questions were designed to explore perspectives and experiences on medication safety, including during COVID. To focus our analysis on perceived roles by older adults, we chose to analyze responses to question six; “What is your role in taking medicine safely? What is your pharmacist's role? What is your doctor's role?” In addition, we assessed the responses to other questions to ensure that authors did not miss any substantive responses on roles. Patient demographics (age and sex) and major health conditions (including medications, if participants could recall) were also obtained. A $10 gift card was provided at the end of the interview. Interviews were conducted in English and Spanish, and researchers kept interview notes. A native Spanish-speaking team member conducted all Spanish interviews and validated translated transcriptions. Interviews were halted upon data saturation when no new themes emerged.
Data Analysis
The interviews were transcribed and translated professionally. Transcripts were reviewed for accuracy by the interviewers. Six team members coded six of the initial transcripts to develop initial codes. Team members met weekly to compare and discuss codes. At least two team members used the final codebook to code the rest of the transcripts. Braun and Clarke's six stages of inductive thematic analysis were utilized to analyze the transcripts through iterative coding using NVivo Version 12 (QSR International) (15). Themes were identified based on occurrence and agreed upon by the team. The coproduction of healthcare service theoretical framework guided a deductive approach to data analysis (13). To ensure data credibility, skilled researchers conducted peer debriefings throughout the study.
Results
The study included nine residents from the retirement community and 19 patients from two clinics. Two participants were accompanied by their caregivers. The mean age of older adults in this study was 75 years (SD = 7.5). Majority were female (67.9%, n = 19). The average number of daily medications was 7.7 (SD = 2.5). More than half (54%) of the participants had a college education. All Spanish-speaking older adults (n = 8) were recruited from the two clinics. All residents of the retirement community had at least some college education. See Table 1 for more detailed demographic data. Primary health conditions reported by participants were cardiovascular disease, diabetes, depression, kidney disease, osteoarthritis, glaucoma, neuropathy, urinary incontinence, chronic obstructive pulmonary disease, lymphoma, valve replacement, and back pain. Medications reported by older adults were insulin, citalopram, pregabalin, quinapril, oxybutynin chloride, atorvastatin, metoprolol, losartan, furosemide, clopidogrel, glucosamine, fluoxetine, warfarin, alprazolam, hydrocodone, and carvedilol.
Demographics Summary n = 28. a

Notes: *SD, standard deviation.
Percentages may not add up to 100 due to rounding.
We identified several themes that were grouped into three categories: (1) older adult's perception of the provider's role (themes: prescribing safely, monitoring for safety, and keeping up with recalled medications), (2) older adult's perception of the pharmacist's role (themes: notification of changes, monitoring for safety, keeping up with recalled medications, and providing medication package inserts), and (3) the perceived older adult's or caregiver's role (themes: taking fewer medications, not missing doses, securing medications, and learning about medications). A deductive approach to data analysis using the coproduction model revealed several themes that directly fit into the framework (see Table 2). Adapting themes into the coproduction of healthcare service framework added new insight to our understanding of the perceived roles of older adults. The themes are discussed below.
Coproduction of Healthcare Services Framework and Perceived Roles in Medication Safety.

Older Adults’ Perception of the Providers’ Role
Older adults acknowledged that providers have a considerable role in medication safety. This perception was rooted in the quality of the patient–provider relationship. These overarching themes of the provider's role are discussed below.
Theme 1: Prescribing Safely
Older adults expected providers to have the necessary knowledge, skills, and qualifications to prescribe their medications safely. Providers were expected to initiate individualized care by knowing all medications older adults took at home. “They’re supposed to know what's good for you and prescribe it when they feel like you need it” (OA6). Providers were expected to be knowledgeable about current medical practice guidelines and changes in healthcare. Providers were expected to have readily available resources to consult whenever necessary. “His job is to understand what medications I need, and if my labs show a problem, he knows immediately. And if he doesn't know immediately, he has references that he turns to and gets the information he needs.” (OA4)
Subtheme: Coordinating care
PCPs were expected to coordinate care with other providers. Several older adults had specialists who prescribed medications for them. PCPs were expected to perform a comprehensive review of prescribed medicines by all providers seen by the patient: “… and the primary care is supposed to be the one that oversees and coordinates all of the specialists that I’m seeing” (OA2).
Subtheme: Communicating with older adults
Older adults stated that the time spent with providers varied, and some allowed more time for questions regarding medications. The provider was also expected to perform basic physical examinations and order blood tests to help older adults feel at ease. One older adult stated that the provider neither assessed her lungs nor ordered any labs during her visit. She felt that her assessment was inadequate, and she was concerned about the safe prescribing practices of the provider. Regarding shared decision-making, older adults mentioned deferring prescribing decisions to the provider: “I don't ask no questions because I figure the doctor knows what he's doing” (PT4).
Theme 2: Monitoring for Safety
This theme included referencing drug interactions and disease interactions. An older adult emphasized that health providers must consider safety for patients with preexisting conditions such as decreased kidney function before prescribing medications. “I expect him to know that I have a little bit of issue with kidney function, and he needs to make sure that he gives me what's going to be the safest for my kidneys and yet do the most for whatever he's trying to control.” (OA3)
Providers were expected to monitor drug–drug interactions and avoid prescribing those medications. One older adult shared that they were “already taking so many medicines, so I don't know what will contradict with the other” (PT5).
Theme 3: Keeping Up with Recalled Medications
Older adults expected providers to keep up with recalled drugs and “to make sure that they’re not giving…medicine that has been recalled” (OA9). In addition, they want to be notified when a replacement medication is prescribed for a previously recalled drug: “let me know that they are going to give me another prescription for the purpose of … the one that has been recalled” (OA9).
Older Adults’ Perception of the Pharmacists’ Role
Older adults acknowledged having a positive relationship with the pharmacy staff. Some of the perceived roles of pharmacists overlapped with the providers’ roles.
Theme 1: Notification of Changes
Older adults mentioned that they relied on the appearance of medications to ensure they were taking them safely. Therefore, they expected the pharmacist to notify them of any changes to their medications’ dosage, shape, size, or color. “I got a medication with no warning, and then I was to cut it in half. The one I was taking before, I didn't have to cut it in half. I took it one time, a full pill, but then I saw on the label that I’m supposed to cut it and only take half. So obviously, they changed the company. They didn't tell me that I needed to cut it in half.” (OA5)
Theme 2: Monitoring for Safety
This theme was similar to the expected role of the provider. An older adult mentioned that their pharmacist had a list of all their medications; therefore, the pharmacist should also monitor potential drug interactions. “Pharmacists, they’re supposed to be able to know if there's any conflict between any medications. They know what I’m taking and the local pharmacy also has the list that I get for my 90-day stuff, so they can look at any of that.” (OA1)
Theme 3: Keeping Up with Recalled Medications
This theme was similar to the provider's expected role. Pharmacists were expected to function as a second layer of security when dispensing prescribed medications, especially routinely ordered medications. Pharmacists were expected not to dispense expired or recalled drugs, even if the provider ordered them. Older adults also mentioned that the pharmacist's role was to notify them of replacement medications.
Theme 4: Providing Medication Package Inserts
Older adults preferred reading the medication package inserts for specific drug information. The inserts were essential to help older adults understand the medication and its side effects. “[The role of the pharmacists is] filling the prescription that's given [to] them and giving me a sheet of paper that tells me the side effects or any warning that's on it” (OA6). However, some older adults said they were hesitant to ask the pharmacist drug-related questions; they expected pertinent drug information from the provider.
Perceived Older Adults’ and Caregivers’ Role
Older adults recognized that their role in medication safety went beyond taking pills as prescribed.
Theme 1: Taking Fewer Medications
Although older adults acknowledged taking several medications, they also believed it was necessary. Older adults perceived their role in medication safety as taking fewer medications by “eating healthier” (PT8) so that they “don't need to take so many pills” (PT8). “In response to the question of “what is your role in taking medications safely?” one older adult commented, “take less and less, I don't like to take more than I have to, nobody wants to, unless they just like medicine, nobody wants to take any more than they have to” (OA6).
Theme 2: Not Missing Doses
Additionally, older adults perceived that it was their role to take medications and not miss any doses. This perceived role was similar to caregivers’ perception as well: “to make sure she [patient] doesn't miss any, that she has all of them, that she has all the normal medication there at the house, to prepare it for her weekly” (PT3). However, several of the older adults reported forgetting to take their medications despite using tools such as pillboxes: “there have been days when I forget, and I’ll know because I’ve checked the day before, and they’re still there [in the pillbox]” (OA5).
Theme 3: Securing Medications
Older adults mentioned that some of the medications they took were controlled substances and had the potential for abuse. Consequently, another perceived role was locking away such medications to avoid them falling into the wrong hands. “They are locked up for one thing because occasionally I have to take hydrocodone, and my doctor told me to lock them up” (OA8). Older adults also expressed their awareness of the potential to abuse some of these drugs: “I don't like to take more than I have to. I don't want to get addicted to anything” (OA10). An older adult mentioned that her role was to ensure that medications were kept away from pets.
Theme 4: Learning About Medications
Older adults stated that asking questions was a crucial part of their role in learning about their medication. According to older adults, it was their role to read and follow prescription instructions. The medication inserts were used as a source of primary information, and the provider was consulted if there were further questions. “They’ll send an information sheet and so I read that very thoroughly. And if I have any questions about it, I’ll ask my doctor when I see him” (OA5).
Discussion
Our findings build upon the growing literature on medication safety by providing an in-depth analysis of older adults’ perceptions and expectations of their providers’ specific roles in medication safety. Pharmacists and providers were perceived to have some overlapping roles (see Figure 1). In contrast, older adults perceived their roles in medication safety as independent of health professionals’ roles. Older adults assumed a passive role in shared decision-making surrounding safe prescribing due to trust in the provider's knowledge, skill, and expertise. The role of safe medication management was viewed as achieved by attending to the physical appearance of drugs. Hence, pharmacists were expected to notify older adults of any changes to the appearance of medications. By contrasting the roles of prescribers, pharmacists, and patients, our study provided new insights on gaps and misconceptions in the coproduction of medication safety in ambulatory settings. For instance, older adults in our study expected coordination of PCPs with specialists and pharmacists. Also, they expect PCPs to have complete knowledge of their medications. Our study on perceived roles may inform the implementation of strategies to engage patients in medication safety. For example, Sharma et al (2018) assessed several strategies, including self-monitoring and titrating of anticoagulants, but for such strategies to be effective, patients and professionals must address the differences in perceived roles in medication safety (16).
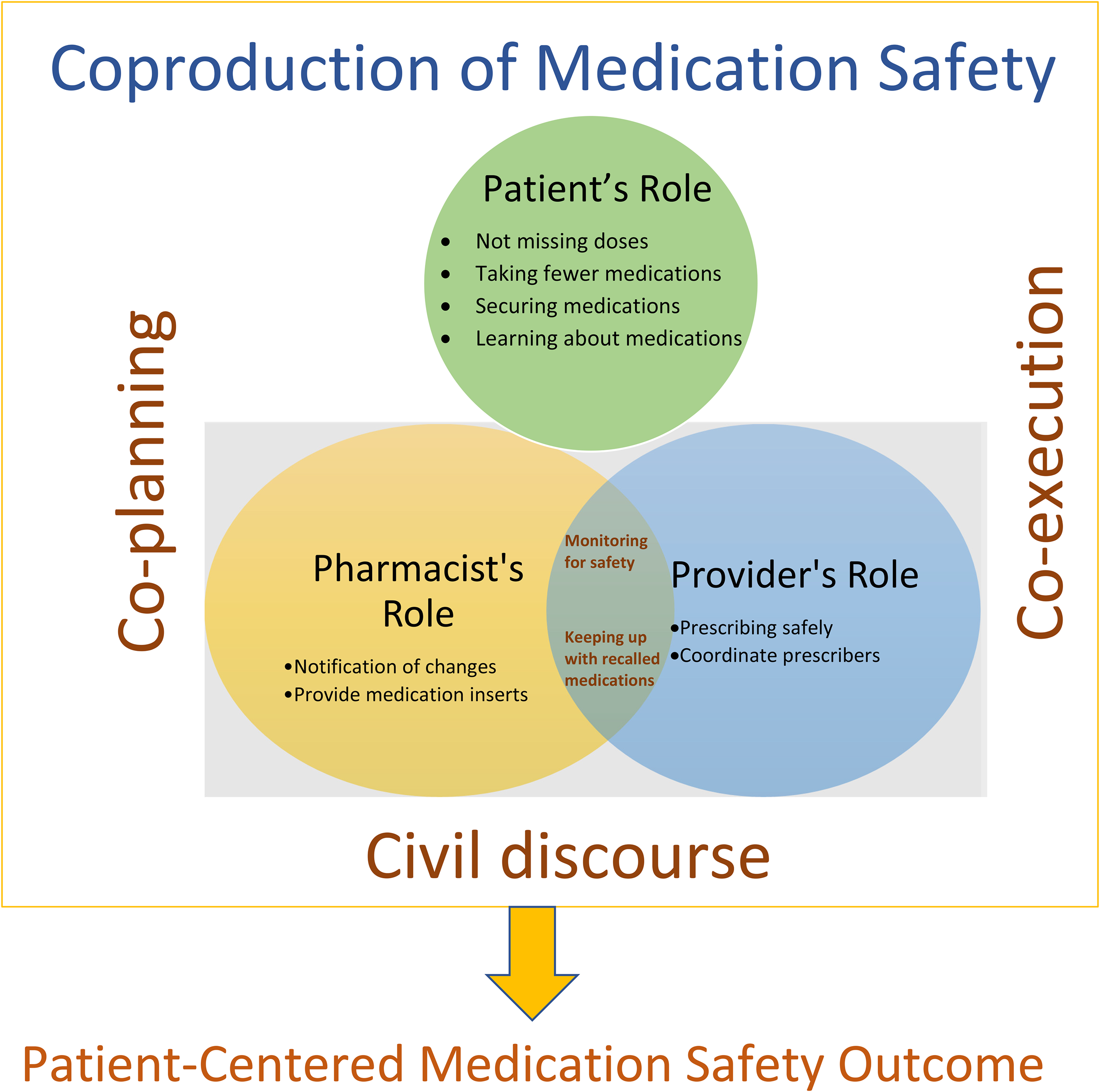
Coproduction of medication safety model: Older adults' perspective.
Similar to our findings, researchers found that older adults’ trust in healthcare providers contributed to their reluctance to participate in decision-making (17). During clinical encounters, providers should be aware of such tendencies and create opportunities for patients to express desired health outcomes (18). Among older adults in our study, “learning about medications” was perceived as their responsibility. Therefore, providers should assess and encourage older adults’ desire to learn about their medications. Individuals vary in how they view their role in medication management; thus, it is important to understand each individual's perceived role in medication safety (19).
Older adults in our study sample relied on the pharmacist for drug safety information, such as the medication inserts that came with their prescriptions. Besides providing medical advice without an appointment, the pharmacist could also be an intermediary between the patient and the provider (20). However, researchers found a lack of two-way communication between providers and pharmacists (21). Researchers also discovered that pharmacists’ lack of access to patient medical records was a significant barrier to making recommendations to providers regarding patients’ medications (22). Therefore, pharmacists need to have access to electronic medical records to make informed medication safety recommendations to clinicians (23).
In our sample, some older adults deferred prescribing decisions to the provider even though they would like to be “taking fewer medications.” Providers should respect and be aware of older adults’ desire to take fewer medications and assess for possible self-dosing practices. Viewed from the perspective of coproduction of health services, further education is needed to align perceived roles by older adults and caregivers regarding the long-term use of medication and the need to stop when necessary. Clinicians would agree that sometimes deprescribing medication is necessary; however, some older adults hesitate to stop their medications because they fear the consequences. Australian researchers also found that older adults were hesitant to participate in deprescribing (20). A jointly made decision between the pharmacist, the provider, and the patient must be made regarding deprescribing (21). Although many older adults do not want to be “missing doses,” they can sometimes be forgetful. Therefore, clinicians should assess cognitive barriers and access to tools to help mitigate risks.
Our findings confirm that older adults expected providers to be knowledgeable and maintain continuing education requirements (24). Older adults in our study also expected providers to review all their medications thoroughly during each visit due to concerns about drug interactions (17). These findings indicate that a comprehensive medication reconciliation should be the role of PCPs, who were also expected to coordinate and oversee the care patients received from other health specialists. Older adults in another study stated that medication reconciliation was one of the top five critical things to them during an annual wellness visit (25). Therefore, providers should incorporate an in-depth medication review during each visit. Unfortunately, the standard 15- to-25-minute office visits may not allow a thorough review of medications. Researchers found that a pharmacist spends an average of 34 minutes during a medication review session (22). Fast-paced clinic visits (26), lack of workflow integration (27), lack of privacy (28)’ and limited support staff (29) create organizational barriers to comprehensive medication therapy management (MTM) within outpatient clinics. In addition, poor information sharing between prescribers (28) and lack of pharmacist reimbursement (30) was also found to be a barrier to MTM.
Healthcare services depend on the coproduction of all team members, such as patients, providers, and pharmacists (13). Researchers have used the coproduction model to analyze clinicians’ perceptions of the model (31). Other researchers have used it to explore patients, refugees, and immigrants’ perceptions of the coproduction of their healthcare services (32–34). In our study, coproduction between older adults, providers, and pharmacists was essential in ensuring medication safety. The theoretical model of coproduction of healthcare service proposes that patients participate in civil discourse, co-planning, and co-execution during health service production (13). This model is appropriate in our study because older adults are participants rather than just consumers of health services (see Table 2). Civil discourse requires effective and clear communication between patients, providers, and pharmacists. The goal of co-planning is to respect individual values and expertise, such as older adults’ experiences and strategies used at home to improve medication safety. Co-execution mandates trust, shared goals, accountability, and responsibility between patients and health providers.(13) Providing this level of service increases trust in the provider-patient relationship and the provider's competence. Understanding and supporting coproduction between older adults and health providers are key to promoting medication safety.
Limitations
The study had limitations. We did not screen for cognitive impairment or frailty, and those with cognitive impairment may face different challenges regarding medication management at home. However, the issues raised by the participants are common issues experienced by other age groups, and thus we believe our findings are transferable to populations with complex medication needs. This study was also limited by the age range of 65–84 years of the recruited participants. Future studies should target the oldest-old (>85 years) to capture the possible varying needs of this population. Deductive thematic analysis was guided by the coproduction of healthcare service theoretical framework, which may have introduced biases. Future studies focusing exclusively on the framework should refine the proposed coproduction model of medication safety. For instance, a cost-based approach to medication safety might be explored.
The modality of data collection varied in this study. The interviews were conducted remotely due to COVID-19 protocols. Some interviews were via video, while most were conducted via voice calls. Some retirement community residents used mail-in pharmacy services primarily; consequently, their interactions with pharmacists differed from those who used community-based pharmacies. Qualitative research seeks to transfer rather than generalize findings. Despite our study limitations, our results are transferable to similar samples and could improve medication safety practices.
Conclusion
Understanding the specific medication safety-related role expectations between older adults and health providers could prevent medication-related harm. Our findings should encourage providers and pharmacists to create opportunities to involve older adults and caregivers in decision-making to facilitate the coproduction of quality healthcare services and a clear delineation of roles. The implications for organizations and policymakers are improving care delivery and allowing health providers to spend more time caring for older adults with complex needs. Future studies should examine providers’ and pharmacists’ perceptions of their roles and evaluate how to ensure all stakeholders understand their respective roles regarding medication safety.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231158887 - Supplemental material for A Multisite Qualitative Analysis of Perceived Roles in Medication Safety: Older Adults’ Perspectives
Supplemental material, sj-docx-1-jpx-10.1177_23743735231158887 for A Multisite Qualitative Analysis of Perceived Roles in Medication Safety: Older Adults’ Perspectives by Fatoumata Jallow, Elisa Stehling, Zara Sajwani-Merchant, Kathryn M Daniel, Kimberly G Fulda, Anna M Espinoza, Ayse P Gurses, Alicia I Arbaje and Yan Xiao in Journal of Patient Experience
Footnotes
Author Contributions
Study concept and design: YX, KD, APG, AIA. Data collection: FJ, AE, ES, ZSM, and KD. Data analysis and interpretation: FJ, ES, ZSM, AE, KD, KF, APG, AIA, and YX. Drafting of the manuscript: FJ, ES, ZSM, AE, KF, and KD. Critical review of manuscript: KD, YX, APG and AIA. Obtaining funding: YX. Supervision: YX, KD. All authors contributed to the critical revision of the manuscript's intellectual content and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Texas at Arlington's Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality, (grant number R18HS027277).
Presentation
Abstract accepted for poster presentation for the Gerontological Society of America Annual Scientific Meeting 2022 in Indianapolis.
Abstract Title: Perceived Roles in Medication Safety—Patients’ Perspectives Abstract accepted for poster presentation at May 2022 Annual Meeting of the American Geriatrics Society:
Abstract title: Perceived Roles of Community Dwelling Multimorbid Older Adults in Medication Safety Select findings from this study were presented on a poster at the 2021 Annual Scientific Meeting of the Gerontological Society of America (GSA).
Abstract Title: Opportunities and Barriers to Medication Safety in Community-Dwelling Older Adults
Sponsor's Role
Sponsors had no role in the design, methods, recruitment, data collection, data analysis, and the development of this manuscript.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the University of Texas at Arlington's Institutional Review Board (IRB
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.