
Abstract
The COVID-19 pandemic has resulted in a widespread move towards virtual consultations within secondary care due to infection concerns. This service evaluation undertaken in a Welsh Interstitial Lung Disease (ILD) specialist center looks at the experiences of unselected ILD patients and their careers with telephone consultations and aims to identify the role of telephone consultations in future practice for this patient group. A mixed methods approach was used with an initial postal questionnaire followed by a virtual focus group. From the 84 patient and 26 carer questionnaire responses, there was broad support for telephone consultations from both groups. The main perceived benefit was reduced infection risk, although face-to-face consultations were seen as holding more value. Themes identified in the virtual focus group of 6 participants recognized the need to balance quality of care against practical considerations. In conclusion, there was support for future telephone consultations if patients and clinicians have flexibility in determining when this occurs, instead of a face-to-face consultation.
Introduction
Interstitial lung diseases (ILD) are a heterogeneous group of respiratory and multisystem diseases including, but not limited to, conditions such as idiopathic interstitial pneumonia (including idiopathic pulmonary fibrosis), connective tissue disease-related ILD, sarcoidosis, and hypersensitivity pneumonitis (1). The COVID-19 pandemic has led to major changes in outpatient service delivery to ILD patients and challenged clinicians to find new solutions to facilitate their ongoing care. One major change is the recommendation to move outpatient consultations from the face-to-face clinic setting to virtual consultations (2).
Prior to the COVID-19 pandemic, there has been limited evaluation of the impact of telephone consultations in respiratory medicine. A 2007 observational study by Roberts et al of 500 respiratory patients who had follow-up by telephone instead of face-to-face noted that the mean length of consultation was reduced from 15 to 9 min, and that there was no significant difference between patient satisfaction scores for telephone and face to face consultations. However, this was a carefully selected patient group with patients deemed to need examination or investigations being excluded, along with patients who opted to have face-to-face consultation instead. In addition, this study did not look at the impact on carers (3). A 2020 patient survey by Vijayakumar et al looked at satisfaction with an initial telephone consultation as part of a 2-week wait lung cancer pathway, prior to the COVID-19 pandemic. The 111 patients surveyed reported high levels of satisfaction, although the authors concluded that frail or comorbid patients may benefit from a face-to-face review and patients should also be offered the choice of a face-to-face consultation if they preferred. This survey only evaluated satisfaction with a first contact appointment, not with further follow-up appointments, and did not evaluate the impact on carers (4).
Since the beginning of the COVID-19 pandemic, there have been many publications on telephone consultations across a range of different specialties and services. A single center prospective study in a National Health Service district general hospital by Vusirikala et al evaluated the satisfaction of both patients and clinicians with secondary care orthopedic telephone consultations implemented as a result of the pandemic. Among the 100 patients and 25 clinicians surveyed, overall satisfaction levels were high and there was support for the ongoing use of telephone consultations post-pandemic. They assessed factors contributing to patient satisfaction, including reduced inconvenience and personal cost. However, the impact on carers was not assessed (5). To date, there has been nothing published specifically on the experiences of patients with ILD and their carers, and no reports on qualitative data were obtained from patient focus groups. This study describes the experiences of ILD patients and their carers with telephone consultations and aims to identify if there is any role for these in the longer term.
Method
Patients within the Cardiff and Vale Interstitial Lung Disease (ILD) service contacted for a telephone appointment between April and May 2020 were invited to take part in a postal questionnaire, with a separate questionnaire to be filled in by their carer (any unpaid individual identified by the patient as providing physical or emotional support to them, eg, spouse or family member). Patients were also sent written information on the virtual focus group which was to be undertaken using a group video call on a virtual platform. Those indicating interest in this were then contacted by telephone to confirm availability and access to appropriate technology. The virtual focus group was undertaken using a semistructured style, recorded and transcribed verbatim. The Framework Method (an analysis methodology that is commonly used in managing qualitative data in health research) (6) was then used to identify themes from the transcripts. Formal ethics approval was not required as the design was a service evaluation rather than a research study.
For the purposes of analysis, the patients were separated into the following categories: mild stable, mild progressive, severe stable, and severe progressive. The criteria used for classification are described in Table 1, with each patient being classified according to one category on the top row of the table (ie, mild or severe) and one category on the bottom row of the table (ie, stable or progressive).
Criteria Used for Classification of Patients.

Previous publications, such as the CaNoPy (The care needs of patients with idiopathic pulmonary fibrosis and their carers) study by Sampson et al (7), have divided ILD patients into categories depending on their lung function results. However, this was not possible for this cohort of patients as the majority of patients were not able to have up-to-date routine lung function performed at the time of evaluation due to restrictions advised by the ARTP (Association for Respiratory Technology and Physiology) (8). The criteria were therefore selected based on data that would be available on clinic letters and the patients’ electronic records.
Results
There were 193 telephone consultations conducted during the period April to May 2020, of which 23 were excluded (15 were general respiratory rather than ILD patients, 1 was a duplicate appointment, 3 appointments were canceled, and 4 patients died between the time of the appointment and the questionnaire being sent), leaving 170 patients in total to contact. Of the 170 patients contacted, 84 patient questionnaires were received (49.4% return rate) of which 26 patients also returned a carer questionnaire (31%).
Patient Questionnaire
The average age of the respondents was 71.6 years (38-91) with 57.1% being male and 42.9% being female. The patients were divided into the following disease categories (Table 1): mild stable 72 (85.7%), mild progressive 7 (8.3%), severe stable 5 (6%), and severe progressive 0 (0%).
Overall satisfaction with the telephone consultation was 7.8 out of 10, although there was some variation between the patient groups. Those patients with mild disease (mild stable 7.8 and mild progressive 8) were more satisfied than those with severe disease (severe stable 7), although this was not statistically significant.
When asked to select the benefits of telephone consultations, reduced infection risk was most commonly reported (89.3%). Other benefits included less time/waiting (69%), less travel (66.7%), less tiring (44%), and less cost, for example, travel and time off work (32.1%, see Figure 1). There was some variation between the patient categories with the benefits of reduced travel, reduced time taken, and less tiring being more frequently recognized by the mild progressive (100%, 100%, and 100%) and severe stable groups (80%, 100%, and 60%).

Benefits and drawbacks of telephone consultations (patients and carers).
When asked to select the drawbacks of their telephone consultations, the inability to have tests done was most commonly reported (84.5%). Other drawbacks included a preference for meeting face to face (60.7%), carers and family feeling less involved (17.9%), communication problems, for example, hearing impairment or need for translator (15.5%), and technology problems, for example, bad phone connection (14.3%). There was some variation between the patient categories with the mild progressive group showing greater concern that their carer felt less involved (42.9% compared to 17.9%). The severe stable group also reported more communication problems (60% compared to 15.5%).
When asked to rate the importance of the following factors in relation to their future appointments on a scale of 1 to 10, the patients responded as follows. The ability to have tests done (8.8), seeing someone face to face (8.4), risk of infection (8), time taken for appointment (5.6), and travel considerations (5.3) (see Figure 2). The ranking of factors was similar across all patient groups although there were some variations. Patients in the severe stable group were more concerned about the time taken for appointments (7.8) than those in the mild stable (5.3) and mild progressive (6.5) groups. Patients in the mild progressive group also appeared more concerned about infection risk (9.5) than those in the mild stable (7.9) and severe stable (7.2) groups.
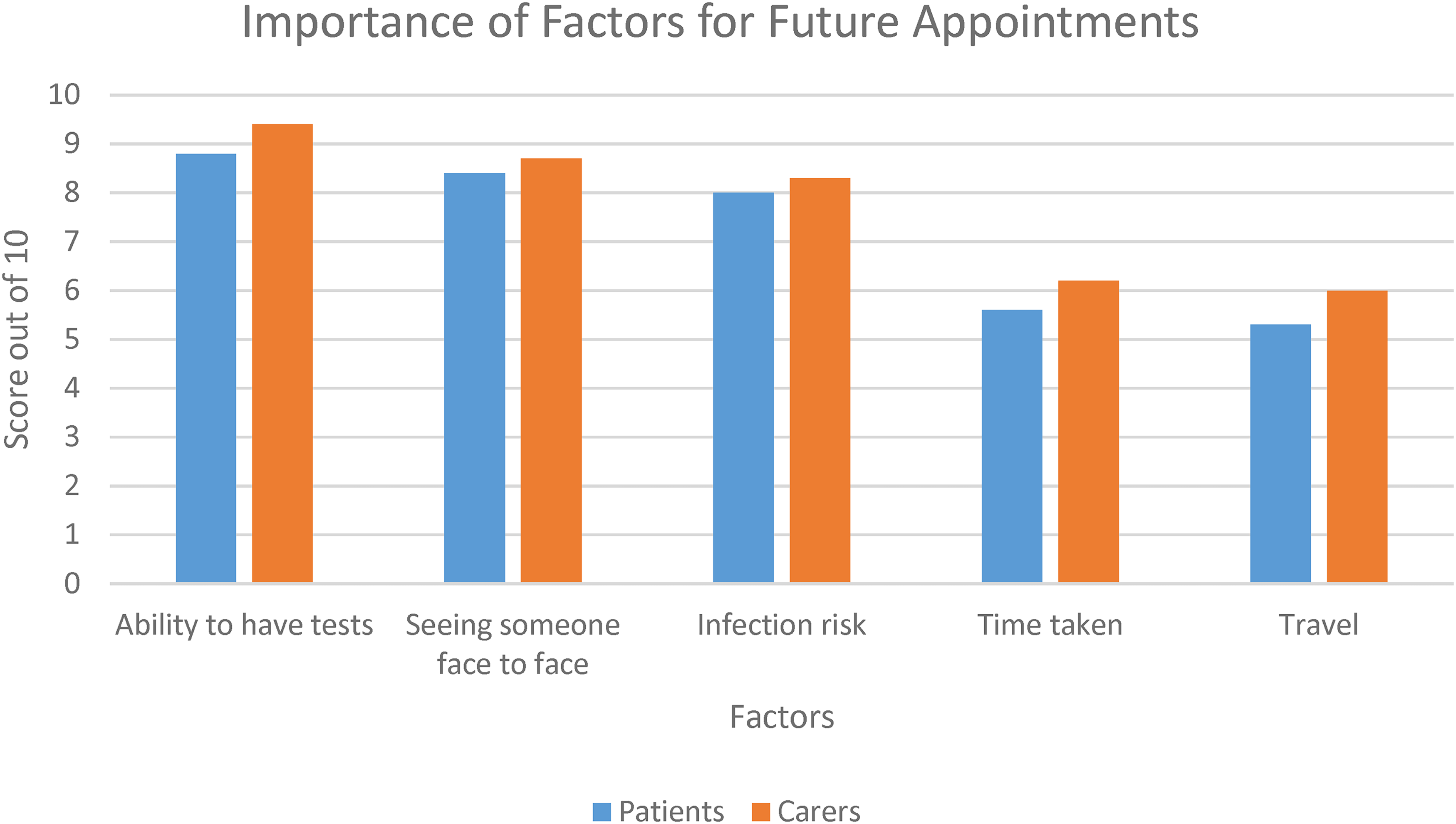
Importance of factors for future appointments (patients and carers).
When asked to score how able they felt to ask questions during their consultation, patients gave an average score of 8.3 out of 10.
When asked if they would be happy to have a telephone consultation in the future, patients mostly indicated that they would, provided that there was an option to arrange a face-to-face review if either they (69%) or their clinician (76.2%) felt they needed one. 27.4% indicated that they would be happy for all future consultations to be via telephone, while 9.5% indicated that they would prefer not to have telephone consultations at all in the future.
Carer Questionnaire
Of the 26 respondents, 80.8% were female and 19.2% male. The patients these individuals cared for were from the following disease categories: mild stable 19 (73.1%), mild progressive 6 (23.1%), severe stable 1 (3.8%), and severe progressive 0 (0%).
Overall satisfaction with their telephone consultation was 7.6 out of 10. Those from the Mild Progressive group (6.8) were less satisfied than those from the mild stable (7.8) and severe stable (8) groups.
The benefits of their telephone consultation were ranked in a similar fashion to the patient responses. Reduced infection risk (92.3%), less travel (76.9%), less time/waiting (61.5%), less tiring (46.2%), and less cost, for example, travel and time off work (26.9%).
The drawbacks of their telephone consultation were also ranked in a similar fashion to the patient responses. Unable to have tests done (76.9%), preference for meeting face to face (50%), feeling less involved in the consultation (38.5%), communication problems, for example, hearing impairment, need for translator (11.5%), and technology problems, for example, bad phone connection (3.8%). Compared to the patients, carers reported more frequently that they felt less involved in the consultations (38.5% compared to 17.9%). This was particularly true for carers of mild progressive (100%) and severe stable (100%) patients, compared to those of mild stable (15.8%) patients.
Carers ranked the importance of the following factors with regard to future appointments in the same order as patients (on a scale of 1 to 10). The ability to have tests done (9.4), risk of infection (8.7), seeing someone face to face (8.3), time taken for appointment (6.2), and travel considerations (6.0).
When asked to score how able they felt to ask questions during their consultation, carers gave an average score of 8.1 out of 10.
When asked if they would be happy to have a telephone consultation in the future, carers responded in a similar fashion to patients. They mostly indicated that they would, provided that there was an option to arrange a face-to-face review if either they (30.8%) or their clinician (76.9%) felt they needed one. 26.9% indicated that they would be happy for all future consultations to be via telephone, while only 3.8% indicated that they would prefer not to have telephone consultations at all in the future.
Virtual Focus Group
Of the 32 patients indicating an interest in participating in the virtual focus group, the first 8 patients who responded to a follow-up phone call and confirmed availability and technological ability to partake were invited to attend the focus group. Of these, 5 patients attended on the day, with 1 carer also participating.
The group was younger (average age 63.4) than the questionnaire group (average age 71.6) and had a higher proportion of female participants (50% compared to 42.9%). The themes identified were divided into 2 subheadings—Quality of Care and Practicalities (see Table 2).
Themes Identified in the Virtual Patient Focus Group.

Quality of Care
The need to be understood clearly was a common theme “we’ve all got our own individual issues and sometimes that gets lost on a telephone call,” “communication over the telephone is not as good as it is face to face,” and there was concern that the quality of their care was being diminished “I think it could be quite dangerous, we could miss out on diagnosis.” The fact that having investigations done was a source of reassurance was also a frequent comment “she doesn’t get those tests as well, so it means her mind isn’t at rest,” “up to date x-rays and some up to date breathing tests would give you peace of mind.” The importance of patient choice was also highlighted “I think the option is the important thing. If you have a telephone appointment and you have concerns I think the option of follow up face to face really needs to be available,” “the patient needs to be asked what they want.”
Practicalities
Patients demonstrated that they were aware the context of the COVID pandemic made changes in practice necessary “I think it's (telephone consultations) the norm because of the circumstances…nobody wants to get COVID,” “it makes sense not going back and forward to the hospital,” and recognized some of the practical benefits of telephone consultations “it sometimes helps just once in a while for travelling and also parking,” “the stress of not having to go to (hospital) is quite nice.” They also showed pragmatism, recognizing that if their condition was stable they would be more content “I’ve been quite well throughout the summer so I haven’t worried about it as much as someone else might,” and also recognized some of the technological problems related specifically to video consultations “there's quite significant IT issues related to video consultations.”
Overall, all participants of the focus group understood the need to balance quality of care against practicalities. The predominant sentiment was that of telephone consultations being inferior to face-to-face interaction but also understanding that the current pandemic and associated restrictions have made telephone appointments a necessity. Many reported that having regular investigations (lung function and radiology) provided them with reassurance, and there was a concern around missing a diagnosis or deterioration if these were not available. There was some acknowledgment of the benefits of not needing to come for a face-to-face appointment, but overall the participants reported that having a degree of choice and being able to arrange a face-to-face appointment if needed (accepting the associated risks) would be preferable.
Discussion
Among the surveyed ILD patients and their carers, telephone consultations were broadly viewed as acceptable in the context of the covid-19 pandemic, with reasonable satisfaction rates. The main benefit perceived was that of reduced infection risk, but patients and carers in the mild progressive and severe stable categories also particularly noticed the benefit of reduced travel and time taken, along with reduced tiredness. However, there was concern from both patients and carers around not having testing to monitor their condition objectively, and face-to-face consultations were felt to hold more value. Patients and their carers showed support for future telephone consultations provided there was a degree of flexibility and choice to opt for a face-to-face consultation if needed.
These sentiments were echoed in the virtual patient focus group. The need to balance quality of care against the context of practical factors dictated by the COVID pandemic was very clear. The importance of patient choice in dictating ongoing follow-up plans was also echoed.
There are similarities with the results from Vusirikala et al's study of orthopedic patients in the COVID era. They also expressed satisfaction with telephone consultations, recognizing the benefits of reduced infection risk and convenience, while also recognizing that some patients have more confidence in face-to-face consultations. Although our patient cohorts are very different, the similarities in the findings suggest that our results may be applicable to many different patient groups.
There are several options available to address patient concerns around the lack of access to tests. Community blood testing has been available to our patients throughout the pandemic, and this has been utilized by patients requiring monitoring blood for treatments such as antifibrotic or immunosuppressive therapies. Prior to the pandemic, our service ran as a “one stop shop” with chest radiograph and spirometry being performed on the same visit as the clinician consultation. In order to reduce footfall, we have arranged separate appointments for lung function and radiology prior to the telephone consultation, where these investigations were deemed to have a material impact on the patient's care. The development of home spirometry technology also offers patients the ability to monitor their condition without needing to attend hospital (9).
One strength of this service evaluation is the mixed methods approach. This allows the benefits of both quantitative and qualitative data and allows us to corroborate the results, with the addition of the focus group giving further detail and elaboration on the initial findings from the questionnaires. The patients being from an unselected ILD group reflects real-life practice and service organization, rather than representing a single disease. Limitations include the fact that this is a single center evaluation, at a particular point in time, and therefore, may not be relevant to other services in other locations. The spread of respondents across the disease categories was not even, with the mild stable patients and carers being the dominant group. However, this was reflective of the patient population within the service. The participants in the virtual focus group were a self-selecting group of participants, reflecting our most engaged and technologically capable patients, and therefore, may not be representative of the whole cohort.
Patients were offered telephone consultations rather than video due to the age of our population and the concern that levels of familiarity with the technology would be low. Gilbert et al also recognized some of the issues around video consultations with patients reporting lower satisfaction with them compared to telephone consultations (44% compared to 94%), in the context of orthopedic outpatient clinics. Participants reported low confidence in using the technology, along with equipment and software issues (10). However, as familiarity with the technology improves, the support for video consultations over telephone may increase.
This picture represents opinion at a particular point in time. These patients and carers had undertaken their telephone consultation during the first few months of the pandemic, and the questionnaire was sent out in the autumn of 2020, at a time when shielding advice was in place and the timelines for vaccine availability were unclear. As concern over infection risk goes down (eg, with mass vaccination and reducing community prevalence), it is likely that factors other than infection risk will influence opinion more. It would, therefore, be useful to repeat this evaluation outside of the context of the covid-19 pandemic. Although the reduced time for appointments and travel considerations were seen as benefits in this evaluation, this was to a lesser degree than the draws of face-to-face contact and having tests performed.
Conclusion
There was broad support for telephone consultations among ILD patients and their carers, with the main benefit being perceived as a reduced infection risk. Although face-to-face consultations were generally preferable, there was support for future telephone consultations provided that patient choice was taken into consideration. This was particularly the case for patients who may find attending outpatient settings more onerous.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221133638 - Supplemental material for Telephone Clinics During the Covid-19 Pandemic—The Experiences of Interstitial Lung Disease Patients and Their Carers
Supplemental material, sj-docx-1-jpx-10.1177_23743735221133638 for Telephone Clinics During the Covid-19 Pandemic—The Experiences of Interstitial Lung Disease Patients and Their Carers by Mia Gillett and Ben Hope-Gill in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735221133638 - Supplemental material for Telephone Clinics During the Covid-19 Pandemic—The Experiences of Interstitial Lung Disease Patients and Their Carers
Supplemental material, sj-docx-2-jpx-10.1177_23743735221133638 for Telephone Clinics During the Covid-19 Pandemic—The Experiences of Interstitial Lung Disease Patients and Their Carers by Mia Gillett and Ben Hope-Gill in Journal of Patient Experience
Footnotes
Authors’ Note
BHG conceived of the idea. MG undertook the literature search, method design, data collection, and analysis. MG wrote the first draft of the manuscript with input from BHG to finalize the manuscript. Data are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.