
Abstract
Despite the fact that millions of individuals living in the United States are coping with disabilities associated with traumatic brain injury (TBI), limited work has explored strategies for patient engagement in research among those with such injuries. The Coalition for Recovery and Innovation in Traumatic Brain Injury Care Across the Lifespan (CRITICAL) brought together those living with TBI, caregivers, clinicians, researchers, and advocates with the goal of developing a new patient-centered research agenda. This platform was also used to explore strategies to engage those with moderate to severe TBI in the research process. The CRITICAL was formed of 6 survivors of moderate to severe TBI, 2 caregivers of survivors of moderate to severe TBI, and 8 TBI professionals. The CRITICAL identified 3 priority topic areas: Relationship Quality, Caregiver Needs, and Thriving. Furthermore, strategies associated with Communication, Preparation, and the Environment facilitated research engagement. Employing the strategies outlined in this article is expected to promote patient engagement in clinical research, which can improve patient-centered interventions and outcomes for individuals living with TBI.
Keywords
Each year in the United States approximately 2.5 million people sustain a traumatic brain injury (TBI) (1). To be diagnosed with a TBI, one must sustain an injury that results in a disruption in brain functioning. Severity of injury ranges from mild (also known as a concussion) to severe and is generally related to the level of brain disruption and damage sustained (2). Every year, approximately 116 000 individuals older than 15 years are discharged from a hospital after sustaining a moderate to severe TBI (3). Individuals with such injuries often live with chronic cognitive, sensory, and physical impairments, as well as decreased participation in all areas of life (4). The present study sought to advance research into the effective long-term care and treatment for people living with TBI through identifying effective strategies for engaging TBI survivors and caregivers as advisors to clinical research.
There are approximately 5.3 million individuals in the United States living with TBI-related disabilities (5). Until recently, many with severe injuries did not live after sustaining the injury. As the first cohorts with such injuries age, TBI is being reconceptualized as a chronic condition, with lifelong health implications for survivors, their caregivers, and health care systems. Research suggests that TBI outcomes dynamically change over the life span (6). Function and quality of life can decline, secondary to progressive neurodegeneration, comorbid physical and mental health conditions, aging, and psychosocial challenges (6). Secondary health conditions arise such as pain, fatigue, obesity, isolation, and depression (7). Acknowledging TBI as a chronic health condition highlights the need to identify patient-centered strategies to facilitate lifelong health.
Despite the recognition that many living with moderate to severe TBI will likely require inventions across the life span, the development of effective interventions aimed at improving patient-centered outcomes across the life span of survivors of TBI has been limited (8,9). A recently completed systematic review to identify “strategies” and “context factors” that optimally enable patient engagement in the design, delivery, and development of health services included very few studies of patient populations who frequently experience cognitive impairments (eg, dementia (10), stroke (11), multiple sclerosis (12)) and no studies of people living with a history of moderate to severe TBI (13). To meet the need for effective interventions in support of the lifelong health of TBI survivors, there has been a call for approaches that address complex variables overtime, integrating acute and post-acute research, as well as employing patient-centered comparative effectiveness research (9) and including those with lived experience in all phases of clinical research (preparation, execution, translation) (14). Furthermore, although there is a growing recognition of the value of patient engagement in rehabilitation science, few methods and resources have been developed to assist individuals with TBI and associated cognitive impairments become fully engaged in different roles and phases of clinical research (15).
The Coalition for Recovery and Innovation in Traumatic Brain Injury Care Across the Lifespan (CRITICAL) brought together patients with moderate to severe TBI, caregivers, clinicians, researchers, and advocates to develop a patient-centered agenda for improving health care across the life span for those living with moderate to severe TBI (16). The CRITICAL not only included patient and caregiver perspectives, but the study presented here examined CRITICAL’s processes to identify techniques to enhance engagement with TBI survivors and caregivers. Although the patient experience is relevant to improving intervention development, translation, and dissemination, it is not enough to involve TBI patients and caregivers in development of a clinical research agenda (17). Emphasized in community-based participatory research (CBPR), patient-centered research demands continued engagement throughout the entire research to practice cycle (18,19). This study applied CBPR methods to identify strategies to improve research engagement with individuals living with moderate to severe TBI and their caregivers.
Methods
Community-based participatory research methods were employed throughout the CRITICAL project, emphasizing shared decision-making and consumer buy-in at all stages of engagement, implementation, and evaluation (17 –19). All phases of the project involved input from the CRITICAL partners, including TBI survivors, caregivers, and professional stakeholders, and the methods and results presented in this article were reviewed by all partners. Through multiple patient engagement, capacity building, and group priority setting methodologies, the CRITICAL was designed to support the participation of those living with a history of TBI (many of whom live with cognitive impairments), and to collaboratively learn from each other how to improve patient engagement for future endeavors.
Participants
Eight TBI professionals (5 female and 3 male participants) were recruited through existing partnerships with the US Veterans Health Administration, TBI Model Systems programs, American Psychological Association Division 22 Rehabilitation Psychology, the Brain Injury Program at Craig Hospital, the Colorado Brain Injury Program, and the Brain Injury Alliance of Colorado. Each TBI professional referred one survivor or caregiver of TBI to participate in CRITICAL. Six survivors of moderate to severe TBI (3 male and 3 female participants) and 2 female caregivers of survivors of severe TBI participated. Inclusion criteria for TBI survivors and caregivers were (1) willingness to volunteer time and energy needed for the workshops and between meeting assignments, (2) motivation to “help others” and “give back something,” (3) successful personal adjustment to the challenges of living with a TBI, (4) adequate insight into personal limitations and strengths, (5) absence of current serious psychiatric problems, (6) an ability to listen, and (7) ability to inhibit personal responses and views or opinions when necessary.
Six of the CRITICAL members were from outside Colorado and 10 were from the local Colorado region. The CRITICAL participants brought lived experience as TBI survivors, caregivers, or professionals working in the field of TBI rehabilitation. Traumatic brain injury professionals attended as part of their professional duties and were not compensated by the project for their time. Survivors of TBI and caregiver stakeholders were compensated for their time at levels roughly equivalent to the hourly pay of professionals ($50/hour).
Procedure
The Coalition for Recovery and Innovation in Traumatic Brain Injury Care Across the Lifespan proceeded through 3 phases for development of the Research Agenda: (1) topic development, (2) question prioritization, and (3) agenda setting. For each phase, participants we expected to (1) review materials prior to in-person workshops, (2) actively participate in in-person workshops, and 3) complete homework tasks between workshops. After each milestone (eg, completion of the first in-person workgroup), investigators met to rereview potential barriers and facilitators to participation. Throughout, efforts were made to structure the process in a manner to engage those with cognitive impairments. Table 1 shows the processes from phase 1 through 3.
CRITICAL Processes, Phases 1-3.

Abbreviation: TBI, traumatic brain injury.
At the beginning of each in-person workshop, the Principal Investigator verbally and visually highlighted project values including mutual respect, the importance of survivors with TBI and caregiver perspectives, shared responsibility, and learning from each other. During the workshops, large posters were placed on the wall in the front of the room listing the phases of the project and providing a simple agenda. The facilitator would repeatedly refer to these posters to remind participants of the overall project phase and highlight progress through the day’s agenda. Moreover, a standing agenda item at the end of each in-person meeting included feedback regarding the process. This feedback was documented in meeting minutes.
Measures
Following each workshop, qualitative interviews were conducted by phone among those participants living with moderate to severe TBI and caregivers (n = 8) to obtain feedback regarding the process. Interviews were conducted within one-week post-workshop. Three interviews were conducted with each TBI survivor or caregiver who attended the workshops, for a total of 23 interviews (one participant missed one interview). Interviews followed a semistructured interview guide with questions designed to elicit feedback on participants’ experience engaging with premeeting review and the in-person meeting, on what went well and what could be improved, and to provide an opportunity for participants to add additional comments on research priorities. Each interview was conducted by 2 research team members—one interviewer and one notetaker. Both the interviewer and note keeper took detailed notes during the interview, including pausing to write down quotes more fully when necessary. After the interview, the notetaker combined the interview notes into a single transcript, and the interviewer reviewed transcripts to ensure accuracy and completeness.
To analyze data on participant engagement, members of this research team reviewed interviews and meeting minutes with the goal of identifying barriers and facilitators to participation for survivors of moderate to severe TBI and caregivers. The team adopted a qualitative descriptive methodology (20) with the goal of summarizing the findings in “everyday terms” reflective of the participants’ experiences. Materials were read by each research team member, and then discussed in a group format. Specific foci included identifying: (1) feedback regarding strategies that had been employed, and (2) additional strategies recommended by participants. It was determined that informational redundancy was achieved (21).
Results
Strategies employed to facilitate participation fell into 3 main categories: (1) Communication, (2) Preparation, and (3) Environment (CPE). Table 2 summarizes results pertaining to participant engagement drawn from thematic analyses of interviews and meeting minutes. Below we further elucidate these results with direct quotes from the interviews with TBI survivors and caregivers.
Strategies to Facilitate In-Person Participation: Communication, Preparation, and Environment (CPE).
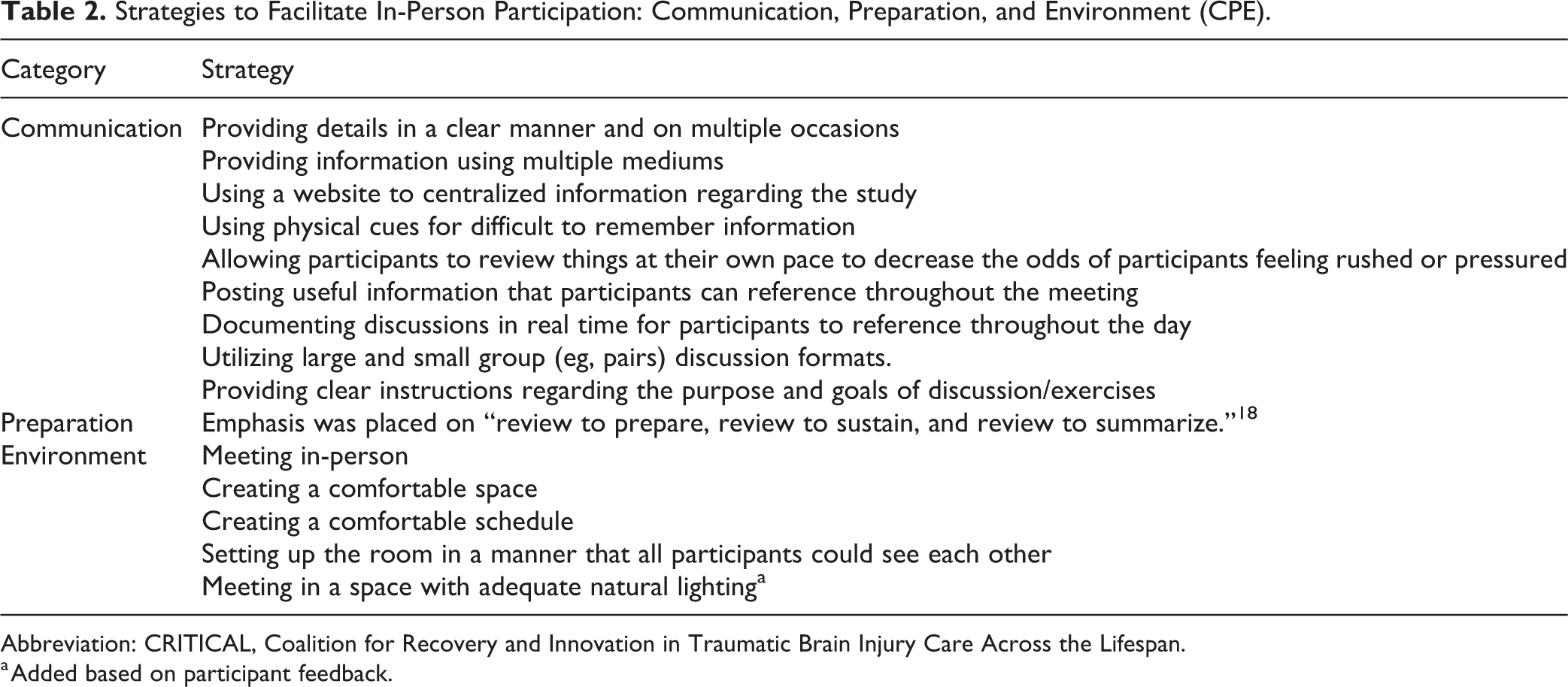
Abbreviation: CRITICAL, Coalition for Recovery and Innovation in Traumatic Brain Injury Care Across the Lifespan.
a Added based on participant feedback.
Communication
Participants commented on the helpful nature of providing information via the computer, as well as hard copies. The CRITICAL study website was identified as an important resource. One individual indicated that the materials were familiar because she went over them prior to the meeting. Several stated that recording content on the flip charts was helpful. “Love all the sticky pads…wall notes…it keeps everything fresh and organized.” Another noted that “saying what information [would follow] was helpful,” (participants were cued at the start of each new discussion topic). Reflecting on the small group discussions (groups were comprised of those living with TBI, as well as professionals), “(They) hooked us up with someone else” so that there was another person to help answer questions regarding the topic at hand. Despite employing multiple strategies to share information, at least one participant had trouble finding the meeting space for the first workshop.
Preparation
Survivors with TBI noted that materials being sent ahead helped them prepare for the in-person meeting. An individual stated that reviewing the materials ahead of time helped them “get in the right mind set.” Several of the participants spoke about challenges with remembering things and stated that having resources to review (eg, meeting minutes) allowed them to go back and review what was previously discussed.
Environment
Participants noted that the in-person nature of the meeting was helpful. In specific, this format was felt to increase focus, participation, and comradery/team building. The first meeting was held in a somewhat smaller room, which did not allow sufficient access for the participant using adaptive equipment. One participant noted, “could have gone to a little bigger room, only because of the wheelchair.” For future meetings, an alternate larger space was identified, and the room was rearranged to accommodate all individual’s access needs. Several participants mentioned that they appreciated the natural lighting in the room, “I liked the windows.” Another noted that the windows “made her feel more open.” Finally, several participants stated that they liked the room set up which allowed for all participants to see each other. “Being able to face everybody helped me feel focused. I felt like I was listened to.”
Participant feedback regarding the process suggested that implementation of the above-stated strategies, as well as identifying and addressing barriers in real time resulted in positive and productive experiences. One individual stated, “I enjoyed it. It was a good experience. We had a good talk. Everyone was able to contribute. I think it went well. I look forward to the next.” This participant went on to note, “I felt like everyone was able to speak their mind I was listened to. If I had something to say, I said it. Everyone was respectful to me. I felt like we had a good bond.” Another participant described their experience as “humbling, in a good way” and noted that being in a room with researchers and clinicians was “amazing.” Whereas as some group members noted that the group of participants could have been more diverse, others highlighted the facilitative nature of the small group format. “Because it is such a personal topic, it needs to be a personal group. Online takes a lot of the personal out, which defeats the purpose.” Summarizing their experience at a workshop one of the participants said, “I’ve never been part of something like this before and was unsure what I was getting into…this was a professional undertaking that could benefit BI [brain injured] folks [which] made me feel good about doing it.” Another said, “I’ve never done anything like the way we did it. I thought how it went was awesome. I’ve never felt like I’ve had such an impact. Having all the professionals in the room with the survivors. I felt like I had an impact on other survivors. I’ve never felt that before.”
Discussion
Despite the fact that TBI has been noted as a significant public health concern, and those with moderate to severe injuries often require long-term care, little research has been done to explore how best to engage those living with TBI in research (15). The CRITICAL formed in August 2017 and met in person 3 times from September 2017 to August 2018, bringing together survivors of TBI, caregivers, and professionals to develop a research agenda to specify the long-term Patient-Centered Outcomes Research needs of TBI survivor and caregivers. In following with CBPR principles, CRITICAL stakeholders were engaged in reviewing materials from September 2017 (prior to the first meeting) through December 2018 and submission of the final project report. The processes employed to advance the CRITICAL’s objectives were carefully designed to enhance and prioritize the voice of TBI survivor’s and caregivers. Through qualitative methods, we examined the CRITICAL’s processes to identify strategies that can effectively engage survivors of moderate to severe TBI and their caregivers in research to improve patient experience. Results from this study indicate that effective research engagement with individuals living with TBI falls within 3 themes: Communication; Preparation; and the Environment.
Within the theme of communication, TBI survivors benefitted from CRITICAL’s deliberate strategy to present important information in multiple formats, as well as having a designated individual to ask clarifying questions of. Through repetition of information across multiple formats, for example, agendas provided in advance via email, in handouts, on flip chart posted to meeting room walls, and repeated verbally, individuals living with TBI were better able to access the information they needed to recall what was discussed previously and keep track of what stage of the project was being worked on. Furthermore, CRITICAL paired up TBI survivors and caregivers with TBI professionals for discussion sessions during each meeting—this strategy supported individuals living with TBI by ensuring they always had an individual they could ask questions of and get assistance from during every meeting.
Regarding preparation, the CRITICAL employed multiple steps prior to every meeting to support participants in being prepared, including providing online training on the topics to be discussed, premeeting review materials (eg, prior meeting notes, agendas, survey results), and premeeting preparation phone calls. Our results suggest that enhanced meeting preparation is important to survivors of TBI in 2 ways. First, it helps them recall and remember where in the process of the project they are and remember prior discussion. Second, it helps them mentally orient and prepare to engage in discussion, that is, to “get in the right mind” as an advisor to research.
Lastly, our results indicate that the physical environment is also a critical domain to attend to in order to promote inclusion and engagement of individuals living with TBI. Of particular note is ensuring that meetings rooms are large enough to accommodate the needs of individuals with disabilities. Survivors of TBI may experience challenges with mobility and balance, requiring larger spaces to be comfortable and safe. Likewise, common cognitive impairments from TBI results in challenges to staying focused or feeling overwhelmed by too much stimulation—attention to open and not cluttered, as well-organized space, helps facilitate engagement. Lastly, TBI participants identified room set up to facilitate seeing each other as critical to helping keep track of the discussion and being able to see others when they speak.
This study, however, is also not without important limitations that must be mentioned. First and foremost, this was a relatively small sample size and qualitative study. Similarly, we examined only our predefined process, and therefore cannot speak to the effectiveness of these strategies for other study types, goals, or participatory processes. Therefore, future research should seek to validate these findings in larger samples and more diverse study contexts. Also, although a relatively diverse group of individuals with moderate to severe TBI participated in this process; the group lacked membership from many minority communities and only included caregivers who were spouses of individuals with severe TBI. Additional efforts are indicated to explore and expand upon identified strategies to evaluate their applicability across different demographic groups, and especially with diverse types of caregivers.
Conclusion
The World Health Organization International Classification of Functioning, Disability, and Health (ICF) (22) can be used to classify functioning and disability using the constructs of Body Functions and Structures, Activities, and Participation (23). The ICF framework also facilitates evaluation of contextual factors including those that are Environmental and Personal (23). According to the ICF impairments in Body Functions (eg, cognitive impairment post-TBI) can be mitigated via the use of Environmental Structures, as well as Activities and Participation (eg, project communications and preparation activities). Use of CPE strategies identified in this study align with the ICF and facilitated engagement among participants living with TBI and TBI sequelae (eg, memory difficulty, problems with initiation and organization).
To meaningfully engage those with TBI in research, additional resources will be likely be required (24). Additionally, participants discussed the positive personal impact of being a part of the above-described scholarly endeavor. Previous work by Brenner et al (25) regarding suicide among those with TBI, highlighted loss of sense-of-self as a risk factor, and having a sense of purpose as a protective factor. CRITCIAL’s stakeholders suggested that incorporating the perspectives of those living with TBI during all stages of the research process may be beneficial to TBI professionals, as well as the larger community of individuals living with TBI. Employing strategies such as those outlined in this article is expected to promote patient engagement, which in turn promises to improve the development, identification, translation, and dissemination of patient-centered interventions and outcomes for individuals living with TBI.
Supplemental Material
Supplemental Material, sj-pdf-1-jpx-10.1177_2374373521998852 - Engaging Those Living With Moderate to Severe TBI and Their Caregivers in Research
Supplemental Material, sj-pdf-1-jpx-10.1177_2374373521998852 for Engaging Those Living With Moderate to Severe TBI and Their Caregivers in Research by Nathaniel V Mohatt, Carlee J Kreisel, Lisa A Brenner and the CRITICAL Team in Journal of Patient Experience
Footnotes
Authors’ Note
Nathaniel V. Mohatt, Veterans Health Administration Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention (RMIRECC); Department of Physical Medicine and Rehabilitation, University of Colorado Anschutz Medical Campus; and Division of Prevention and Community Research, Department of Psychiatry, Yale University School of Medicine. Carlee J. Kreisel, RMIRECC and Department of Physical Medicine and Rehabilitation, University of Colorado Anschutz Medical Campus; Lisa A. Brenner, RMIRECC and Departments of Physical Medicine and Rehabilitation Psychiatry, Psychiatry, and Neurology, University of Colorado Anschutz Medical Campus. The Coalition for Recovery and Innovation in Traumatic Brain Injury Care Across the Lifespan (CRITICAL) included Julia Terlinchamp, Cindy Ashworth, Mark J. Condon, Ivonne Thompson, Lenore Hawley, Jody Newman, Judy Detmer, Gavin Attwood, Joel Scholten, Dawn M. Ehde, Nazanin Bahraini, John D. Corrigan, and 4 other members. Dr. Brenner consults for sports leagues. The views, statements, opinions presented in this publication are solely the responsibility of the authors and do not necessarily represent the views of the Department of Veterans Affairs, the United States Government, or the Patient-Centered Outcomes Research Institute® (PCORI®), its Board of Governors, or Methodology Committee. Correspondence concerning this article should be addressed to Nathaniel Mohatt, Ph.D., Department of Physical Medicine and Rehabilitation, University of Colorado Anschutz Medical Campus, Aurora, CO, USA. Phone: 720-788-2184. Email:
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded through a Patient-Centered Outcomes Research Institute® (PCORI®) Eugene Washington PCORI Engagement Award (3908-UCD), and is based on work supported, in part, by the Department of Veterans Affairs.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.