
Abstract
The comprehensive psychosocial assessment of children with cancer requires listening to them and understanding their point of view. The objective of this work was to know what the participating children with cancer thought about the hospital, which they considered to be the best and worst aspects of their experience. We conducted a qualitative study using semi-structured interviews with 27 children with cancer. The interviewer asked the participating children what they considered to be the best thing about the hospital and what they considered to be the worst. These conversations with them were recorded and transcribed, and a thematic analysis of these transcripts was conducted. Among the aspects of the hospital that the children rated most highly was the treatment they received from the health care staff. Among what the children considered the worst aspect of their experience was pain, particularly pain caused by medical procedures such as injections. The obtained results lead us to conclude that children have a complex view of the hospital and are capable of a detailed analysis that must be taken into account.
Introduction
As a result of medical advances, the survival of children with cancer has increased considerably (1). However, children and adolescents with cancer continue to face medical and emotional situations that can affect their overall psychological adaptation. The physical symptoms produced by the disease and the treatments (pain, nausea, vomiting, reduced mobility, and alterations in body image), together with the severity of their medical condition can generate emotional distress that prevents their correct psychosocial and school adaptation, or even exacerbate some premorbid psychological symptoms (2). To this should be added the family reactions, alterations in social relationships, deterioration of school progress, and the impact of the disease on the environment of the child or adolescent. The psychosocial impact of a pediatric cancer diagnosis on the child and their family is well established; but despite this, psychosocial care for children with cancer and their families is not systematically or consistently provided (3).
The comprehensive psychosocial assessment of children with cancer requires listening to them and understanding their point of view. These children will be hospitalized frequently, in longer or shorter stays, in a way that intensifies their experience of the health institutions. Listening to children in the hospital is not only their right but also a strategy to improve the quality of pediatric health services (4,5). Asking children about their experience in the hospital and analyzing their answers allows us to know and understand their point of view in hospitalization processes (6).
Children, like adults, react as they do according to the meaning they give to what happens to them and the situation in which they find themselves. What does the hospital mean to a child? Traditionally, adults—parents and health staff—have spoken about children’s experience in the hospital. The standard approach to measuring patient satisfaction in pediatrics overlooks the input of the pediatric inpatient and relies instead on contact with parents (7). There are few works in which the voice of the children themselves is directly collected in this regard. However, carefully considering the perspective of the pediatric patients is a key element in the design of child-centered care systems that respond to their needs not only for physical care but also for psychological and social care (4). The work set out below was carried out from this point of view of listening to children with cancer about their experience in the hospital. The goal was to learn what the participating children with cancer thought about the hospital, what they considered to be the best thing about their time in the hospital, and what they considered to be the worst.
Design and Method
A qualitative study was carried out through a series of semi-structured interviews with children admitted to a hospital for cancer treatments. The interviews were set up as conversations with the children about what they liked most and least about the hospital. To facilitate communication with the children, they were asked to draw a picture about the hospital during the interview. The interviews were audio-recorded after the children gave their consent. These recordings were transcribed verbatim, and a thematic analysis of these transcripts was carried out.
Setting
The study was carried out at the Hospital Universitario Niño Jesús, a 170-bed tertiary children’s hospital located in Madrid (Spain), specifically in the hemato-oncology department.
Ethical Approval
The study was approved by the hospital's ethics committee (ref. CI:R-0100/20). The parents were informed about the study protocol and their explicit authorization and signed informed consent were requested for their children to participate. Children’s assent was also sought to participate in the study. This assent was given verbally if they were under 12 years old, or by signing an informed consent if they were 12 years old or older.
Subjects
Children between 4 and 17 years old admitted to the onco-hematology and transplant service of the hospital during the data collection period (February–April 2021) were considered eligible to participate in the study. Finally, 27 patients (16 girls and 11 boys) participated in the study. The age distribution of the participants is shown in Table 1.
Age Distribution of the Participants.

Data Collection
The first author conducted all interviews. She is a social psychologist with experience in research on pediatric hospitalization. Purposive sampling was directed toward achieving the maximum variation in age and gender. Sample size was estimated to be sufficient based on the principle of theoretical saturation. Theoretical saturation was considered to be achieved when new topics no longer appeared in the interviews and a relatively similar number of children from different age groups had been interviewed. Once the eligible children were selected, the interviewer entered the child’s room accompanied by a hospital nurse, who introduced her to the child and their parents. After greeting the child and their companion, the mandatory documentation described in the ethics section was completed and then the researcher began the interview, explaining to the children, talked to the children about these issues, and asked them to draw a picture of the hospital, offering them the necessary materials. These conversations with the children about the best and worst aspects of the hospital took place in their hospital room and in the presence of the parent or surrogate caregiver, who could also participate in the conversation. These conversations were recorded in audio. Only two families declined to participate. In one case because the child had just had a haircut and was very emotionally affected and in another because the child was asleep during the period of data collection.
Data Analysis Procedures
The interviews conducted (n = 27) were transcribed literally. A thematic analysis of the transcripts of the interviews was carried out. Our goal was develop patterns of meaning across the transcription of interviews. An inductive approach for coding was used in the thematic analysis. We used the Atlas.ti software (version 22). A codebook was developed, including a priori codes and pop-up codes. Based on what the children had said, codes were developed that allowed synthesizing what the child had expressed verbally. These codes, in turn, were grouped into themes.
Results
In general, the children readily expressed their views on the issues raised. In total, we recorded and transcribed 5 hours and 50 minutes of conversations with the participating children about their views on the hospital and the hospitalization experience. The recorded conversations ranged from long conversations to other short answers from the children to questions about what they thought was the best and worst thing about the hospital. Only the children’s responses to these questions were recorded, which formed the core of the interviews. The length of these recordings was as follows: 4 lasted 5 minutes or less; 11 recordings lasted between 6 and 10 minutes, 4 recordings between 11 and 15 minutes, 6 recordings lasted between 16 and 20 minutes, one recording lasted between 21 and 25 minutes, and another lasted 30 minutes. The analysis of the interviews conducted with the children about their perspective of the hospital allowed us to define 53 codes related to positive aspects of the hospital and 43 related to negative aspects, all of them were included in the codebook. All these codes were grouped by affinity into 11 themes. These 11 topics are summarized graphically in Figure 1 and Table 2 includes examples of verbatim quotations for each of these topics. Each of these themes is discussed below, indicating the number of children mentioning it and the number of quotes that were coded in it, since it could happen that the same child mentioned one of the themes several times in the interview.
Pain and injections. Pain, particularly pain produced by medical procedures, is an almost ubiquitous fear in the interviewed children. Children fear receiving injections and being hurt in the hospital. This aspect stands out among what they consider to be the worst thing about the hospital. Eight children of the interviewees mention it expressly, and 13 quotes were coded in this topic, all of them very descriptive (see Table 2). The treatment by the health staff. The children insisted that they felt well treated by the health workers, especially the nurses. This issue was valued as one of the main positive aspects of the hospital. The younger children were more succinct in their expressions and, when asked what they thought was the best thing about the hospital, they mentioned “their friends, the nurses” or “their favorite nurses.” The adolescents described the processes of communication with the staff in more detail, referring to the best thing for them in the hospital. Eight children mentioned these aspects, and 13 quotes were coded in this topic (see Table 2). Positive aspects of the hospital facilities. In this topic, the children’s references to the child-friendly environment of the hospital, the drawings illustrating the halls and corridors of the hospital, stand out above all. Some children mentioned the views from their rooms. In some cases, reference was also made to positive aspects of the furniture, such as the comfortable beds. Of the 27 children interviewed, 12 mentioned these aspects, and 17 citations were coded in this topic (see Table 2). Negative aspects of the hospital facilities. The children also negatively rated some aspects that referred to the hospital facilities (the size of the room, the uncomfortable furniture, etc.). Seven children mentioned as what they liked least about the hospital aspects that had to do with the health center facilities and 12 citations were coded in this theme (see Table 2). Positive aspects of the hospital’s non-medical services. In this sense, the interviewed children mentioned the educational services, especially the hospital school, which they valued highly. But they also referred to entertainment services, among which having an internet connection in the room stood out. They also referred to the food as a positive aspect of the hospital, talking about it very often, praising it because they liked it, and valued it. However, some of them also complained because it was what they liked the least about the hospital. Nine children mentioned the issue of the hospital’s non-medical services, and they were coded in the 19 citations (see Table 2). Absence of services or inadequate non-medical services from the point of view of children. The children mention the lack of leisure and entertainment services for children as a distinctly negative aspect of their experience in the hospital. Eight of the interviewed children mentioned negative aspects that had to do with the lack of services in the hospital for children, particularly leisure and entertainment services, or the inadequacy of non-medical services, for example, the food (already commented on). Thirteen citations were coded for this issue of lack or inadequacy of services (see Table 2). Improving health. Some children mentioned the issue of improving health, to feel better, as a positive aspect of the hospital. Four citations were coded in this topic (see Table 2). Negative aspects related to the disease and/or treatment. Some children mentioned issues related to the disease and/or treatment among the negative aspects of the hospital, besides the above-mentioned ones related to pain. But these issues were only mentioned by 3 children, and 5 citations were coded in this topic (see Table 2). Isolation and loneliness is another issue that the children mentioned as the worst part of their experience in the hospital. Four children expressly mentioned this topic, and 4 citations were coded in it (see Table 2). Other positive aspects. Four children also mentioned other positive aspects of the hospital, apart from those indicated above. Five citations were coded in this topic (see Table 2). Negative overall assessment of the hospital. Throughout the interviews, some children expressed globally negative views of the hospital. These negative evaluations were coded in 9 citations extracted from interviews with 8 children (see Table 2).

The best and the worst things about the hospital for children with cancer.
Examples of verbatim quotes, grouped by theme.

Discussion
The children involved in our study expressed a consistent view of the hospital. Their way of expressing themselves in this regard varied depending on their age, their cognitive development, and their social skills but, in general, with few exceptions, when given the opportunity, they could talk about aspects of the hospital that described an important part of their experience. The thematic analysis of these conversations has allowed us to identify the most significant aspects of the experience of the participating children with cancer in relation to the hospitalization process. We could speak of four interrelated dimensions particularly relevant to the hospitalization experience of the children with cancer interviewed (Figure 2). The first would refer to safety, care, and protection. Children emphasize the need to feel safe, cared for and protected in the hospital. They wish to be cured, to get well, and, above all, they do not want to experience pain, but in the hospital, they feel very threatened by painful experiences. The importance of pain as the most negative aspect of the hospitalization experience of children also stands out as particularly significant. And not only, or fundamentally, the pain derived from the disease, but that related to the medical procedures, in particular, the pain and the fear of pain produced by injections and needles. Painful procedures involving needle-stick or the like are very common in hospitals (8) and are a source of considerable suffering for the children. Evidence supports multiple techniques to reduce procedural pain (9) but their widespread implementation in hospitals is far from being achieved (10). The children interviewed in this work again mostly point to the pain of pokes and the like as the worst part of their experience in the hospital.
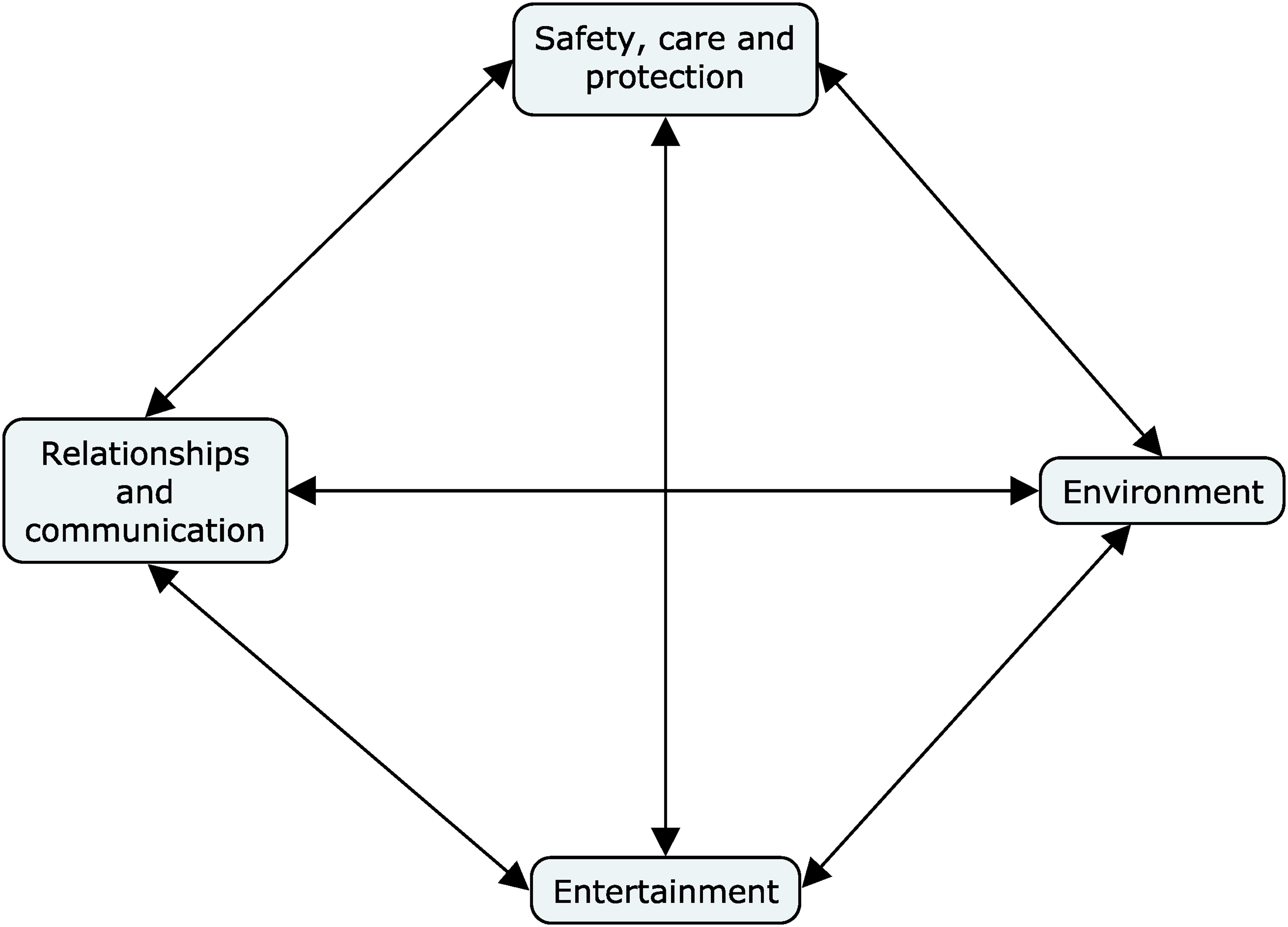
Relevant dimensions to the hospital experience of participating children with cancer.
The second dimension derived from the thematic analysis carried out has to do with aspects related to communication and the relationships of the children with the health personnel and with their family. In this sense, the children insisted on the importance for them of the treatment they received from the health personnel, particularly the nursing staff. Children highly value the care provided by the health workers. Their image of them, particularly of the nursing staff, and the role of the relationship of these staff members with the children and families in their well-being during hospitalization is one of the highlights of this work. The hospitalization experiences of children and adolescents (11) are greatly influenced by the relationships they establish with the health staff: when these relationships produce trust and participation, the children express greater satisfaction and feel better about the procedures and treatments. The evidence about this issue is extensive (11–14), and the children participating in our work expressed this in the same sense. The children interviewed also spoke of the importance of relationships with their families, with the members of their families who were with them in the hospital, but also with those who could not visit them during their admission, especially their siblings. They miss their siblings and friends, and online communication alternatives can help.
The third dimension derived from the thematic analysis has to do with the characteristics of the hospital environment. Some aspects of the hospital facilities are highly valued. Among them, the atmosphere of the corridors and rooms stands out. Regardless of age, the children mention it as one of the aspects of the hospital they liked the most. Visual arts can play an important role in the pediatric patient experience (15) because they can improve the symbolic quality of hospital environments and facilitate communication processes with children. The participating children considered the artistic interventions in the hospital, in the corridors and rooms, as positive elements that helped them feel better during their stay. In the section of the facilities, an issue that the children mentioned was the need to have wifi in all the rooms, both for their entertainment and to connect with their friends and their school.
Finally, the children valued aspects of the hospital that had nothing to do with medical issues, but rather with other services that the hospital provides for the children, especially school services and play and entertainment. The hospital school and the support of its teachers gives them a sense of normality and continuity with their daily lives and helps them to keep in touch and feel hopeful about their return to school after hospitalization. It has been found (16) that children attach great importance to the facilities and leisure activities in the hospital, which help them create a more positive hospitalization experience, combating boredom, improving their sense of control, and reducing the feeling of isolation.
The four dimensions noted above reinforce each other. For example, the characteristics of the environment can facilitate (or hinder) children’s communication and entertainment. In the same vein, positive communication with healthcare professionals can reinforce a child’s security, making him or her feel cared for and protected. Well-designed play and entertainment activities have the potential to promote positive relationships between patients and caregivers and reinforce children’s feelings of security.
In general terms, the children’s perspective was coherent with the scientific evidence on the humanization of pediatric hospitals (17). This raises the need for the design of health care in hospitals to take into account aspects in which the children of our study coincide with the researchers who have addressed these issues. We underline the decisive importance of communication with the child and their family; the control of pain and symptoms of distress; the environment should be designed to adapt to infantile users, that is, it should be a hospital “tailored to children”; children should be able to carry out activities to occupy their hospitalization time positively. In short, the design of hospital care should be oriented toward the child and the family, toward their needs and perspectives.
We acknowledge that the study has various limitations. First, all the participating children were admitted to the same hospital. For this reason, the generalizability of their views is limited. Even so, we believe that their observations may be useful to better understand the experience of pediatric oncology patients receiving treatment in other hospitals. As a second limitation, we note that the opinion of children with delays in neurocognitive development was not collected. The difficulty of doing this with the methodology used is evident, but so is the need to include these children’s points of view because oncological problems that affect the nervous system can lead to difficulties and delays in neurocognitive development.
From our point of view, the clinical implications of this study are important, as they point to relevant dimensions of care for children with cancer who are hospitalized as they experience it. From their perspective, children need to feel safe and protected in the hospital, that communication with them is taken care of as an essential part of their care, that the positive (or negative) impact that the characteristics of the physical environment of the hospital may have on their emotional state is considered, and last but not least, that during the hospitalization time, children’s entertainment is taken care of, that is, that they can develop playful and/or educational activities adapted to their age and health conditions in the hospital. Actively listening to children with cancer, as we have done in this work, allows us to promote their participation in the design of the health care they receive. This participation is a way to improve the quality of pediatric care and to fulfill the right of children to be involved in issues that affect their health.
Footnotes
Acknowledgements
We wish to express our thanks the children who collaborated with us by participating in the investigation.
Data Availability
Data available on request from the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Hospital Ethics Committee (ref.: R-0100/20).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Spanish Ministry of Science, Innovation and Universities (grant number PID2019-104506GB-I00).