
Abstract
Advances in diagnostics and therapeutics have improved prognosis for metastatic breast cancer (MBC). Yet, treatment and disease burden—including experiences of pain and nausea—present practical and emotional challenges. To better support patients and enhance quality of life, deeper understanding of the pathways linking physical and psychological health is needed. To this end, we examined associations of pain and nausea with depression and anxiety among women with MBC. In doing so, we highlighted social function as a potentially important mechanism in this relationship. This observational, cross-sectional study included 148 predominantly non-Hispanic White, highly educated women living with MBC. Multivariate regression models demonstrated that more intense pain and nausea were significantly associated with higher levels of depression and anxiety (p < .001). Causal mediation analyses confirmed significant indirect effects whereby decreases in social function associated with pain and nausea contributed to depression and anxiety. Thus, our findings illustrate decreased social function as one pathway through which pain and nausea contribute to escalation of depression and anxiety. Our results, therefore, underscore the importance of supporting social function among women with MBC to potentially reduce psychological sequelae of pain and nausea.
Introduction
Breast cancer is the most common form of cancer among women in the United States, with an estimated 281,550 new cases in 2021 (1). Of new cases, approximately 6% to 10% will initially be diagnosed as metastatic, and nearly 30% of those diagnosed with earlier-stage breast cancer will develop metastatic disease (2,3). Advances in drug development, treatments, and imaging techniques (4-7) have led to substantial increases in survival rate for metastatic breast cancer (MBC) patients since 1990 (8).
Nevertheless, the physical and emotional burden accompanying MBC can be substantial. Pain and nausea, in particular, are typical of the patient experience. Intense pain is commonly reported; and, pain is one of the most significant predictors of poor quality of life for this population (9-12). Additionally, due to the prevalence, impact, and undertreatment of pain in MBC patients (13), opioid usage is high (14). Limited research suggests that opioid-induced nausea also negatively impacts quality of life (10,11,15). Thus, in the face of intense pain and nausea, critical opportunities exist to maintain well-being and enhance quality of life (16-18).
Alleviating physical symptoms through effective palliative and supportive care has been shown to improve patients’ quality of life (19,20). One potential avenue for such intervention is maintenance of social function. Indeed, among patients with MBC, social interactions, activities, and relationships are linked to improved clinical outcomes and lower levels of distress (21,22). At the same time, patients express concerns over their ability to maintain social roles during the course of their illness (23,24). Thus, while experiencing pain and nausea may hinder participation in social roles and activities, supporting social function in light of such physical symptoms might help improve psychological health.
In this spirit, the purpose of this study is to evaluate associations of pain and nausea with depression and anxiety in MBC patients and add to the current understanding by examining a potentially important mechanism—ability to participate in social roles and activities. Specifically, we dive deeper into the relationship between physical symptoms and psychological well-being by examining the degree to which diminished social function accounts for (ie, mediates) these associations.
By conceptualizing social function as a mechanism, we provide a more comprehensive illustration of the dynamic pathways linking pain and nausea with psychological health. In doing so, we offer insight into the importance of promoting social function among women with MBC.
Methods
In 2018, Cancer Support Community (CSC) developed an online survey to characterize experiences of MBC patients with pain and nausea. Participants were recruited through CSC's Cancer Experience Registry, online networks, CSC’s network partners, including Cancer Support Community and Gilda’s Club partners, and advocacy partners. Ethical and Independent Review Services (E&I) served as the Institutional Review Board of record (Protocol #18145-01). Study procedures were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Participants provided electronic informed consent prior to participation.
Sample
From October 2018 to March 2020, 161 MBC patients provided informed consent to participate in this study. We limited the analytical sample to the 148 respondents who answered questions on key independent variables (psychological well-being, pain and nausea, and ability to participate in social roles).
Measures
Psychological well-being
Participants completed the Patient-Reported Outcomes Measurement Information System 29 Profile V2.0 (PROMIS-29) (25). PROMIS-29 consists of a series of 4-item subscales where patients rate their physical and mental well-being over the past 7 days. Responses are measured on a 5-point Likert-type scales, summed to create raw subscale scores, and transformed into T-scores. T-scores are standardized with a mean of 50 and standard deviation of 10, with a normative reference group of the US general population. Each PROMIS-29 subscale has shown to be reliable, with Cronbach's α ranging from 0.87 to 0.96.
For this study, two dependent variables captured psychological well-being. One series of analyses predicted T-scores for the PROMIS-29 depression subscale and a second set of analyses predicted T-scores for the anxiety subscale.
Pain and nausea intensity
As part of PROMIS-29, participants answered a single item on pain intensity. Specifically, participants rated their average pain in the last 7 days on a scale from 0 to 10 (10 being the most significant). A nausea intensity item was developed for this study, mirroring the PROMIS-29 pain item. Participants rated their average nausea in the past 7 days on a scale from 0 to 10 (10 being the most significant).
Social function
PROMIS-29 includes a subscale evaluating ability to participate in social roles and activities. Participants respond to the frequency with which they had trouble doing leisure activities, family activities, work, and activities with friends over the past 7 days. T-scores were calculated and used in multivariate analyses. Higher scores represent greater social functioning.
Sociodemographic background and clinical history
Participants provided information on birth year, race, ethnicity, education, employment status, household income, sexual orientation, marital status, and geographic region. Participants self-reported general health (1 = excellent to 5 = poor), year diagnosed, stage diagnosed, remission status, and number of recurrences. Finally, participants indicated whether they have ever had surgery, and whether they have undergone or are currently undergoing chemotherapy, radiation therapy, hormonal therapy, oral therapy, and immunotherapy.
Analyses
Descriptive statistics
We calculated descriptive statistics for independent, dependent, and mediating variables, as well as sociodemographic background and clinical history variables. To facilitate ease of interpretation, social function, depression, and anxiety subscales were collapsed into dichotomous variables (0 = Not at all or A little bit; 1 = Somewhat, Quite a bit, or Very much) and the percentage of participants in each category were calculated; in inferential analyses, continuous T-scores were used.
Multivariate analyses
The primary goal of this study was to test social function as a mechanism through which pain and nausea are associated with psychological well-being. To accomplish this goal, multivariate analyses were performed in three steps.
First, we confirmed associations between pain and nausea and psychological well-being in a regression framework. Second, we introduced social function to the regression models, considering the degree to which the associations were attenuated. The third, and focal, step was causal mediation analysis (26-29), which describes how an independent variable (pain/nausea) affects an outcome (psychological well-being) through a mechanistic variable (social function) by decomposing the total effect into direct and indirect effects.
Analyses were performed in R 4.0.5 (30) using RStudio.
Results
Descriptive Statistics
The analytical sample was entirely female, predominantly non-Hispanic White (89%), and highly educated (68% with a Bachelor's degree or higher). 62% of respondents were married at time of survey. The average age was 57.7 years (range: 26 to 81). Nearly two-thirds (63%) reported good, very good, or excellent health. Two-fifths (41%) indicated that they were originally diagnosed with metastatic disease, and nearly all (90%) were actively undergoing some form of treatment for their cancer at time of survey.
Age at diagnosis, general health, initial metastatic diagnosis, marital status, and current treatment status were hypothesized to be confounding variables for regression analyses. Bivariate correlations confirmed that age at diagnosis and general health were significantly associated with psychological outcomes. As such, these measures were included as controls in multivariate analyses. Notably, marital status was not significantly correlated with depression and anxiety among our sample, and ANOVA tests showed no significant differences in social function across marital statuses.
As shown in Table 1, participants reported low to moderate pain intensity (mean = 3.92; SD = 2.82) and nausea intensity (mean = 1.82, SD = 2.58), with significantly higher mean pain ratings compared to nausea ratings (t = 6.66, p < 0.001). Nausea and pain intensity were significantly correlated, with participants who reported higher pain being more likely to report higher intensity of nausea (t = 6.84, p < .001).
Descriptive Statistics for Pain, Nausea, Depression, Anxiety, and Social Function.
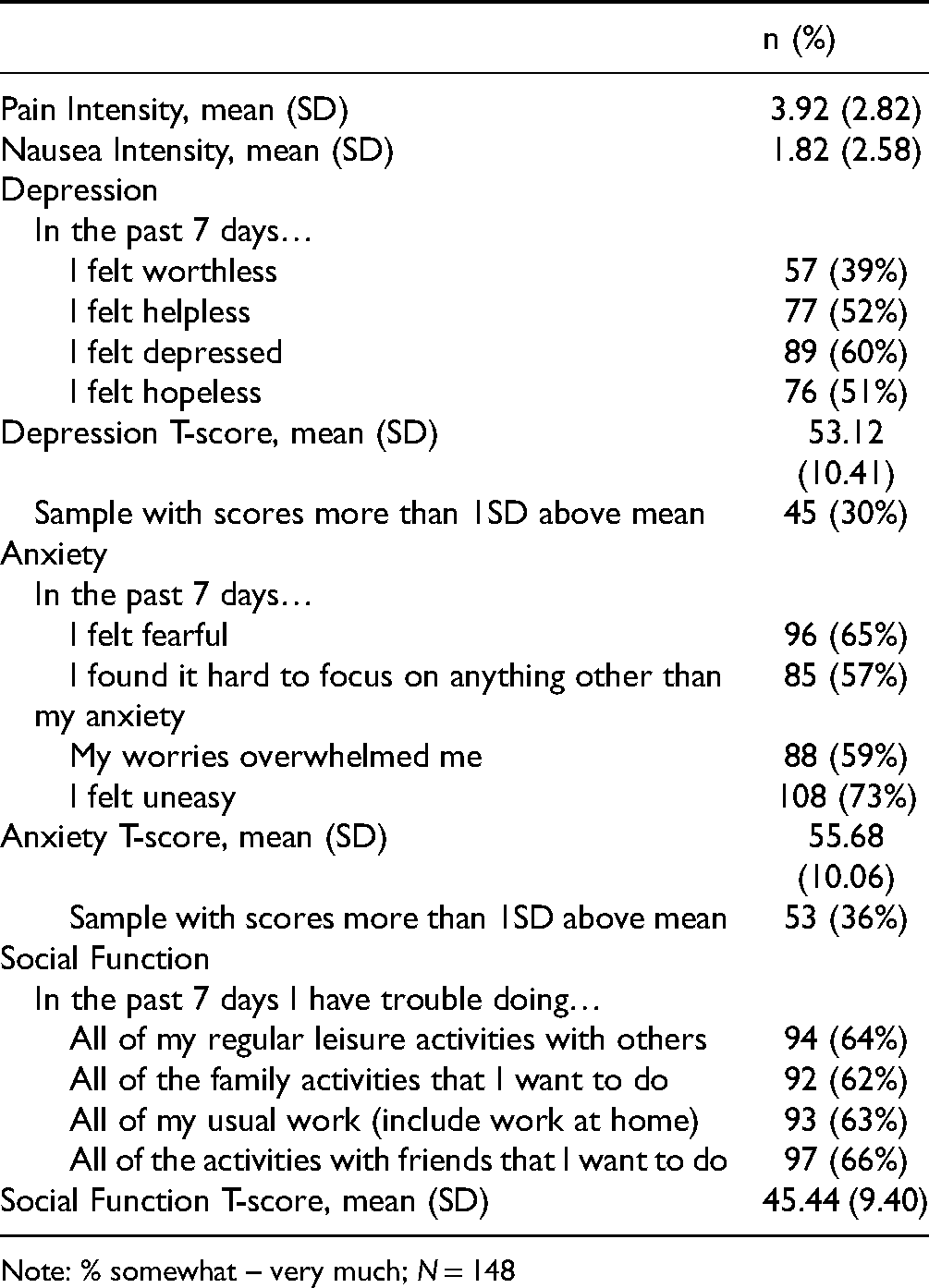
Note: % somewhat – very much; N = 148
Responses to PROMIS-29 subscales for depression and anxiety suggested variability in participants’ psychological well-being (Table 1). Depression items were somewhat to very much endorsed by 39% to 60% of participants, and anxiety items were somewhat to very much endorsed by 57% to 73% of participants. T-score calculations allowed for comparison to national averages, highlighting that 30% and 36% of respondents scored at least one standard deviation above the mean for depression and anxiety, respectively.
For social function, about two-thirds of participants consistently reported having somewhat to very much trouble engaging in social roles and activities.
Pain and Nausea Intensity and Psychological Well-Being
To test social function as a mechanism through which pain and nausea are associated with psychological well-being, a necessary first step was to confirm direct pathways. Table 2 presents results predicting depression T-scores. Model 1 confirms a significant, positive association between pain intensity and depression (b = 1.289; p < .001), whereby higher self-rated pain was associated with more severe depressive symptoms. Similarly, Model 2 confirms a significant, positive association between nausea intensity and depression (b = 1.438; p < .001).
Multivariate Regression Models Predicting PROMIS Depression T-Score.

Note: N = 148; * p < .05, *** p < .001
Table 3 includes results for anxiety. Models 1 and 2 show significant, positive associations between pain intensity (b = 1.311; p < .001) and nausea intensity (b = 1.360; p < .001) with anxiety. The more severely participants reported their pain and nausea, the higher their anxiety T-score. In this way, results are consistent with previously documented associations and confirm that more intense pain and nausea were associated with poorer psychological well-being in our sample.
Multivariate Regression Models Predicting PROMIS Anxiety T-Score.
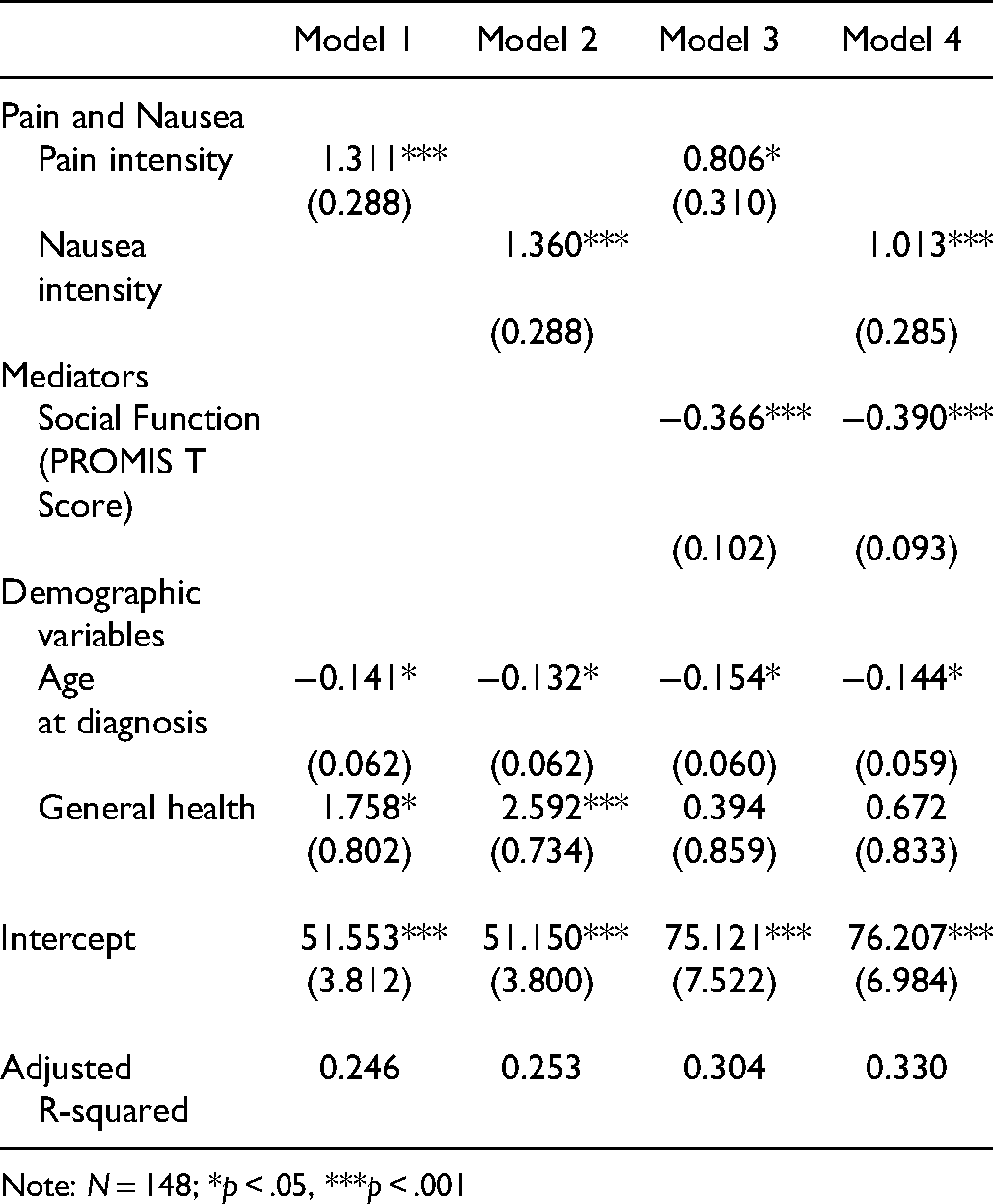
Note: N = 148; *p < .05, ***p < .001
Physical Symptoms, Social Function, and Psychological Well-Being
Building on Models 1 and 2, our second analytical step was to test for attenuation of the direct associations when introducing social function. Models 3 and 4 in Table 2 include those analyses for depression, while Models 3 and 4 in Table 3 include those analyses for anxiety.
In Table 2, social function is significantly, negatively associated with depression T-score (b = −0.443 and b = −0.445 in Models 3 and 4; p < .001). Thus, the better a participant's social function was, the lower their depressive symptomatology. Additionally, the association between pain intensity and depression appears to be attenuated in Model 3 of Table 2 (b = 0.677 and p < .05, compared with b = 1.289 and p < .001 in Model 1). The association between nausea intensity and depressive symptoms remains strongly significant (b = 1.043; p < .001) in Model 4 (compared with b = 1.438 and p < .001 in Model 2).
In Table 3, social function was also significantly, negatively associated with anxiety T-score (b = −0.366; p < .001). Hence, better social function was linked to decreased anxiety. While the association between pain intensity and anxiety appears to be slightly attenuated (b = 0.806 and p < .05 in Model 3, compared with b = 1.311 and p < .001 in Model 1), the association between nausea intensity and anxiety was significant at p < .001 in Model 2 (b = 1.360) and Model 4 (b = 1.013).
Overall, we confirm that better social function was associated with more positive psychological well-being. Moreover, social function appeared to partially explain the relationship between pain intensity and psychological outcomes.
Causal Mediation Analysis
Our final step was estimating causal mediation models to better understand direct and indirect pathways linking pain and nausea, social function, and psychological well-being (Table 4). The total effect, which describes the strength of the association of pain and nausea with psychological well-being, is decomposed into an indirect path (ACME) and direct path (ADE). ACME reports the degree to which the total association channels through social function (26-29). The proportion mediated is reported, as is the regression coefficient for social function on pain/nausea, informing directionality of associations.
Causal Mediation Analysis Testing Mediation by Social Function.
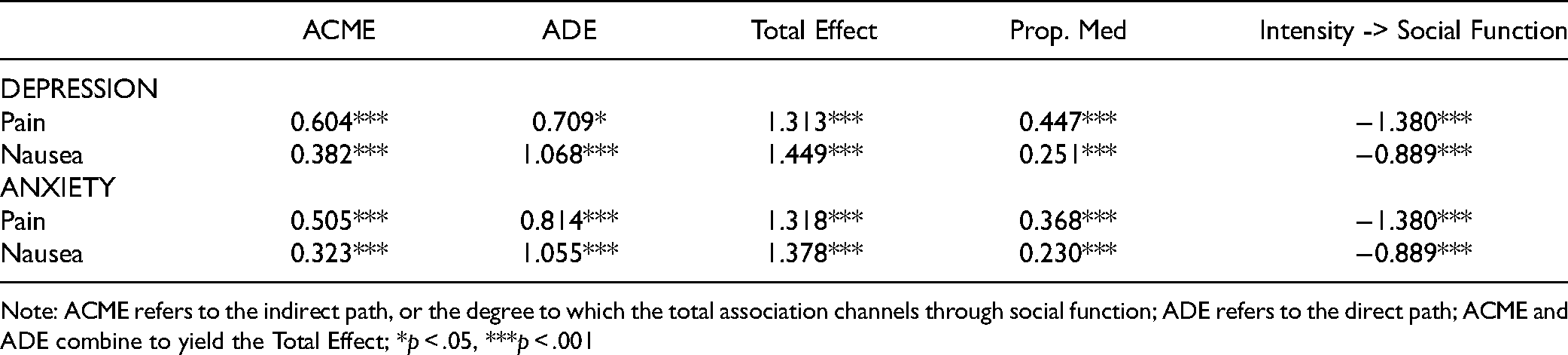
Note: ACME refers to the indirect path, or the degree to which the total association channels through social function; ADE refers to the direct path; ACME and ADE combine to yield the Total Effect; *p < .05, ***p < .001
For depression and anxiety, social function significantly mediated the association between pain and nausea and psychological well-being. Specifically, intense pain and nausea reduced social function, which, in turn, decreased psychological health. This indirect path held statistical significance for all models considered—those with pain intensity as the predictor, nausea intensity as the predictor, depression as the outcome, and anxiety as the outcome (ACME p < .001). Despite the consistency of social function as a mediator, however, nuances across models warrant mentioning.
First, nearly half of the total effect between pain intensity and depression was explained by social function (proportion mediated = 0.447). Pain limited social function, thereby amplifying depressive symptomatology.
At the same time, the direct effect accounted for the vast majority of the total effect across the other models, indicating that social function only partially mediates the associations considered (proportion mediated ranging from 25% to 37%). In other words, pain and nausea limited social function; and, though this limitation mattered for psychological well-being, the direct linkages from pain and nausea to depression and anxiety were robust.
Overall, our analyses confirmed direct associations between pain and nausea intensity and psychological well-being. The pain and nausea reported by women with MBC increased their risk of depression and anxiety. Further, we documented a meaningful mechanism for these associations—social function. The decrease in social function associated with pain and nausea contributed to the impact of pain and nausea on psychological well-being. This mediation was particularly relevant for the relationship between pain and depression.
Discussion
Over the past few decades, advances in drug development, treatments, and imaging have led to a reduction in mortality rates for MBC (4-8). However, even with the focus on (16-18)–and proven efficacy of (19,20)–palliative care interventions, pain and nausea remain chronic problems with clinically meaningful implications for depression and anxiety (31-35). As such, we explored the relationship between pain and nausea intensity and psychological well-being among women with MBC, highlighting the role of social function. We hypothesized that pain and nausea would decrease ability to participate in social roles and activities, thereby hindering psychological well-being.
Consistent with existing literature (31-35), we documented significant associations between pain and nausea intensity and anxiety and depression. Extending previous findings, we also found support for social function as a mechanism that partially explained these relationships.
Our focus on social function points to a practical avenue for intervention and supportive care. Our results suggest that supporting patients in their efforts to maintain social engagement and meaningful relationships—which may be accomplished, for example, through effective screening for social needs or connection to support group services through healthcare settings as well as advocacy and non-profit support organizations—might reduce the detrimental impact of pain and nausea on psychological well-being. Social outcomes are a priority for women with MBC, and factor, more generally, into patient experiences (21-24). Interestingly, beyond the focal associations presented, social function also mediated linkages between general self-reported health and psychological outcomes among our analytical sample (Models 3 and 4 of Tables 3 and 4), pointing to multidimensional processes whereby social function contributes to patient experiences. Social outcomes should thus be considered critically important not only for patient experience research, but also more practically in the clinical development pipeline and during treatment decision-making.
We found social function to be particularly salient in explaining the relationship between pain and depression. The impediment of nausea on psychological well-being was less attenuated by maintenance of social function. A more detailed examination of mechanisms linking nausea and distress, therefore, would allow for better understanding of how to address downstream effects of nausea, particularly for individuals who routinely experience nausea in their current course of treatment.
Despite evidence for social function mediating the implications of physical symptoms on psychological well-being, our results consistently illustrated the ever-important direct associations. Undoubtedly, pain and nausea are powerful predictors of depression and anxiety among MBC patients. Future research should thus extend conceptualization of interceding factors to support patients as they grapple with the physical sequalae of metastatic disease. Additionally, discussions with care providers should emphasize the psychosocial effects of pain and nausea.
Our study has limitations. Data collected from participants were self-reported. Given the complexity of clinical questions and the subjectivity inherent in self-reporting psychosocial data, some of the data may not be fully accurate. Additionally, our sample size was relatively small and largely comprised of well-educated, White women. Expanding the sample by inclusion of underserved groups would improve study generalizability. These results should be substantiated in underrepresented groups before drawing conclusions, as past research has clearly documented racial biases in the perception of others’ pain (36,37). Likewise, though educational attainment was accounted for in multivariate analyses, patient knowledge and education on disease process—that can influence sense of preparedness and perceived sense of control, which in turn are related to psychological outcomes (38)—was not; and, future work highlighting the role of patient education in the pathways we considered would provide more information on potential intervention. Finally, social function and psychological well-being are reciprocally linked, and we are limited by the use of cross-sectional data. Longitudinal data would allow for a more nuanced conceptualization of the dynamic ways that social function and psychological well-being relate.
Conclusion
In conclusion, supporting social function may alleviate some of the psychological burden associated with experiences of pain and nausea among women with MBC. Social function should be considered an important part of the patient experience. Still, the physical-to-psychological link remains even when social function is considered, suggesting that future work should continue to study mechanistic pathways that might lend themselves to intervention and support.
Footnotes
Disclosures and Acknowledgements
The authors thank Alyssa Jaisle and Kelly Clark as well as the Cancer Support Community and Gilda’s Club network partners and advocacy partners for support in the recruitment of participants for this study.
Authors report institutional grant from Charleston Laboratories during the conduct of the study. Dr Zaleta: Institutional research funding from: Astellas Pharma, Gilead Sciences, Novartis, Pfizer Oncology, Seattle Genetics. Dr Fortune: Institutional research funding from: AbbVie, Amgen Oncology, AstraZeneca, Astellas Pharma, Bristol Myers Squibb, Genentech, Gilead Sciences, Lilly Oncology, Merck & Co, Inc, Sumitomo Dainippon Pharma Co, Takeda Oncology.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article