
Abstract
Introduction
According to the World Health Organization (WHO), prenatal care is one of the necessary services for women and one of the key indicators of the third sustainable development goals. Prenatal care providers play the key role in maintaining the health of mothers and infants (1); since during pregnancy, while mothers pay attention to her health and fetus (2). Moreover, a competent prenatal care provider may be a reliable support for women during pregnancy (3).
An investigation has revealed that health care recipients consider different criteria for selecting health care providers, which indicated providers should be competent (4). Competence has various definitions. Steele believed competency as the ability to perform activities essential to a profession (5). Other researchers summarized people's competence in having individual and personality traits, occupational skills, as well as knowledge (6). The International Confederation of Midwives considers the competence of prenatal care providers a combination of their knowledge, professional behaviors, and special skills. In conducted studies in Africa, participants pointed out to the professional skills of care providers (7,8). The findings of other studies revealed that the individual characteristics of health care provider were important for patients (9,10). Also, in a research conducted in South Africa, pregnant women intended their midwives to communicate emotionally and aware their feelings at the time of childbirth (11).
Although some studies have analyzed the competence of health care providers (12), the expected and current statuses of the competencies of prenatal care providers has not been so far considered and compared by researchers. Therefore, it is significant to examine what competencies the pregnant prenatal care providers should have and how far they are from the current status, according to viewpoints of prenatal care recipients. The gap between the current status of competencies and what is expected will lead to the identification of needs, and the required decisions to reduce this gap will be made according to the views of care recipients (13).
Based on the above, having enough information about the gap between the current status and the expectations of pregnant women from the competencies of prenatal care providers is necessary and a basis for prenatal care providers that improve their competencies. This study was aimed for assessing of prenatal care providers’ competencies according to the viewpoints of pregnant women. It is hoped that the findings of the present study will help health care providers and planners implement strategies meeting the expectations of those pregnant women and minimize the gap between the expected status and current status of prenatal care providers’ competencies.
Method
This is an analytical descriptive study. The statistical population included all pregnant women referring to prenatal care clinics affiliated to Shiraz University of Medical Sciences, Iran in 2019. To collect data, according to the given number of items in the questionnaire (60 items) and considering 5 samples for each item (14), 300 self-report questionnaires were completed by qualified samples that had been selected by convenience sampling method in Shiraz, Iran. Inclusion criteria in this study included: (1) pregnant women, (2) having Iranian nationality, and (3) being interested in participating in the research.
The data collection tool was a researcher-made questionnaire for comparing the expected and current statuses of competencies of prenatal care providers. The questionnaire was designed according to the results of an analysis of interviews with prenatal care recipients, prenatal care providers, and a literature review.
Validity and Reliability
Face, content, and structural validities of the questionnaire were investigated. For quantitative content validity of the questionnaire, the content validity ratio (CVR) was 0.76 and the content validity index (CVI) was 0.90, which were acceptable both of them (15,16). The structural validity placed questionnaire's items in 4 factors of professional skills, communication skills, individual characteristics of prenatal care providers, as well as characteristics of prenatal care and birth centers. Cronbach's alpha and stability (17) of this questionnaire were 0.941 and 0.951, respectively. The final questionnaire comprised of 2 parts. The first part included the participants’ demographic characteristics. The second part consisted of 60 items including the professional skills of prenatal care providers (15 items), the communication skills of prenatal care providers (20 items), the individual characteristics of prenatal care providers (15 items), and the characteristics of prenatal care and birth centers (10 items). For each item, 2 expected and current statuses were considered. Items of the expected status of competencies were in the form of a 5-point Likert scale (strongly agree to strongly disagree) where score 1 represented “strongly disagree” and 5 represented “strongly agree.” Items of the current status of competencies had a 3-point Likert scale (strongly, to some extent, never) that scores ranged from 3 “strongly” to 1 “never”.
The statistical analysis of the data was performed by means of descriptive statistics (mean, standard deviation) and inferential statistics (paired t-test) using SPSS 21 software.
Results
Demographic characteristics of 300 participants are presented in Table 1.
Demographic Characteristics of Participants in the Study.

Findings of comparing the expected status of the prenatal care providers’ competencies and the current status are presented in Table 2. At confidence level of 95%, the results of the paired t-test revealed a significant difference between the mean scores of the expected and current statuses in dimensions of communication skills, individual characteristics of prenatal care providers, and the characteristics of prenatal care and birth centers. Furthermore, the table shows that the professional skills of prenatal care providers were the most important and the individual characteristics of prenatal care providers were the least important competencies for the prenatal care recipients.
Comparison of the Mean, Standard Deviation, and Percent of the Scores of the Prenatal Care Providers’ Competencies.

Findings of Table 3 indicate that the most significant difference between the mean scores of the expected and current statuses in dimension of professional skills was related to “making phone contact” with providers during pregnancy. Moreover, there was a statistically significant difference between the mean scores of the expected and current statuses in some item of communication skills of prenatal care providers, characteristics of prenatal care and birth centers, and the individual characteristics of prenatal care providers. In dimension of communication skills, the most difference between the mean of the expected and current statuses was related to the item of “allowing for one person to be present at labour.”
Comparison of the Mean Scores of the Competencies of Prenatal Care Providers.
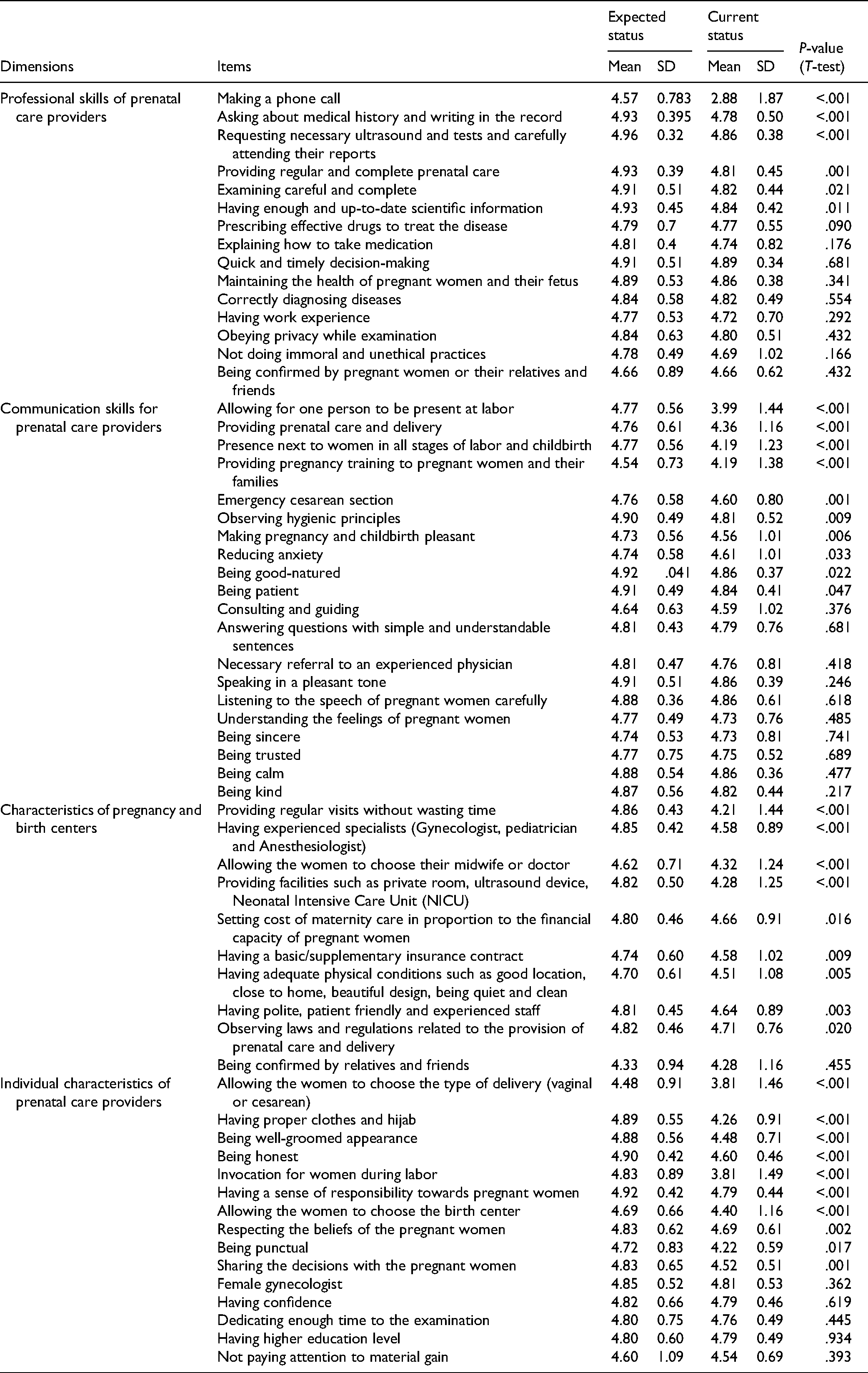
In dimension of the characteristics of prenatal care and birth centers, the maximum difference was observed in the item of “having regular visits without wasting time,” and in individual characteristics of prenatal care providers, it was observed for “allowing for choosing a vaginal childbirth or caesarean delivery.”
Discussion
In the present study, the competencies of prenatal care providers were assessed. The findings of this study revealed no significant difference between the mean scores of the expected status and the current status of prenatal care providers’ professional skills. Nevertheless, there were significant differences between the mean scores of the expected and current statuses in the dimensions of communication skills as well as individual characteristics of prenatal care providers and prenatal care and birth centers.
In this study, although there was no significant difference between the mean scores of the expected status of prenatal care providers’ professional skills and current status, there was a significant statistical difference between the scores of the expected and current statuses of some items. In this dimension, the maximum difference between the mean scores of the current and optimal statuses was for the item of “making a phone call” during pregnancy. That is, there was a gap between the expectations of the pregnant women to make a phone contact to their care provider and the current status. The results of our research were in line with the findings of some conducted studies. For instance, the findings of a study in Thailand indicated that women receiving educational text messages by phone during pregnancy had significantly higher levels of satisfaction compared to those not receiving text messages (18). Moreover, in a study, the observance of privacy of individuals, one of the expected expectations of pregnant women in our study, has been regarded as a right of clients (19). Furthermore, WHO has emphasized that all pregnant women have privacy and they must be respected during labor and delivery (20). Other expectation of participants in the present study was to take a complete history, perform accurate physical examinations, request timely laboratory tests, and record and report them accurately, which is important in early diagnosis of complications and controlling maternal health and this may quickly detect potential problems, so that it has been emphasized as part of midwifery care (21). In the present study, these expectations significantly differed from the current status. The gap between the expected status and current status of these items may be related to the inexperience of prenatal care providers, lack of enough knowledge, or lack of use of medical knowledge.
The findings of this study revealed a significant difference between the score of the expected status and the current status in the dimension of communication skills. This difference was observed between the expected score of some items of communication skills and current status. The highest difference between the average score of the expected and current statuses was the item of “Allowing for one person to be present at labour.” In line with the results of this study, another study indicated that having a companion (attendance) during labor and delivery is effective in creating physical and mental comfort of the woman because of physical and emotional support (22). Due to the importance of communicating between health care providers and caregivers, the patients participating in another research also expected physicians and healthcare professionals to be actively communicated with them (23). The authors of a research attributed the gap between the expected status and the current status of communication skills to the lack of knowledge or inattention of providers in this field. Furthermore, other causes such as cultural, social, economic issues, and workload were considered to be effective (24).
In the present study, there was a statistically significant difference between the scores of the expected status and the current status of the characteristics of the prenatal care and birth centers. In this dimension, a significant statistical difference was seen between the mean scores of the optimal status and current status of all items except “being confirmed by relatives and friends.” This significant difference argues that the expectations of pregnant women in these centers have not been met. Moreover, it can indicate that the work force, facilities, and management system of these centers have to be changed to provide comfort and peace of mind for health care recipients. According to a study, researchers who investigated the level of patients’ satisfaction with health care providers realized that clients had values in mind to assess the staff behavior, structures, physical space, as well as the center equipment (25). In this study, the highest difference between the mean score of the expected and current statuses of the characteristics of prenatal care and birth centers was related to the item of “having regular visits without wasting time.” The expectations of the participants in other studies were in line with some of the findings of our study. Investigators reported short waiting time for visits was one of the key factors in choosing health care centers (9,26).
Furthermore, in Nigeria, the competence of midwives and physicians of health centers was one of the main factors affecting the selection of maternity ward by women (27). One of the priorities investigated from the viewpoints of health care providers and caregivers in an Iranian research was the right to choose a physician (28). Since care centers are one of the key institutions of the health system using human, physical, financial, and equipment resources to provide, maintain, and promote community health, the use of competent human resources along with an optimal management system in these centers may lead to client satisfaction and reduce the gap between the expected status and the current status (29).
In the present research, there was a significant gap between the score of the expected status and the current status of prenatal care providers’ individual characteristics. This significant difference was observed between the scores of the expected and current statuses of some items. The maximum difference was observed between the mean score of the expected status and current status in the item of “allowing the women to choose the type of delivery (vaginal or caesarean section).” In order to reducing the space, Otogara et al. recommended that midwives and other health care providers should assist pregnant women in choosing the type of delivery through providing the necessary training in choosing the type of delivery and expressing the pros and cons of each delivery type (30). Unlike the participants of a study who claimed that the physician's gender is important to them (9), there was no statistical difference between the score of the expected status and the current status of this item in our study and the reason could be the choice of female students for midwifery and gynecologist in Iran. The findings of another study showed that the health care provider should have suitable individual characteristics like a well-groomed appearance (31) that was in line with the expectations of the participants in the current study.
Finally, it may be stated that the gap between the scores of the expected and current statuses indicated that the prenatal care providers’ competence in the dimensions of prenatal care providers’ communication skills and individual characteristics needs to be improved. Moreover, providers should provide prenatal care and delivery in centers with the expected specifications of pregnant women. In fact, these centers should try to meet the expectations of pregnant women through having a good management system, employing the competent human resources, as well as making optimal use of financial and equipment resources. Besides, prenatal care providers should strive to strengthen the expected skills by the pregnant women. To minimize the gap between the expected and current statuses of the competencies of prenatal care providers, training in various skills may be a good step to improve all the competencies of prenatal care providers. Furthermore, universities and higher education institutions are expected to choose students with the high potential to play their future role. Moreover, they should train graduates to have the required skills to provide prenatal care and the responsibility they will take on in the future. Healthcare providers organizations should also continuously evaluate the competencies of maternity care providers and survey their caregivers; since a feedback loop makes it possible for health care providers to able to establish in-service retraining courses according to the present needs and approach the optimal status in case of any gap between the prenatal care recipients’ expectations and the prenatal care providers’ current status.
It is recommended to conduct similar studies in other cities in Iran and identify the gap between the expectations of pregnant women and the current status. Then, according to the needs in each region, suitable planning should be performed in order to improve the competencies of prenatal care providers and minimize the possible gap.
Conclusion
The findings of the present study revealed that it is necessary to upgrade some competencies of pregnancy care providers. In the dimensions of communication skills, the characteristics of prenatal care and birth centers, and the prenatal care providers’ individual characteristics, there was a significant difference between the score of the current status and the expected status of these competencies. To upgrade these, prenatal care providers must spend all their energy to improve the expected skills by those receiving the services. Taking measure to close these gaps will help the health system approach its goals.
Footnotes
Acknowledgments
The authors would like to appreciate all the prenatal care providers, pregnant women, personnel of health centers and hospitals affiliated to Shiraz University of Medical Sciences who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The present study is part of the PhD dissertation of corresponding author (Mahboubeh Hajifoghaha) in Reproductive Health which received the code of ethics of IR: SBMU.PHNM.1396.843 from Joint Ethics Committee of Nursing, Midwifery and Pharmacology faculties at Shahid Beheshti University of Medical Sciences, Iran.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the “Joint Ethics Committee of Nursing, Midwifery and Pharmacology faculties at Shahid Beheshti University of Medical Sciences, Iran (Approval ID: IR. SBMU.PHNM.1396.843) “approved protocols.”
Statement of Informed Consent
Verbal informed consent was obtained from the pregnant women for their anonymized information to be published in this article.