
Abstract
Introduction
Supporting people as they consider their reproductive goals is a key component of comprehensive healthcare, particularly for those with chronic health conditions such as cystic fibrosis (CF). Routine clinician-patient discussions are recommended to facilitate patient-centered reproductive goals counseling and care to optimize pre-pregnancy health and prevent unintended pregnancies or births.1,2 Typically, it is assumed that primary care providers (PCPs) and reproductive health specialists provide such counseling; 3 however, national data indicates that only 14% of United States (US) primary care visits with non-pregnant reproductive-age people include contraceptive or pre-pregnancy counseling. 4 Furthermore, a recent survey found that 41% of adult women with CF report that they have no PCP and over 85% view their CF provider as their “main doctor”. 5 As people with CF (pwCF) are reaching adulthood in increasing numbers and considering their reproductive futures, it is crucial for their CF specialists to address reproductive health concerns.6,7
Women with CF report significantly lower utilization of reproductive health care and preventive services compared to the general US population.8,9 While CF providers feel that sexual and reproductive health care provision should be standardized for pwCF, especially as they face a myriad of general and CF-specific concerns, 10 there are major discrepancies between the importance providers place on this aspect of care and how often they discuss it. 11 Similarly, PCPs or reproductive health specialists may have insufficient expertise to provide disease-specific care for those with a chronic disease and may defer such care to the subspecialist. 12 As a result, pwCF may perceive this lack of clear care direction and feel they have less access to relevant education and resources related to reproductive health. 13
In our formative interview and focus group research among 38 adult women with CF, we found that they believe a disease-specific reproductive goals decision aid would encourage relevant parenting, pregnancy, and contraceptive discussions with their CF team. 14 This paper reports on our development process for MyVoice:CF, a novel web-based reproductive goals decision aid, to help women with CF engage in shared decision making regarding family planning. Given the importance of co-production or stakeholder input into the design of care interventions, 15 we highlight our formal process of partnering with and measuring stakeholder engagement in the development of this tool.
Methods
Conceptual Model
The conceptual models that informed MyVoice:CF development centered both on reproductive autonomy and shared decision making.16,17 Reproductive autonomy, or the ability to have ownership and freedom over one's reproductive choices is multifactorial and includes societal and cultural considerations and the influences of partners, family, and healthcare providers.18,19 Shared decision making is a communication approach where patients elucidate their priorities, providers offer the best available evidence, and patients are supported to consider these factors when faced with a decision. 20 Often, health decisions are heavily preference-sensitive and must be made in complex or unclear clinical situations where there is usually no clear medically superior choice. In such situations, decisions are dynamic or conditional. 21 People may have complex feelings about achieving parenthood or avoiding pregnancy that can make discussions in the clinical context challenging. Supporting shared decision making and reproductive autonomy in these scenarios is dependent upon encouraging patient self-determination to improve health behaviors and outcomes. 22 Our conceptual model pairs these frameworks by incorporating patient-centered approaches while providing up-to-date medical evidence to best support pwCF safely achieve the reproductive goals that are right for them and for their families. 23
Decision aids provide information and support to help users as they make health decisions aligned with their values and priorities. A Cochrane review found that people exposed to decision aids felt more knowledgeable and informed, had decreased decision conflict, and had a more active role in values-concordant decision making. 24 We designed the web-based MyVoice:CF to support reproductive autonomy by allowing users the opportunity to clarify their goals and concerns independent of a clinical encounter. To encourage shared decision making and self-determination, MyVoice:CF supports users as they formulate and clarify questions and concerns that will ultimately facilitate patient-provider discussions about family planning.
Systematic Development Process
Stakeholder Engagement
We recruited a stakeholder panel consisting of adult women with CF, CF providers, and women's health providers. We identified patient stakeholders from local CF centers and from participants in prior reproductive health-related advocacy efforts. We attempted to select individuals of various ages and from varied geographic locations. We did not include adolescent women with CF in this study due to concerns regarding age of consent and regulatory approval and potential reticence to contribute in adult group engagement. We identified care team stakeholders through recommended contacts from the principal investigator (PI)'s clinical and research colleagues based on expertise in reproductive health and CF. After identification of potential stakeholders, the PI conducted individual calls or corresponded via email with each stakeholder to begin relationship-building. If the identified potential stakeholder wished to participate in the project, we explained the stakeholder role and expectations and invited the stakeholder to join.
Stakeholders partnered in MyVoice:CF development through regularly scheduled feedback sessions. Due to CF infection control policies, patient stakeholders could not meet in-person; thus, we conducted stakeholder meetings via video conference calls guided by the PI and research team. We used email correspondence to facilitate ongoing communication as topics arose between scheduled meetings. During the initial conference call and email correspondence, the PI reviewed the roles and expectations of stakeholders in the project and the overall process of stakeholder engagement. A research team member took notes during all calls. We tracked all recommendations provided by stakeholders through discussion in post-call study team meetings and review of written notes. We further incorporated the perspectives of pwCF by drawing on our prior work related to reproductive health in this population.6,8,9,11,13,25–29
Storyboard and Prototype Development
We developed MyVoice:CF using best practices for patient-facing decision aids drawn from the evidence-based International Patient Decision Aid Standards (IPDAS).30,31 Based on our formative research, we developed the initial “storyboard” of MyVoice:CF from an existing patient-centered, web-based reproductive decision support tool for primary care called MyPath. 32 MyPath was designed to act as a family planning tool for female veterans receiving care through the VA Healthcare System. The tool asks participants to clarify their reproductive goals through a series of questions, then allows users to explore sections related to preconception planning, prenatal care, and birth control. At the end of MyPath, a PDF report is generated which summarizes the user's reproductive goals and questions for them to share with a healthcare provider.
During calls, all stakeholders brainstormed and ranked the important reproductive health topics that should be targeted by a CF-specific decision aid. The group also provided input on the tool's content, language, and design. Conference calls occurred routinely throughout the project (with a target of every 3–4 months) and we provided email updates on the development process between meetings. The PI and research team reviewed all feedback and recommendations and provided stakeholders with call summaries and results of recommendations.
The proposed storyboard content and functionality for MyVoice:CF drew from our prior work related to reproductive health in this population6,8,9,11,13,25–29 and the iterative input from our stakeholder panel. The initial storyboard highlighted the proposed content and illustrations for the tool using Microsoft PowerPoint. We then developed the web-based prototype with support and input from our design and development partners. All stakeholders iteratively reviewed and edited MyVoice:CF prototypes using group editing and email correspondence. All stakeholders had the opportunity to provide edits and approve the finalized tool.
Evaluation
Our evaluation examined and measured the process of stakeholder engagement in creating MyVoice:CF. At midpoint and end of the project, we emailed an anonymous online survey asking stakeholders to self-describe their role in the project as well as assess the frequency of engagement, co-learning, and transparency. This survey used the Ray and Miller framework (Table 1), 33 which is designed to measure the self-perceived degree of engagement and impact on a topic or project. The PI and research team assessed stakeholders’ impact on the decision aid development through stakeholder recommendations and input during conference calls, emails, and group editing. We obtained IRB approval as non-human subjects research from the University of Pittsburgh Institutional Review Board (STUDY 18110091); we, in turn, did not need to obtain informed consent from stakeholders prior to participation in this project. We compensated all stakeholders equally for their attendance at each study call with 50USD Amazon gift cards.
Stakeholder Survey Items for Evaluation of Engagement Process.

Stakeholder Survey Items for Evaluation of Engagement Process.
Evaluation and Outcomes of Stakeholder Engagement Process
Fourteen stakeholders participated in this project. All potential stakeholders who were invited participated in the project. Eight and 10 stakeholders completed the mid- and post-project stakeholder surveys, respectively. At each time point, the majority of stakeholders felt that they had received adequate information about the project (88% at the midpoint and 90% at the end of development), were satisfied with the amount of feedback they were able to provide (88% and 90%), had their expectations met or exceeded (100% and 100%), and were satisfied with the frequency of engagement in the project (63% and 85%). All stakeholders provided multiple concrete recommendations during the development process and reported that they were satisfied with the research team's response to their recommendations (100% at the midpoint and 90% at the end of development). Stakeholder group composition, attendance during conference calls, and attitudes toward the engagement frequency are summarized in Table 2.
Evaluation of the Stakeholder Engagement Process of Creating SRH Educational Resources for AYA Women with CF.

Evaluation of the Stakeholder Engagement Process of Creating SRH Educational Resources for AYA Women with CF.
*One stakeholder did not provide information on their gender, race or ethnicity.
When asked to describe their role in the project in an open-ended fashion, the majority described themselves as a “consultant” or “reviewer”. Stakeholders were also asked to describe their experience with the project compared to their expectations. The majority of participants felt their expectations for the project had been met or exceeded. One participant commented, “I appreciate the leadership's willingness to hear and consider all comments from all stakeholders.” Another agreed, stating, “It has been easy to be involved, share perspectives, and contribute.” Stakeholders unanimously agreed that they received sufficient information to provide feedback on the project via co-learning. Stakeholders also unanimously agreed that their input was incorporated and valued, with one participant commenting, “[The study team is] wonderful in soliciting feedback and input, and implementing suggestions when appropriate.”
Our mid-point survey indicated some stakeholders desired more frequent meetings. Prior to this survey, there had been an 8-month gap between meetings as our designers developed an initial prototype. Following receipt of this feedback, our stakeholder meetings were held every 4 months.
Stakeholders reflected on the motivations of women with CF related to family planning and agreed that the ideal resource should be web-based. They also decided that a key goal of the tool should be to enhance patient-provider communication and shared decision making related to reproductive goals. It was agreed that this decision aid was not intended to replace patient-provider counseling or interactions but, rather, would serve to provide users with information relevant to their personal reproductive goals and key questions to pose to their CF providers.
Importantly, stakeholders noted that MyVoice:CF should be applicable to anyone with gestational capability, regardless of their gender identity or that of any sexual partners. In aspects of the tool that highlighted known sex-based differences in CF health (likely driven by innate female sex hormones) or when referencing studies conducted with females with CF, we intentionally used the words “female” or “women”; otherwise, we attempted to use gender-neutral language and pronouns throughout MyVoice:CF.
One example of significant stakeholder impact on the tool was the removal of an image used in the birth control section. The design team had included an image of a woman in a wheelchair, intended to make the tool welcoming to a broad range of users. Stakeholders reacted negatively to this image, noting that, within the context of CF, a wheelchair often signifies severe disease and end-of-life status. Due to the reactions elicited by this image, we opted to remove that image from the tool.
Stakeholders decided by consensus to use the underlying principles of the existing MyPath reproductive decision support tool to develop MyVoice:CF. Additionally, they agreed that all content be derived from current medical evidence and references to source publications be cited and linked in the tool. Key sections and functionalities of MyVoice:CF are highlighted below:
Exploratory Questions About Parenthood, Pregnancy, and Children: Similar to MyPath, the opening section of MyVoice:CF includes a series of patient-centered questions designed to help the user consider their personal reproductive goals. Recent research demonstrates that beliefs about potential parenthood or pregnancy at any given time exist on a spectrum, from clear, binary intentions to plan or avoid pregnancy to ambivalent, labile, or conflicting feelings.34,35 Thus, this section is designed to help users consider both their cognitive and affective thoughts toward pregnancy and parenthood. Stakeholder input was essential in deciding the content, potential responses and order of the questions. For example, women who have been struggling with infertility may have emotional reactions to questions about if and when they become pregnant. In response to our stakeholder group's concerns that the personal nature of the questions might be uncomfortable for some users, especially in the opening of the tool, we decided that the public version of the tool should include a response option of “I’d prefer not to answer” to the questions. This feature will be incorporated after efficacy, feasibility, and acceptability studies have been completed. Following the exploratory questions, users are presented with a menu of the different pregnancy and parenting topics covered by the tool. Users can select which topics they want to view, or they can opt to skip to the section on birth control (Figure 1).
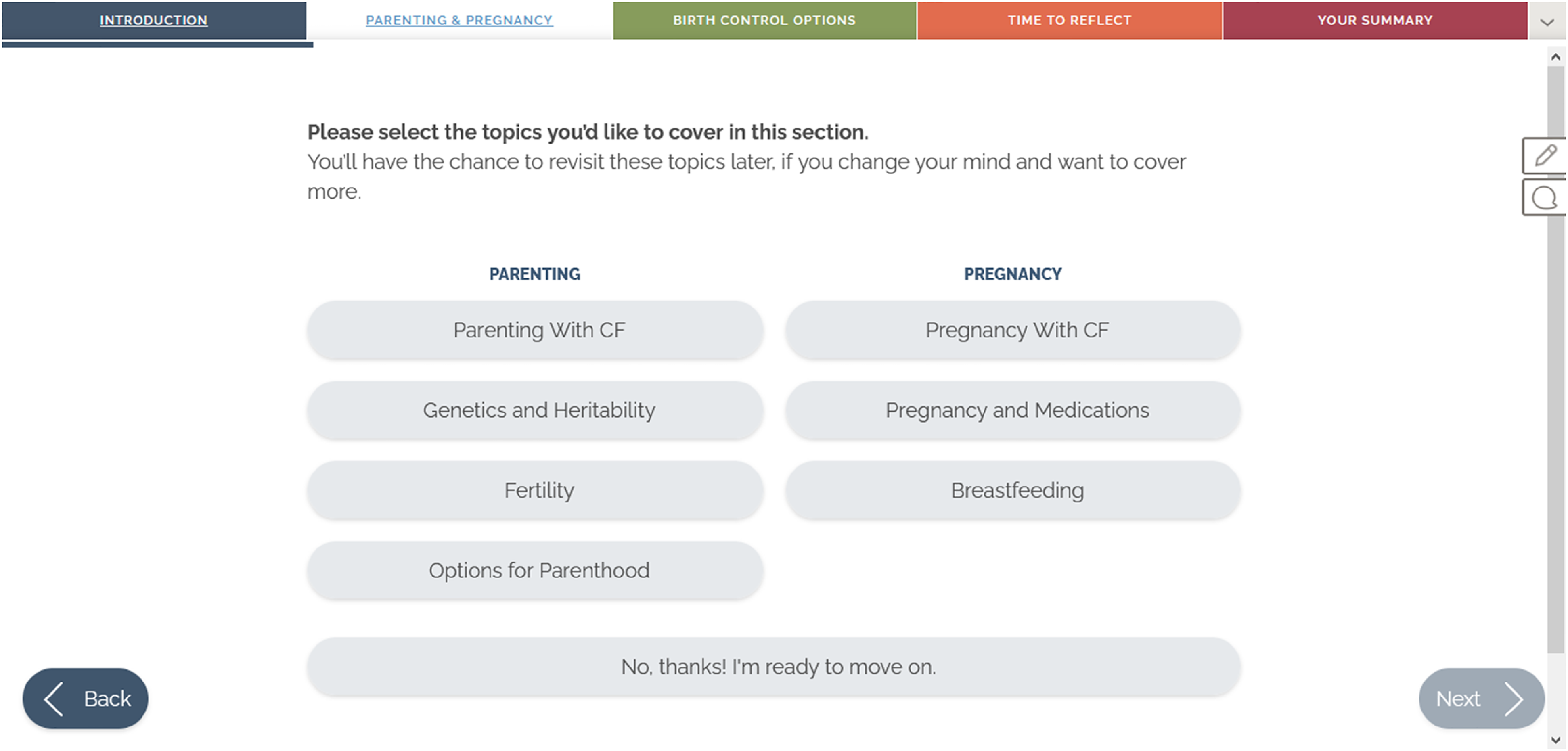
The topics menu for myVoiceCF. Users select all topics they are interested in browsing.
Parenthood and Pregnancy. This section includes frequently asked questions and answers developed to support informed decision making by addressing common concerns related to parenthood and pregnancy for a person with CF.14,30 Users begin the section by selecting topics of interest and then view each topic sequentially. After viewing their selected topics, users can select more topics or move on to the next section. Figure 1 is a screenshot of the main page and layout of this section of the tool.
Parenting with CF: This section addresses potential concerns and barriers to being a parent, including the impact of parenthood on life expectancy, and provides coping strategies to issues such as balancing health and parenting, postpartum depression, anxiety, infection control with young children, and financial difficulties. Each of these issues is accompanied by strategies, such as having a predetermined plan for childcare if the user is hospitalized, and links to relevant resources. All stakeholders significantly contributed to the content and formatting of this section.
Genetics and heritability: This section addresses the genetics of CF as well as if and how partners can be tested for carrier status. We included relevant resources as well as sample language for women to ask their CF care team for a referral to a genetic counselor.
Fertility: This section begins with a video explaining the biological processes that lead to pregnancy, including ovulation, fertilization, and implantation. Next, the section addresses CF-specific fertility concerns, including addressing the misconception that all women with CF are sub-fertile or infertile. Users can access information on fertility treatment options and any CF-specific considerations. Stakeholder input led to the removal of information regarding declining fertility throughout the female life course as it was felt to be extraneous to the purpose of this CF-specific tool.
Options for Parenthood: The tool includes a section dedicated to becoming a parent through means other than pregnancy. This section highlights the logistics and laws regarding adoption, surrogacy, and foster care, as well as links to additional resources for each of these paths to parenthood. Stakeholders agreed on the importance of this section due to the concerns related to pregnancy in the setting of severe CF disease.
Pregnancy with CF: In this section, we explain the interplay between CF and pregnancy, including topics such as pulmonary exacerbations, gestational diabetes, pre-term delivery, constipation, pregnancy-related hypertension, and breathing capacity. The tool also explains how medical care may change during pregnancy to incorporate care from maternal-fetal medicine specialists, genetic counselors, lactation consultants, and others. It includes a timeline showing what kinds of procedures and healthcare appointments to anticipate before pregnancy, during each trimester, and in the postpartum period. This section emphasizes that there are health-related benefits to planning when to become pregnant. It highlights different CF-related factors that can influence or affect pregnancy planning, including lung function, nutritional status, CF-related diabetes, CF-related liver disease, and lung transplant. With the help of our stakeholders, we crafted this section to avoid specific recommendations and instead encouraged discussion about these factors with the user's CF care team.
Pregnancy and Medications: Because decisions about medication use during pregnancy can be dependent on individual health factors, this section emphasizes the importance of informing the CF care team when pregnancy is planned, suspected, or confirmed. The user can then select CF-related medications from a list based on which medications they want to discuss with their CF care team. Because of the increased use of newly available therapies, we also included a page noting that research on the use of new therapies during pregnancy is ongoing and recommended discussions with the CF care team and obstetrician. Stakeholders assisted with the decision to provide the user the ability to look up and select their own medications rather than view the known risks of each medication commonly used in CF care.
Breastfeeding: This section addresses common concerns about breastfeeding, including the nutritional content of breastmilk produced by women with CF as well as the impact breastfeeding can have on the parent's weight. Users can again add any medications that they wish to discuss with their CF care team.
Birth Control: This section provides education about the attributes of birth control methods (efficacy, side effects, mode of delivery and frequency of administration), elicitation of women's preferences, and CF-specific contraceptive information (Figure 2). Given concerns related to the hormonal impact of contraception on CF disease, 14 we specifically highlight the utilization of female sex hormones in contraception. Users can conduct a side-by-side comparison of up to four birth control methods. MyVoice:CF also highlights abortion as an option and the use of emergency contraception to prevent pregnancy.

An information page about oral contraceptives and CF-specific considerations for myVoiceCF.
Time to Reflect: This section allows the user to reflect on parenthood/pregnancy in several ways. First, the user can opt to reflect on previously identified key considerations related to this decision as derived from prior evidence and stakeholder input.14,30,36,37 Users can also reflect on the attitudes of key supports such as partners, family members, or friends. Finally, users can explore their gut or “reflex” reactions to considering parenthood and/or pregnancy. Regarding birth control, we incorporated reflection exercises into the Birth Control section to improve the flow of the tool, per stakeholder recommendation. Such exercises enable users to rank what aspects of birth control are most important to them (efficacy, frequency, side effects, etc.) as well as indicate their satisfaction with their current method of birth control.
In alignment with the goals of MyVoice:CF, stakeholders integrated the ability for users to easily select questions for their CF team or healthcare providers throughout the tool. All users of MyVoice:CF are prompted to review the list of questions they added through an exercise at the end of the tool and to add additional questions or delete previously selected questions to be added to their Summary Page (outlined below).
Key Features and Summary Page: As users progress through the tool, they can select information buttons, resources, and medical literature citations and add free-text questions and notes in a text box that are populated on a Summary Page. All questions added from the reflection exercise above are highlighted on the Summary Page. For users who complete the contraception section, the Summary Page includes a list of preferences for birth control methods and comparisons of user-selected methods. The Summary Page can be emailed and subsequently printed, giving users the choice whether or not they wish to share it with their healthcare providers or others, per our stakeholders’ recommendation. Figure 2 is a mock summary page including several questions, resources, and birth control considerations. Users can also provide feedback on any given page throughout the tool through the use of a reaction button and free-text responses.
Discussion
This study describes the development of a reproductive goals decision aid for women with CF using a formal process for and evaluation of stakeholder engagement. It highlights the importance of contributions of stakeholders to the content and relevance of the MyVoice:CF tool. Critically, we successfully demonstrate a formal process for reporting the methods and evaluation of stakeholder engagement that could be extended to resource and intervention development for improving other aspects of CF care. 33
Stakeholder engagement or co-production is the process of inviting patients, families, and providers to participate in the design and delivery of healthcare. 38 Such engagement was crucial to the development of MyVoice:CF as we believe our tool became more relevant and meaningful for both patients and health care providers. 39 Unfortunately, the process of stakeholder engagement is often not detailed or evaluated in the literature. 33 In this study, we embedded key principles for effective engagement, including the recruitment of a balanced stakeholder group, participant understanding of the project and their roles, expert facilitation, establishment of connections among participants, and active and dynamic discussions throughout the research process. 40 By documenting the outcomes of our stakeholder engagement process and the results of its evaluation, we hope to encourage implementation of such a framework to improve the quality of similar patient-centered research and the development of educational resources and interventions.
Several acceptable and effective decision aids are focused on reproductive health considerations and goals for the general population.32,41,42 Additionally, colleagues are pursuing the development of a similar disease-specific tool for those with rheumatic diseases called MyVoice:Rheum. We recognize that women value the opportunity to discuss their reproductive goals and needs with CF providers.14,30 However, understanding of how to initiate these conversations while remaining patient-centered are limited. 40 Women may feel uncomfortable with direct questions about their reproductive goals or plans due to privacy concerns, mistrust of provider motivations, and concerns about being judged.43,44 Our prior work among women with CF found that many did not share their pregnancy intentions with their CF team for fear of judgment related to their choice. 30
In response to such complex considerations, reproductive goals decision aids, such as MyVoice:CF, give users the opportunity to personally and privately consider their reproductive goals and provides them control over disclosure of this information to healthcare providers or others. By highlighting specific questions to consider related to reproductive health, it is our hope that it will assist with the quality and quantity of reproductive goals discussions with their healthcare providers and improve shared decision making related to family planning.
We incorporated the majority of stakeholder recommendations into MyVoice:CF development. It is our hope that our intentional use of stakeholder input and co-production will result in high acceptability and feasibility of MyVoice:CF among pwCF and CF providers. We are undertaking a single center feasibility trial of the tool among women with CF with the primary outcomes of acceptability and usability and an exploration of the preliminary efficacy of MyVoice:CF's impact on shared decision making and the quality and quantity of reproductive goals discussions between pwCF and the CF team (NCT04825236).
A major limitation of this project is the lack of consistent reporting guidelines for this type of work. To alleviate this issue, we chose key guidelines for decision support tool development and effective stakeholder engagement and used a proposed process for research on stakeholder engagement.31,33 We did not record or code stakeholder meetings as the goal of our assessment was to measure the degree to which stakeholders felt they had control over the final tool; future work with stakeholders may follow a more traditional qualitative methodology by recording and coding each meeting.
Although we attempted to create MyVoice:CF in a manner that avoids assumptions about users’ gender identity, we did not have any trans, non-binary, or gender-expansive individuals with gestational capacity on our stakeholder panel. Additionally, our stakeholder group did not include partners or family members of pwCF, despite their key roles in reproductive decision making. We also had limited male provider input and a lack of diversity related to race, ethnicity, and socioeconomic status of our stakeholder group. Future modifications of MyVoice:CF should include such voices to enhance the relevance and applicability of the tool. Finally, we may be missing key feedback on the engagement process from all participants as only two-thirds of stakeholders completed the anonymous evaluation survey.
Conclusion
In summary, this study describes the development of a novel, web-based, patient-centered reproductive goals decision aid for women with CF. By using rigorous and planned processes for engaging stakeholders, this strategy of intervention development could benefit the CF community. If the tool is successfully utilized by women with CF and enables conversations that lead to improved understanding of options and decreased decisional conflict regarding reproductive goals, it could be extended to other emerging comprehensive care concerns among pwCF and to other populations of women with disease-specific concerns related to reproductive health.
Practical Implications
Aside from future feasibility and efficacy testing of MyVoice:CF, future directions for this work include the development of similar decision aids for males with CF and other patient-centered interventions to encourage discussion of reproductive goals between pwCF and healthcare providers. Future work should also focus on building the evidence that stakeholder engagement in intervention development is indeed valuable and leads to improvements in intervention feasibility and adoption. The methods used in this study may be useful in other chronic disease populations with unique sexual and reproductive health needs and experiences.
Footnotes
Acknowledgments
The authors would like to thank the pwCF and providers who provided crucial input and guidance for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cystic Fibrosis Foundation (grant number KAZMER18A0-Q).