
Abstract
There is limited research evaluating the diagnosis and treatment of patients with autoimmune gastritis (AIG) and pernicious anemia (PA). We used a 2-phase data collection process to examine the literature and individual patient accounts. Phase one comprised a systematically conducted literature review focusing on diagnosis and treatment, relationships with healthcare practitioners and health-related quality of life (HRQOL). Phase two involved analysis of individual accounts via posts in online patient forums. We identified 6 main themes: the diagnosis journey, seeking treatment, patient-provider relationships, HRQOL, patient disempowerment, and the “expert patient.” Our findings confirm significant knowledge gaps concerning AIG/PA across the healthcare community. These have a cascading effect starting with delays in diagnosis and poor treatment protocols and often lead to complete withdrawal from care seeking. The establishment of standard consensus guidelines and improved clinical awareness should be urgently addressed. Interventions that better help patients understand their illness are also needed to improve psychological health. Without these changes disengagement from health systems, and poor health outcomes, will continue for this population group.
Introduction
Autoimmune gastritis (AIG) is a chronic inflammatory disease with gastric parietal cell destruction. Its prevalence varies from 0.5% (1,2). to 19.5% depending on the setting (1,3–9). AIG is slowly progressive and usually asymptomatic for years. However, it raises the risk of gastric cancers, reduces acid output and triggers malabsorption of several micronutrients including iron and vitamin B12 (1). Chronic B12 malabsorption results in pernicious anemia (PA) (1,4,10). PA is associated with neurological, hematological, and gastrointestinal manifestations and a broad clinical presentation. Diagnosis is often delayed; over half of AIG/PA patients have another autoimmune disease including thyroiditis and type 1 diabetes (1,11,12).
Research into such delays is limited but a recent study found an average delay of 14 months (13). AIG is frequently overlooked by endoscopists; in Japan only 31.7% of study participants received a confirmatory endoscopic diagnosis compared to 68.3% receiving their diagnosis pathologically (14). Hooper et al's survey of nearly 1200 UK patients found that one-third experienced a 12 month delay and 14% waited over 10 years for a diagnosis (15). They also found inconsistency concerning types of tests conducted and treatment prescribed (15). Less than one-third of respondents were satisfied with their treatment; half stated they received poor medical care (15). Patients with AIG have a decreased health-related quality of life (HRQOL) compared to healthy controls, largely attributable to impaired physical functioning (16).
In response to diagnostic delays and suboptimal treatment many turn to online discussion forums where patients devise their own protocols. Anecdotal evidence of successful self-management suggests a gap between “lived experience” and medical advice. We aimed to identify these gaps by exploring peer-reviewed literature alongside individual accounts of AIG/PA.
Methods
The study comprised 2 phases. Phase one was a systematic review of peer-reviewed literature exploring lived experience of AIG/PA patients focusing on diagnosis and treatment, practitioner relationships and HRQOL. Phase two involved analyzing individual accounts via posts in online patient forums.
Phase One
Search Strategy
Phase one involved systematically searching academic literature using 5 medical databases: PUBMED, EMBASE, MEDLINE, WEB OF SCIENCE, CINAHL. Search terms derived from the literature included PA, megaloblastic anemia, B12 deficiency, autoimmune atrophic gastritis, parietal cell antibodies, guideline, symptom, protocol, treatment, criteria, unmet needs, lived experience, patient journey, case study, prevalence, incidence, and a large array of related terms. Co-citation and bibliographic coupling listings were also identified using connectedpapers.com to identify relevant prior and derivative works.
Inclusion/Exclusion Criteria
Inclusion criteria were English language studies to August 2021 focusing on the patient journey. All designs including qualitative, quantitative, cross-sectional, and mixed methods research were included. Exclusion criteria were a lack of focus on HRQOL or patient journeys and a lack of focus on AIG/PA. About 869 papers were imported into Covidence, a software package supporting systematic screening and extraction of literature. After removing duplicates, 638 titles and abstracts were screened and 559 excluded (Figure 1). Seventy-eight full text articles were screened, with 69 excluded due to a lack of focus on patient experiences, or availability only in abstract or non-English form. Nine publications remained for inclusion and data extraction. One comprised 4 separate studies (3 quantitative and one qualitative) bringing the number of unique studies for analysis to 12 (Appendix).

Phase one literature search.
Analysis
The literature heterogeneity suggested a narrative synthesis analytic approach to identify common themes (17). This facilitates the identification of common stories and themes from multiple sources. Data from each study were extracted into a spreadsheet. Key themes included diagnostic delays, suboptimal treatment, and poor doctor-patient relationships. These were coded in line with areas of focus for this study: diagnosis experiences, treatment experiences, relationships with healthcare practitioners, and HRQOL.
Phase Two
This involved systematically searching online AIG/PA patient forums. A search identified active forums using search terms including support OR patient groups (AND) pernicious anaemia, autoimmune gastritis, and associated synonyms. Social platforms with AIG/PA support groups were found on Reddit, Healthunlocked, and Facebook (Table 1). Reddit was excluded; the only thread was comparatively small and relatively inactive. Healthunlocked, the social platform used by the Pernicious Anaemia Society (PAS), contained nearly 27 000 members and almost 20 000 posts. Nineteen English-language groups were identified on Facebook, comprising over 50 000 global members. Groups focusing solely on B12 deficiency were excluded. Three online groups—PAS (HealthUnlocked), Pernicious Anaemia Support (Facebook), and Pernicious Anaemia/B12 Deficiency-Support Group (Facebook) represented the largest number of members. The Autoimmune Atrophic Gastritis & Pernicious Anaemia group on Facebook were also included because of their specific focus on AIG.
Online Patient Forums.

*Groups included for data extraction.
Data Extraction and Analysis
Over 3 dates in September 2021 (6th, 11th, and 20th) the most recent 50 forum posts were extracted to a spreadsheet. Each was treated as a unit of data. Using Braun and Clarke's (18) thematic analysis framework, common codes and themes were identified and cross-referenced with literature. Analysis began with reading and coding each post independently. Taking a deductive approach, we looked specifically at data related to focus areas for this study—diagnosis, treatment, healthcare professional relationships, and HRQOL. Subsequent readings used an inductive approach to identify additional codes not previously considered. All codes were then summarized into 6 over-arching themes: the diagnosis journey, seeking treatment, patient-provider relationships, quality of life, patient disempowerment, and the expert patient (Figure 2).

Themes identified across the literature and patient forums.
Results
Phase One
Of the 12 studies, 9 originated in the United Kingdom, 2 in Italy and 1 in Germany. Seven were cross-sectional and 2 were single-center evaluations. Median sample size was 198 (range: 102-889). The 3 qualitative studies used semi-structured interviews and patient workshops involving 7 to 12 participants.
The cross-sectional studies were online surveys, with recruitment via advocacy groups like the PAS in the United Kingdom, B12 deficiency/PA information websites and online patient forums. The single-center evaluations were from a UK doctor's surgery and an Italian gastrointestinal clinic. The qualitative studies all recruited participants through the PAS member databases, university volunteer newsletters, and social media.
Phase Two
The 4 online forums represented a diverse collection of members, ranging from 1700 to nearly 29 300 worldwide participants (Table 1). The Facebook groups shared similar demographics: predominantly female (on average 92%), aged between 25 and 54 and mostly living in the United Kingdom, United States, and Australia. Demographics were unavailable for HealthUnlocked. Engagement was high in all groups; new posts averaged between 4 and 14 daily within individual groups, with up to 200 nested responses.
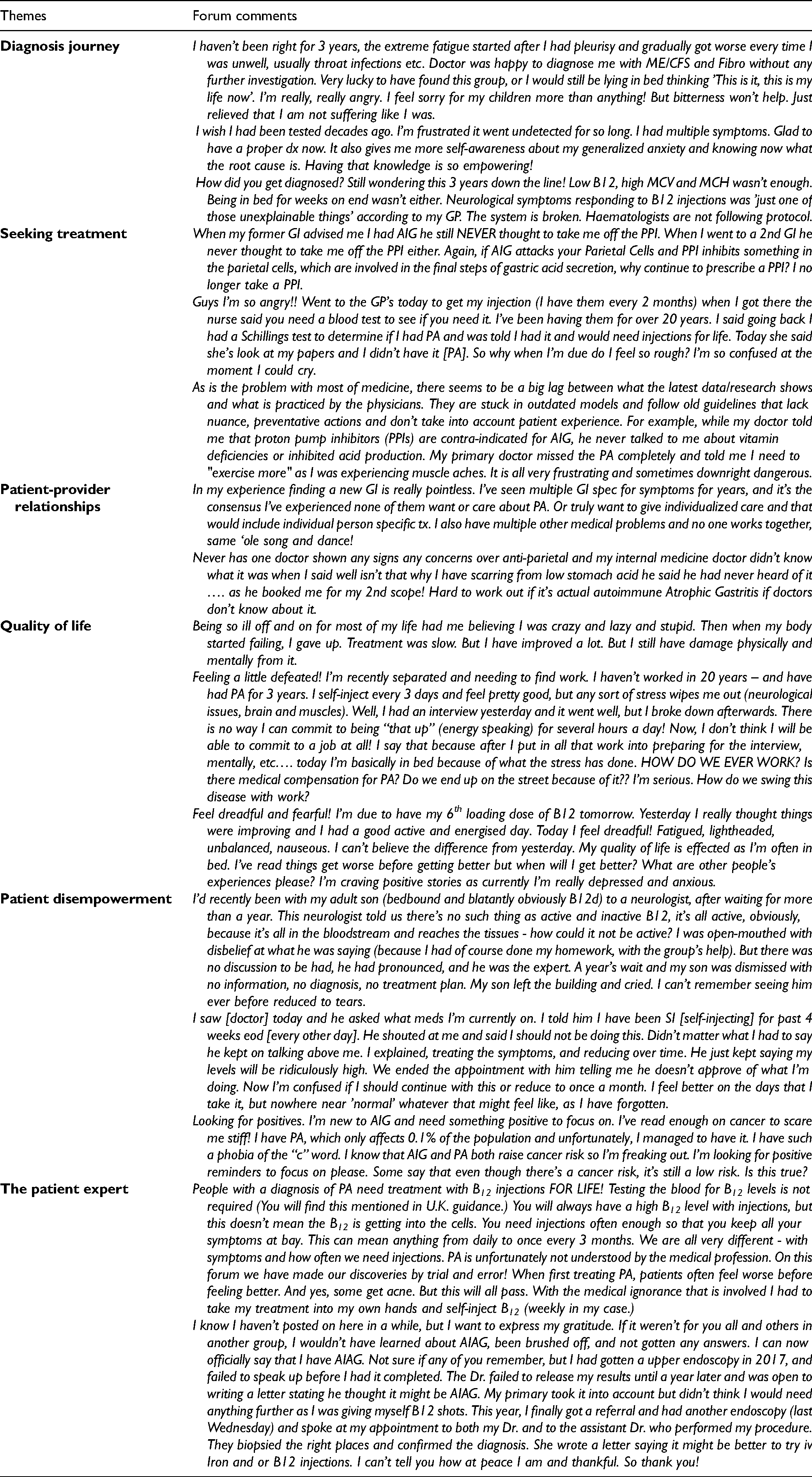
The 6 themes identified (see above) are considered consecutively, with illustrative forum quotes highlighting key themes (Table 2).
Illustrative Quotes From Online Forums.
Diagnosis Journey
The diagnosis journey was consistently described as “difficult” in the literature, with significant delays. Hooper et al found that 80% of patients described diagnostic delays of between 1 and 10 years (15). Lenti et al reported a median overall delay of 14 months; 65% of their study participants experienced delays of between 2 and 3 years and 8% more than 10 years (13). Many authors suggested this was due to a lack of awareness, lack of routine screening and inconsistencies across testing protocols and diagnostic criteria (13,15,19,20). Lenti et al found delays were longest for women, suggesting a confounding of menstruation and iron deficiency (13). Other confounding issues included autoimmune comorbidities in many patients (13). Paralleling the literature, forum participants also recounted misdiagnosis and diagnostic delays: PA for me took almost 15 years to diagnose. I only found out by doing my own research after years of misdiagnosis and being sent to multiple specialists on a wild goose chase, with so many weird symptoms that adversely affected my confidence and career, including my own sanity. I finally requested doctor to run an IF antibodies test. I was thrilled to be positive as B12 shots began and they immediately improved my overall symptoms.
Seeking Treatment
Suboptimal treatment was commonly described. Hooper et al's survey found that 64% of patients reported suboptimal care; 51% describing their care as poor or very poor (15). Across the literature inconsistent treatment was reported, including poor understanding of symptom severity and neuropsychological distress (13,15,19–23). Little is offered in terms of treatment for gastrointestinal issues; practitioners commonly prescribe proton pump inhibitors (PPIs) which are contra-indicated for AIG (13).
Forum participants often reported clinicians’ reliance on B12 biomarkers, leading to treatment cancellation despite symptom persistence. Current research indicates basic B12 biomarkers should not be considered without other essential markers, including holotranscobalamin, MMA, homocysteine, and patient symptoms (1,24). Frustration concerning the lack of patient-centered care and adherence to outdated guidelines was common (Table 2).
Patient-Provider Relationships
Across the literature and forums, participants expressed dissatisfaction with medical care, poor doctor relationships, and disengagement from healthcare (15,19,20,22,23,25). Many described symptoms that were frequently trivialized, leaving them feeling misunderstood and unheard (19,22). Seage et al reported high levels of stigma and a delegitimization of patient experiences (19). They found a perceived gender bias in patient-provider relationships with females commonly told their symptoms were stress-based, psychosomatic, or hormonal (19). Complaints concerning fragmented care and lack of patient-centered care were also commonly expressed (Table 2). Though “trust” and fragmented services were often identified, not all patients felt unheard: I have had brilliant treatment from my GP & get annoyed when they are all tarred with the same brush!
Quality of Life
Literature survey responses indicated that most people with AIG/PA experienced low HRQOL and psychological well-being compared with other gastro-intestinal diseases such as celiac disease (13,16). HRQOL results were poor across domains of physical functioning, bodily pain, general health, vitality, social functioning, emotional and mental health (16). Stigmatization was commonly described in the literature and individual forum stories: Being so ill off and on for most of my life had me believing I was crazy and lazy and stupid. Then when my body started failing, I gave up. Treatment was slow. I have improved a lot, but I still have damage physically and mentally from it.
Semedo found that a better understanding of AIG/PA positively enhances people's HRQOL (20). Cognitive deficits and psychological disturbances due to B12 deficiency were a common source of distress across the literature and forums (20,22,23). Semedo also found concerns around managing work due to physical and mental fatigue from stress and ill-health (20). Mirroring this, one forum participant explained that just preparing for and completing an employment interview left her feeling depleted and concerned for her future (Table 2).
Stigma was perceived across the main quality of life domains of health, work, and family (22). High anxiety levels were also common as people tried to deal with their condition and expressed concerns about their prognosis (20).
Patient Disempowerment
Patient forums provided additional data not identified in the literature. Lack of awareness in healthcare about AIG/PA had a cascading effect for patients who, like their doctors, did not fully understand their condition, its associated complications and its management. Across the forums, misinformation was commonly discussed. Patients often failed to realize how broad disease symptoms could be, or alternatively assumed that all ill health was caused by AIG/PA. Poor patient-provider relationships and HRQOL compounded fear, uncertainty, and disengagement from healthcare. One forum participant described feeling dismissed by a clinician who disregarded their understanding of B12.
Forum participants described benefits from self-administering B12 in response to symptom recurrence, but also reported a lack of approval and support from healthcare providers, creating self-doubt and concern.
Poor insight into their condition resulted in many forum members expressing concern for their long-term prognosis, particularly around the association between AIG and cancer (20). A poor understanding of micronutrient deficiency was also widespread. People living with AIG/PA commonly perceived stigma around the practitioner-patient relationship with the perception that practitioners may lose patience when patients constantly present with new symptoms (19,22).
The Expert Patient
Another novel theme identified via patient forums was the emergence of the “expert patient.” Widespread suboptimal AIG/PA treatment leads to the emergence of individuals who achieve high levels of self-efficacy and who invest significant time and energy into researching their condition. These forum participants frequently become community leaders, providing advice and encouragement to other members.
Some engage in long research discussions, offering theories and advising others of treatment based on anecdotes. Given the widespread lack of knowledge in general, these patient experts often become key forum players, with patients consulting them for treatment advice rather than arranging medical appointments (Table 2).
Patient experts commonly encourage others to self-educate and instruct their healthcare practitioners. Others offer informative commentary to fill information gaps. Newer members often expressed gratitude to patient experts for empowering them: …. after several attempts I just go to the experts now – you!
Discussion
Our study identified 6 themes concerning diagnosing and treating AIG/PA. Significant knowledge gaps exist. These have a cascading effect starting with delayed diagnosis and poor treatment which impact quality of life, lead to stigmatization, poor patient/doctor relationships, and often to complete withdrawal from care seeking (19,20,22,23,25).
Routine screening is commonly overlooked (13,15,20). Inconsistent testing protocols and guidelines contribute to delayed diagnosis (1,26–28). For example, there are currently more than 5 sets of UK guidelines on PA, all proffering different advice (29). Chronic B12 deficiency results in significant harm; diagnostic delays can lead to irreversible complications (13,16).
Lenti et al developed an AIG “red-flags” questionnaire incorporating 7 diagnostic features (neurological, gastrointestinal, hematological, cardiological, autoimmune, fertility, and family history) to help avoid such delays (30). They also identified affordable laboratory test scores to confirm AIG including parietal cell antibody, plasma MMA, and homocysteine (1,31). These collective scores, alongside gastric biopsies, are considered essential for diagnosis (30). Importantly, “normal” serum B12 and MMA alone do not exclude B12 malabsorption (27,32). Adopting a red-flags questionnaire would clearly promote early diagnosis.
Suboptimal treatment is common. Issues range from clinicians’ lack of awareness and inconsistent management to frankly inappropriate treatment. For example, the use of PPI's to inhibit acid production in AIG patients with reflux symptoms is common. Another issue concerns treatment based on B12 biomarkers despite evidence that, once PA is diagnosed, these become irrelevant (21,27,33). Continued testing is especially controversial when doctors discontinue treatment based on B12 laboratory ranges. This is a key source of negative practitioner-patient relationships (15,29).
Significant debate surrounds B12 dosage. Kornic found that symptoms were significantly improved with daily/weekly parenteral treatment rather than every 2 to 3 months (21). Hooper suggests there is no firm evidence for 3-monthly injections to treat PA (29). It is unclear why clinicians refuse additional supplementation or discourage self-treatment since B12 has no upper toxicity and few side-effects (15,21,27). The reliance of biomarkers over symptoms to guide treatment indicates a significant unmet need, likely resolvable using a more “patient-centered” approach. Moreover, research is urgently needed to explore individual variance in B12 treatment requirements.
Equally controversial is the debate over oral versus parenteral supplementation. A Cochrane Systematic Review found there is some evidence for oral B12 efficacy, although based on 2 small studies (34). While oral supplementation restores blood abnormalities, other research and forum anecdotal reports suggest it is ineffective for many; parenteral supplementation is recommended for those with neurological symptoms (1,21,27,28). Combined oral and parenteral supplementation often provides optimum symptom relief (21).
Wolffenbuttel et al identified and debunked 7 common myths associated with B12 treatment (27): (1) oral B12 equals or is better than parenteral to alleviate neurological symptoms; (2) once serum B12 is normalized treatment can be stopped; (3) elevated serum B12 requires treatment cessation; (4) more than 5 injections is harmful; (5) serum B12 should be tested after 3 injections to assess whether supplementation is working; (6) treatment should be stopped if symptoms worsen, and (7) treatment must stop during pregnancy. Correcting these myths would address many of the complaints in patient forums, indicating a need for improved education and standard consensus guidelines.
Patient-provider relationships are impacted by inconsistent and inappropriate treatment, gender-bias, perceived stigma, and delegitimization of patient experiences (19,20,22,23,25). Shared decision-making can result in happier patients, with improved health outcomes and quality of life (35,36). Across the literature there were also few mentions of the implications of broader nutrient malabsorption. Deficiencies in folate, iron, vitamin C, calcium, and vitamin D are commonly associated with AIG/PA, leading to various neurological, blood, and skeletal issues that directly impact HRQOL (15,37,38).
At the far end of the AIG/PA disempowerment spectrum sit the patient experts and community leaders. The patient expert is usually a veteran of the AIG/PA journey, who has studied the literature extensively and shares anecdotes and learnings for others’ benefit. Given the widespread lack of awareness of AIG/PA they become important leaders; people consult them for advice rather than seek medical help. Patient experts help newer members with improved health literacy and self-efficacy by pushing them to educate themselves and their doctors about AIG/PA. Using such experts as “consumer engagement consultants” (39) in the development of patient-centered guidelines might provide experiential input often missed by researchers and clinicians.
Limitations
Our literature search was conducted systematically to ensure all relevant publications were included; however, while ad-hoc citation and reference list searches were carried out, a more systematic process of searching may have identified additional studies. Online forums provide a unique insight into the “lived experience” of an international audience of AIG/PA patients; however, the countries represented were all high income, clearly introducing bias. Importantly, there is a tendency for forums to attract participants with biased views (eg, those dissatisfied with their diagnosis and treatment). Despite these limitations, our study provides unique insight into a diverse group of people experiencing a condition that frequently goes undiagnosed and under-treated.
Conclusion
This study is the first to examine empirical evidence on the lived experience of people with AIG/PA and the accounts of those engaging in online AIG/PA patient forums. It provides insight into the challenging journey such patients experience. Interventions to prevent diagnostic delays and improve clinical awareness should be urgently addressed through the establishment of standard consensus guidelines and education. The implementation of a “red-flags” questionnaire by primary health practitioners might assist early diagnosis and improve health outcomes. The reliance of biomarkers rather than symptoms to manage treatment is a significant unmet need, possibly resolvable by a “patient-centered” approach to AIG/PA. Interventions that provide patients with an improved understanding of their illness may also significantly improve psychological health outcomes. Using the experiences of AIG/PA expert patients as consumer engagement consultants might also prove beneficial. Without better awareness and understanding of this condition, improved patient HRQOL support and a patient-centered approach, disengagement from health systems will likely continue.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231151767 - Supplemental material for Examining the Diagnosis and Treatment Experiences of People Living With Autoimmune Gastritis and Pernicious Anemia
Supplemental material, sj-docx-1-jpx-10.1177_23743735231151767 for Examining the Diagnosis and Treatment Experiences of People Living With Autoimmune Gastritis and Pernicious Anemia by Martine Cotton and Andrew McCaddon in Journal of Patient Experience
Footnotes
Acknowledgements
The authors thank the indefatigable duo Dr Allyson Mutch and Dr Lisa Fitzgerald from the UQ School of Public Health for their invaluable guidance and support throughout this research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AM is a Scientific Advisor and shareholder of COBALZ Limited.
Ethical Statement
Written informed consent was obtained from legally authorized representatives for anonymized patient information to be published in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by COBALZ Limited, Pernicious Anaemia Society.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.