
Abstract
Chronic kidney disease (CKD) is associated with substantial morbidity, mortality, cost, and increased caregiver burden. Peer mentoring (PM) improves multiple outcomes in various chronic diseases. The effect of PM on caregiver burden among caregivers of patients with CKD has not been studied. We conducted a randomized clinical trial to test the effectiveness of a structured PM program on burden of care among caregivers of patients with CKD. We randomized 86 caregivers to receive 6 months of intervention in 1 of 3 groups: (1) face-to-face PM (n = 29); (2) online PM (n = 29); and (3) usual care: textbook-only (n = 28). Peer mentors were caregivers of patients with CKD, who received 16 h of instruction. All participants received a copy of a textbook, which contains detailed information about kidney disease. Participants in the PM groups received FTF or online PM for 6 months. The outcome was time-related change in the Zarit Burden Interview (ZBI) score. There was a statistically significant decrease in the ZBI score (SE: −3.44; CI: −6.31, −0.57 [p = 0.002]) compared with baseline, among the online PM group. Online PM led to decreased caregiver burden among caregivers of patients with CKD. The study was limited to English-speaking subjects with computer literacy.
Introduction
Chronic kidney disease (CKD) and end stage renal disease (ESRD) are associated with considerable patient morbidity and mortality, as well as caregiver burden (1,2). CKD and its treatment influence a patient's role and function within the family and affects the entire household (3,4). Family members of patients with CKD are engaged in both the practical aspects of being caregivers (eg, transportation) as well as providing psychological and cognitive support during the decision-making process, particularly about the choice of renal replacement therapy (5,6). As a result of their role as caregivers, family members often experience stress, depression, negative changes in the relationship quality, marital dissatisfaction, and poor quality of life (QOL) (2,7). Yet, their needs are often neglected and under-prioritized, despite the obvious impact they may have on patient-centered care.
Knowledge about goals of care can help prepare family members for the practical aspects of the burden related to treatment options, engaging them in the patient's care. Educational interventions addressing factors that CKD patients and their families consider important are likely to facilitate choice of treatment that is congruent with the patients’ and their families’ wishes and values (5). Such interventions will improve the family members’ understanding of the risks and benefits of various treatments, facilitating discussions about expectations and goals of care. Patients have expressed concern about the often devastating impact of CKD on caregivers and have suggested assessment of caregiver burden and improvement of support for caregivers among research priorities (8).
Despite the increasing awareness of the burden and adverse effects of CKD on caregivers, high-quality evidence is lacking about the effect of information or support interventions on the psychosocial well-being of caregivers (9). Peer mentoring (PM) for caregivers of patients with chronic diseases has been shown to be perceived as positive, resulting in feeling of being understood and empowered, reducing anxiety and reducing sense of isolation. Much of the published work has focused on PM for parents of children with cancer, diabetes, inflammatory bowel diseases, and brain tumor (10–14). In a randomized clinical trial, we studied the effectiveness of structured mentoring by trained peers on burden of care as measured by Zarit Burden Interview (ZBI) (15), among caregivers of patients with CKD.
Materials and Methods
Study Overview
The protocol is fully described in the research report submitted to the Patient-Centered Outcomes Research Institute (PCORI) (16). We randomized caregivers of patients with CKD into 3 groups: (1) face-to-face (FTF) PM, (2) online PM, and (3) only usual care: review of a textbook about CKD. Participants in all 3 groups received a copy of a textbook, which contains detailed information about kidney disease. The research was conducted according to principles having their origin in the Declaration of Helsinki. All participants provided written informed consent. The protocol was reviewed and approved by the Pennsylvania State University College of Medicine Institutional Review Board. The clinical trial was registered with
Mentor Training (the Patient and Family Partner Program [PFPP])
Details of the mentor training program which have been previously reported (17) are briefly outlined. Since 2004, the Kidney Foundation of Central Pennsylvania (KFCP) has operated a comprehensive patient engagement and empowerment program (PFPP). The program trained CKD patients and their caregivers to serve as volunteer mentors to other CKD patients and their caregivers (17,18). In this trial, mentors were adult caregivers of patients with CKD, who received 16 h of formal training to become peer mentors (Supplemental Appendix A).
Interventions and Comparators (17)
Results

CONSORT diagram for flow of caregivers through the trial.
Baseline Characteristics of Caregivers According to Intervention Group.

Abbreviations: FTF, face-to-face; PM, peer mentoring.
Employed: employed, student, and homemaker.
Caregiver Burden Scores
In Table 2, we document the mean unadjusted ZBI scores in the 3 groups at baseline, 12 months, and 18 months. The mean unadjusted baseline scores did not statistically differ among the 3 groups.
Mean Unadjusted Zarit Burden Interview Scores Through the Study Period Among the Intervention Groups (Intention to Treat Analysis).

Abbreviations: FTF, face-to-face; PM, peer mentoring.
Table 3 shows the changes in mean unadjusted ZBI scores over the study period. FTF PM was associated with a statistically significant decrease (improvement) in the mean ZBI score at 12 months (change in mean [Δ]: −5.1; 95% confidence interval [CI]:−10.0, −0.2 [P = .04]). FTF PM was also associated with a statistically significant improvement in the ZBI score at 18 months (Δ: −7.1; CI: −12.2, −2.1 [P = .007]). Online PM was associated with a statistically significant improvement in the mean ZBI score at 12 months ([Δ]: −7.1; 95% CI:−13.3, −0.9 [P = .03]). Online PM was also associated with a statistically significant improvement in the ZBI score at 18 months (Δ: −8.4; CI: −14.9, −1.9 [P = .01]).
Changes in Mean Unadjusted Zarit Burden Interview (ZBI) Scores Through the Study Period by Intervention Group (Intention to Treat Analysis).
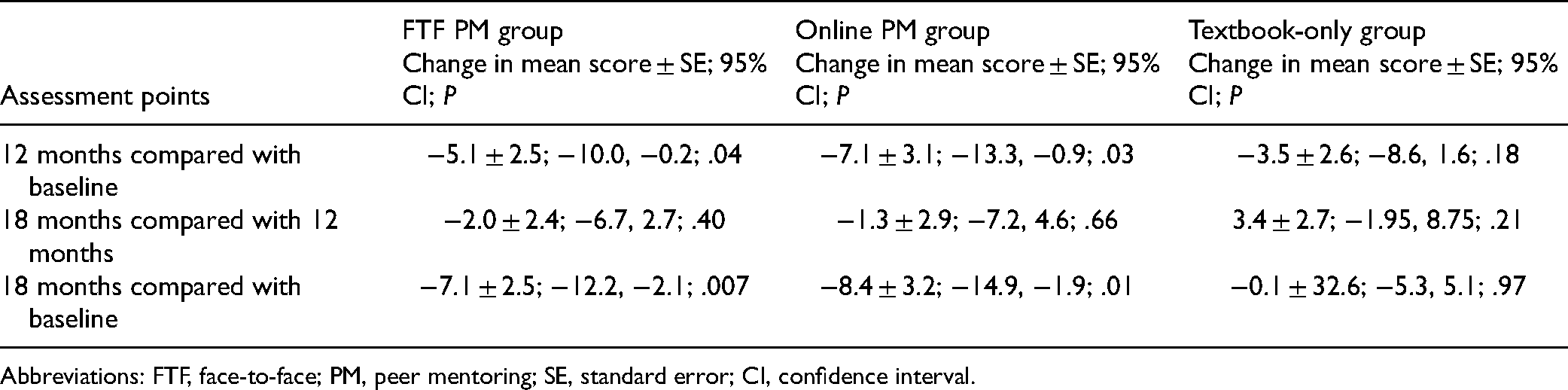
Abbreviations: FTF, face-to-face; PM, peer mentoring; SE, standard error; CI, confidence interval.
Table 4 shows the changes in mean ZBI scores over the study period, adjusted for demographic variables (race, ethnicity, sex, age quartile, marital status, education, employment status, rural/urban location). ZBI scores decreased significantly in the study period in the online PM group (SE: −3.44; CI: −6.31, −0.57 [P = .02]). No demographic variables had a significant independent effect on the change in ZBI scores among the groups.
Changes in Mean Adjusted Zarit Burden Interview Score Through the Study Period Among the Groups a (Intention to Treat Analysis).

Abbreviations: FTF, face-to-face; PM, peer mentoring.
Adjusted for race, ethnicity, sex, age quartile, marital status, education, employment status, rural/urban location.
The slope estimates represent change in scores in standard points over 18 months.
Discussion/Conclusion
The results from this study support the hypothesis that, among caregivers of patients with CKD, PM, particularly online PM, improves caregiver burden. We expected FTF PM to lead to at least similar results as online PM. We were surprised to find that online PM was associated with a better outcome. This is consistent with our previous finding of superiority of online PM compared with FTF PM in regards to improvement in QOL among CKD patients (17). We believe the accessibility and flexibility of online communication are the main contributors to the improved outcomes associated with online PM. This was noted by several mentors in their reports to the program coordinator.
In general, conclusions from previous studies about the impact of PM have been limited due to variations in PM programs, loose definitions of PM and lack of clear outcomes. Our clinical trial addressed those limitations by studying a structured PM program, in which mentors received formal training, the delivery of the PM program was relatively consistent and continuously monitored. The outcome was distinct and measured over a period of 18 months. Other strengths of our study include the engagement of patients, caregivers, and stakeholders during study design, recruitment, and delivery of the intervention, as well as close collaboration with a patient advocacy organization. A vast majority of the information about the role of PM among caregivers relates to parents of children with chronic conditions (10–14). Evidence regarding the role of PM among caregivers of adult patients is limited (35,36). This study is unique in reporting quantitative results of the effect of PM on caregiver burden.
This study has three main limitations. The first limitation is that participants were limited to English-speaking subjects with computer literacy and those with internet access. The second limitation is reliance on self-report as the source of information for adherence to the review of textbook and to the PFPP protocol. The third limitation is that insufficient number of rural and ethnically diverse participants resulted in limitations regarding geographic and ethnic generalizability. Future larger studies with participants from diverse backgrounds, including non-English speaking participants from rural and urban settings will allow for appropriate subgroup analyses. Development of a Spanish version of the PM program would facilitate inclusion of a more diverse group of participants. Furthermore, given the relative accessibility of smart phones compared with online platforms that require computer access, future studies of PM might allow for improved participation by employing a phone-based PM application.
Although certain aspects of the study are unique to caregivers of patients with CKD, and although the study benefitted considerably from the already existing infrastructure of the Kidney Foundation of Central Pennsylvania (KFCP) and the Patient and Family Partner Program (PFPP), the protocol and results may be generalizable to caregivers in other chronic disease settings. Future areas of potential research include assessment of the impact of PM among caregivers of children and adolescents with CKD and among caregivers of patients with other chronic medical conditions.
The specific aim of this study was to evaluate the effect of a PM program on caregiver burden among caregivers of patients with CKD. Online PM was associated with decreased burden of care among caregivers of patients with CKD. We conclude that online PM is an effective strategy that leads to improved caregiver burden in CKD with potential for use in other chronic disease states. The COVID-19 pandemic has underscored the need for online alternatives to in-person mentoring. Online programs also allow access to mentoring by populations with limited ability to travel and for regions with limited resources. The study was limited to English-speaking caregivers with computer literacy. Future, larger studies with participants from diverse ethnic and geographic backgrounds will permit subgroup analyses, allowing for conclusions about generalizability.
Data Sharing Statement
De-identified participant data will be made available to qualified external researchers, for a specific purpose in accordance with the PCORI Policy for Data Management and Data Sharing Plan: https://www.pcori.org/about-us/governance/policy-data-management-and-data-sharing.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221076314 - Supplemental material for Improving Caregiver Burden by a Peer-Led Mentoring Program for Caregivers of Patients With Chronic Kidney Disease: Randomized Controlled Trial
Supplemental material, sj-docx-1-jpx-10.1177_23743735221076314 for Improving Caregiver Burden by a Peer-Led Mentoring Program for Caregivers of Patients With Chronic Kidney Disease: Randomized Controlled Trial by Nasrollah Ghahramani, Vernon M. Chinchilli, Jennifer L. Kraschnewski, Eugene J. Lengerich and Christopher N. Sciamanna in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735221076314 - Supplemental material for Improving Caregiver Burden by a Peer-Led Mentoring Program for Caregivers of Patients With Chronic Kidney Disease: Randomized Controlled Trial
Supplemental material, sj-docx-2-jpx-10.1177_23743735221076314 for Improving Caregiver Burden by a Peer-Led Mentoring Program for Caregivers of Patients With Chronic Kidney Disease: Randomized Controlled Trial by Nasrollah Ghahramani, Vernon M. Chinchilli, Jennifer L. Kraschnewski, Eugene J. Lengerich and Christopher N. Sciamanna in Journal of Patient Experience
Footnotes
Acknowledgments
The investigators wish to acknowledge the following for their assistance in various stages of the study:
All patients and caregivers who participated in the study as peer mentors, as members of the advisory groups, or as study subjects; without their active and enthusiastic participation, this study would not have been possible. The Kidney Foundation of Central Pennsylvania (KFCP) and members of its Board of Directors who served as members of the Community Advisory Board. Parts of this study were presented in abstract form at the Annual Meeting of the American Society of Nephrology November 7–10, 2019 in Washington, D.C.
Author Contributions
Research idea and study design: NG, VC, JK, EL, CS; data acquisition: NG; data analysis/interpretation: NG, VC, JK, EL, CS; statistical analysis: VC. Each author contributed important intellectual content during manuscript drafting or revision, accepts personal accountability for the author's own contributions, and agrees to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Ethical Approval
The research was conducted according to principles having their origin in the Declaration of Helsinki. Written informed consent was obtained from all participants. The protocol was reviewed and approved by the Pennsylvania State University College of Medicine Institutional Review Board (Approval #STUDY00001339). The clinical trial was registered with Clinicaltrials.gov (NCT02429115).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Pennsylvania State University College of Medicine Institutional Review Board (Approval #STUDY00001339) approved protocols.
Informed Consent
Written informed consent was obtained from the caregiver participants for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this article was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award CDR-1310-07055 (to Nasrollah Ghahramani). The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee. VC, JK, EL, and CS were co-investigators on the study. The funding agency (Patient Centered Outcomes Research Institute), and the employer (Penn State College of Medicine/Penn State Health) did not have a role in the study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication.
Clinicaltrials.gov identifier: NCT02429115.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.