
Abstract
Nonadherence to iron chelation therapy (ICT) remains a long-standing and serious issue in thalassemia, especially in resource-constrained developing countries. Barriers and facilitators of adherence to ICT in transfusion-dependent thalassemia (TDT) adult patients in Malaysia are not completely understood. This qualitative study explored factors affecting adherence to ICT among TDT adult patients at a public tertiary hospital in Malaysia. Data were collected through 21 semistructured in-depth interviews conducted among purposively sampled patients using a pretested interview guide. All interviews were audio-recorded and transcribed verbatim. Data were analyzed manually using thematic analysis method and managed using Atlas.Ti software. The most frequently discussed subthemes of barriers to adherence included patient-related factors, medications-related factors, sociocultural-related factors, environmental context and resources, and patient–health care provider relationship factors. The facilitators to adherence included having insights of their illness, prevailing sources of motivation emphasizing on strong self-efficacy, low medication burden, and having enabling environment. This study has identified barriers and facilitators that are unique to Malaysian thalassemic adults related to medication adherence. Options for future multifaceted interventions are suggested.
Keywords
Introduction
Thalassemia is the most common inherited monogenic hemoglobin disorder worldwide (1). An estimated 7% of the world population is a carrier for this disorder, and approximately 60 000 children are born with the severe type of thalassemia each year (2). The mainstay management for these patients includes regular blood transfusions and iron chelation therapy (ICT). Iron chelation therapy is used to prevent iron overload to numerous vital body organs (3). Currently, there are only 3 iron chelators licensed for clinical use, namely, deferoxamine, deferiprone, and deferasirox. Advancement in blood transfusions and ICT transforms this disease from fatal childhood disease to adult chronic disease (1). Numerous studies have reported that advancement in medical care and good adherence to ICT treatment are instrumental to increase patients’ survival and quality of life (4 –10).
Nonadherence to ICT remains a long-standing and serious issue in thalassemia (11). Worldwide, nonadherence rate to iron chelators ranges from 30% to 80% (6). Issue of nonadherence to ICT is complex and multifactorial (9 –13). It has been established that nonadherence to ICT increases mortality and morbidity, reduces quality of life, and incurs huge economic burden to the country (14 –16). However, most of these studies were conducted in developed countries and among younger patients (17 –19). In Malaysia, suboptimal ICT adherence among thalassemia patients remains a persistent problem, and limited studies have explored this issue (20). Thus, this study aimed to explore barriers and facilitators to treatment adherence among transfusion-dependent thalassemia (TDT) adult patients in Malaysian population.
Participants and Methods
Study Design
This study used qualitative methodology, adopting phenomenological approach, through semistructured, face-to-face in-depth interview with purposively selected participants. Qualitative methodology was deemed the most appropriate method to explore in-depth experience and perception of study participants (21,22).
The participants were enrolled from a transfusion day care and outpatient thalassemia clinic of a public tertiary hospital. It is the national hematology referral center, serving the largest number of adult TDT patients in Malaysia. This study was carried out according to the principles stated in the Helsinki Declaration and approved by the medical research and ethics committee of the Ministry of Health, Malaysia (NMRR-19-73-45840).
Participant Selection
A purposive sample of adult (aged ≥18 years) TDT patients and taking any types of ICT was included in this study. The following participants were excluded: persons with impaired cognitive abilities and persons who were unable to understand or speak either English, Malay (the national language), or Mandarin language. Participants were selected from both genders, diverse races, and religious and socioeconomic background for maximum variation. Participants who agreed to participate voluntarily and signed the written consent form were assured of their anonymity and confidentiality throughout the research. All research-related data were kept in a password-protected database, and result findings were solely presented in deidentified terms.
Development of Interview Guide
An interview guide containing a list of predetermined open-ended questions was developed, based on the objectives of the study. The interview guide was independently reviewed and validated by an expert in thalassemia and 2 experienced qualitative researchers to ensure the development of meaningful questions that will motivate relevant responses. A pilot study was conducted on 3 patients to improve consistency and to ensure the interview questions were clear and relevant.
Data Collection
The face-to-face semistructured interview was conducted in English, Bahasa Malaysia, or Mandarin languages, according to the participant’s preference by a researcher who is fluent in all 3 languages. Individual interviews with patients were conducted in a private room to ensure confidentiality. Ice-breaking was initiated to establish rapport. The average time for each interview session was 45 minutes. Probing questions were asked to reduce ambiguity and to further explore the participant’s answers in depth. The researcher periodically summarized the information received and clarified with the participants to determine accuracy. A reflective journal was maintained after each interview. All interviews were audio-recorded and transcribed verbatim. Where necessary, a follow-up interview was conducted to reexamine certain issues in light of emerging ideas.
Through circular approach, a total of 21 participants were recruited, based on data saturation (23). Data were collected until no new themes were identified and no new information was forthcoming. Throughout the data collection process, ongoing data analysis occurred concurrently.
Data Analysis
Data were analyzed manually using thematic analysis method (24) and subsequently managed using both Atlas.Ti version 7.0 software. Transcripts were re-read multiple times, with notes taking at the margins. Memo-taking was done simultaneously to capture reflections and general idea about each interview transcript. Coding was performed line by line inductively (25). Each new code was entered into a codebook indiscriminately at first, and subsequently codes were then collapsed by removing overlapping codes. Codings from transcripts were compared to the list and finally categorized into similar, meaningful units called themes. These themes were then carefully listed, checked, compared constantly, and finalized. The main researcher conducted this coding and thematic analysis independently. To ensure consistency and reliability of the findings, 2 researchers reviewed and verified the codings and themes generated. During the event of discrepancy, the opinions of all research team members were sought and consensus obtained to finalize the themes and quotes representing the themes.
Rigor of Study
To ensure trustworthiness of data, peer debriefing and analytic triangulation were conducted throughout the research with skilled researchers. Upon study completion, findings were shared with a few participants to affirm the accuracy and completeness of the findings.
Results
The mean duration of the interview was 45 minutes (range from 27 to 73 minutes). Majority of them were females (n = 13), young adults (mean age = 31.8 years; range = 21-47 years old) and had received education above secondary school (n = 16). Patients were predominantly single and staying with family. Most of them were from the lower middle-income bracket (n = 16). Two main categories emerged from the interview: barriers to adherence (Figure 1) and facilitators to adherence (Figure 2).
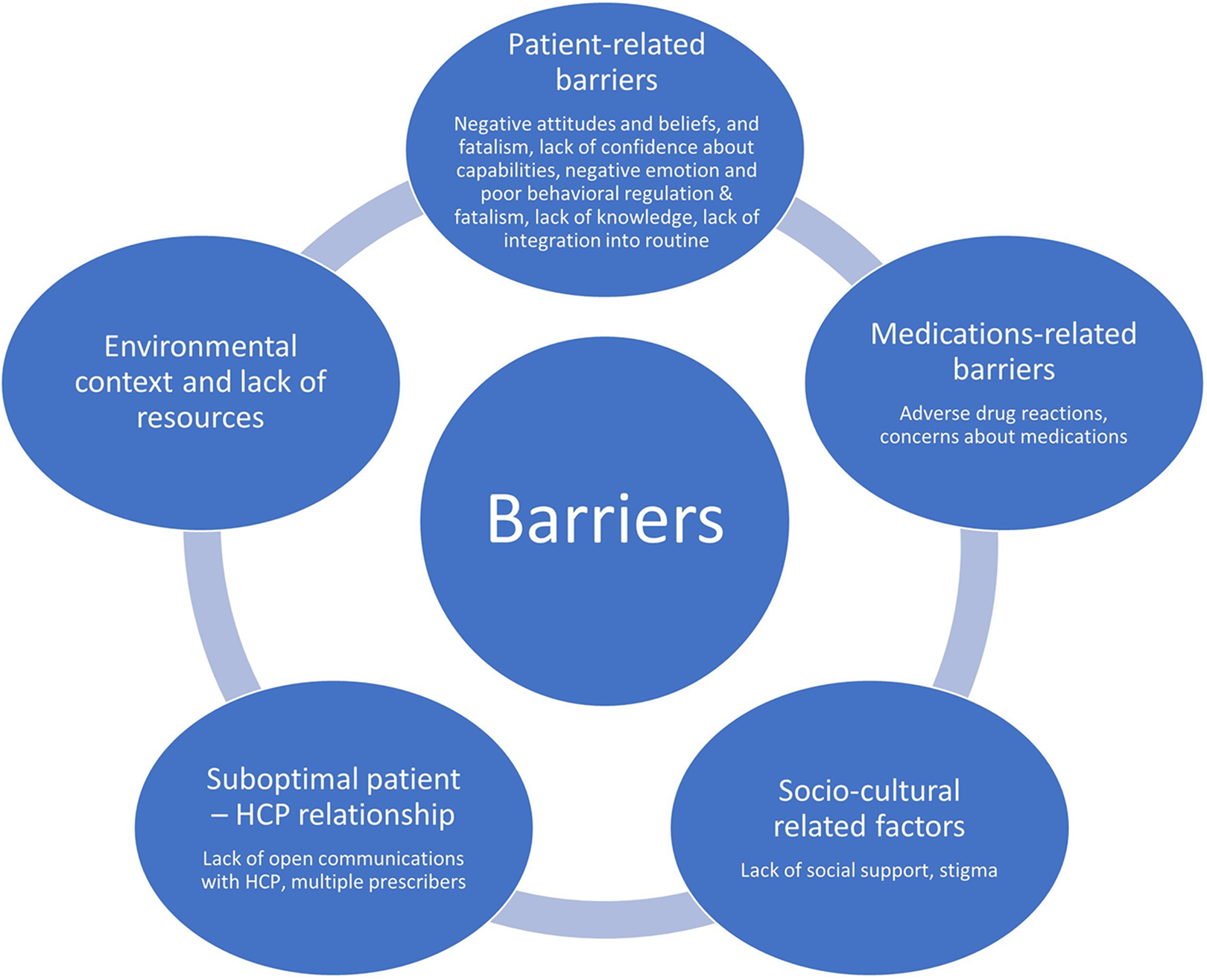
Diagram showing the themes and subthemes of the barriers to medication adherence.

Diagram showing the themes and subthemes of the facilitators to medication adherence.
Barriers to Adherence
Five main subthemes of barriers to adherence (patient-related factors, medication-related factors, sociocultural-related factors, patient–provider relationship factors, environmental context and resources) emerged from the patients’ interviews (Table 1).
Themes, Subthemes, and Exemplar Quotations for Barriers to Iron Chelation Therapy Adherence Among Transfusion-Dependent Thalassemia Adult Patients.

Abbreviation: AIDS, acquired immune deficiency syndrome.
Theme 1: Patient-related barriers
Five subthemes emerged in the patient-related barriers theme. Each of these subthemes is described in detail below without any specific hierarchy/order.
Negative attitude, beliefs, and fatalism
A few participants reported that they strongly dislike using the infusion pump as the injection caused damages to their skin and affected their sleep. Another participant narrated that he did not believe the ICT is effective due to unmatched outcome expectancy. A few participants also expressed fatalistic beliefs, particularly in areas of developing iron overload complications and mortality.
Lack of confidence about capabilities
A few of the young adult participants mentioned having no confidence to self-administer deferoxamine infusion. They felt this lack of confidence originated since their childhood, when they were being shielded from taking up responsibilities for their therapy by overprotective parents.
Negative emotion, poor behavioral regulation, and fatigue
A few participants described prevalent emotional distress and overt negativity that comes from having thalassemia, perpetuating their feeling of hopelessness. These participants claimed that negative emotions and fatigue during period of low hemoglobin further dampened their motivation to handle challenges. Therefore, they revealed adopting avoidance coping style to avoid dealing with the stressful situations in their lives. These underlying psychological constructs are important aspect of nonadherence to ICT.
Lack of knowledge
A few participants stated lack of understanding of the disease and drugs including the skills for correct medication administration and synergistic effect of different iron chelators.
Lack of integration into routine
A few participants discussed their struggles to integrate the time-consuming medication regimen into their daily routine due to their hectic life. This was observed among participants who are working, having small children, or juggling heavy family commitments.
Theme 2: Medication-related factors
Medication-related factors were the most frequently mentioned barriers (85.7%) and consisted of 2 main subthemes, mainly adverse drug reactions and concerns about medications.
Adverse drug reactions
The majority of participants reported that they had experienced significant life-disturbing adverse drug reactions with ICT, causing them to withhold, alter, or skip the medications. A few participants experienced uncommon side effects, which include mood changes, impaired cognitive abilities, and unpleasant burning sensation.
Concerns about medications
Participants described perceived high burden to deferoxamine and oral ICT therapy as reason for medication nonadherence. Most participants consumed an average of 5 types of medications on top of iron chelators, further predisposing them to drugs-related problems. Many participants also expressed concern about their medications, including that oral ICT may cause kidney damage, when taken for long term. Some believed that oral ICT has “heaty” effect on the body, thus should not be taken when feeling unwell.
Theme 3: Sociocultural-related factors
Lack of social support and stigma were constructs that emerged as sociocultural-related barriers to adherence.
Lack of social support
A few participants claimed lack of social support, particularly from influencing figures such as the parents, was found to discourage them from persisting with their medications.
Stigma
A few participants described their day-to-day interaction with others and revealed fear of stigma made them conceal their disease condition to others. Subsequently, participants intentionally refrained from taking medication in front of others, leading to missed doses.
Theme 4: Patient–provider relationship
There were 2 subthemes identified in this category: lack of open communications with health care providers and multiple prescribers.
Lack of open communications with health care providers
Participants highlighted that doctors with stoic facial expression who were paternalistic tend to discourage them from attending future clinics appointment. They developed mistrust when their doctors were reluctant to disclose the laboratory results or were not open in understanding reasons they cannot adhere fully to treatment.
Multiple prescribers
Participants reported that having multiple prescribers reduced rapport between patients and health care providers. Participants felt frustrated having to constantly repeat the same clinical history to different prescribers each time.
Theme 5: Environmental context and resources
Environmental context and resources refers to the circumstances of a person’s situation or environment that influences the person’s behavior. Almost 95% of participants claimed not taking ICT if they go overseas travelling, travel out of home during festive seasons, or attend social functions. Reasons given were obligation for socially desirable behavior during festival gatherings and concerns of environmental cleanliness for infusion. Some participants reported episodes of nonadherence during period of unfavorable life situations, such as during trauma or time of crisis. Majority of participants lamented the high cost of purchasing consumables (syringe, newer needles, alcohol swab) for deferoxamine infusion posed monetary burden to them. Consequently, participants will self-adjust their doses or administration frequency to reduce the cost.
Facilitators to Adherence
Four major categories were identified: having insights of the illness, prevailing sources of motivation, low perceived medication burden, and an enabling environment (Table 2).
Themes, Subthemes, and Exemplar Quotations for Facilitators to Iron Chelation Therapy Adherence Among Transfusion-Dependent Thalassemia Adult Patients.

Abbreviation: ICT, iron chelation therapy.
Theme 1: Having insights
Participants who had insights of their illness knew the necessity of ICT, had good awareness of the complications of iron overload, perceived effectiveness of ICT either through outcome experienced by self or others, understood the synergistic effect of combination therapy, and appreciated the value of medicine.
Theme 2: Prevailing sources of motivation
Participants illustrated that they were motivated to persist with their treatment regimen through narratives of having strong self-efficacy, living for significant others, having positive reinforcement, having goals, having positive identity, and being optimistic.
Self-efficacy
Patients who possessed high self-efficacy were able to persevere with the treatment despite facing setbacks. Among the characteristics described were planning ahead, resilience, sense of capability, having positive emotion, high discipline, emotional management, fighting spirit, self-determination, problem-solving skills, making adjustments, and taking initiatives. Even if they faced periodical lapses in adherence, such as having local injection site reactions or in times of personal crisis, they were able to quickly recover their sense of efficacy after these setbacks.
Living for significant others
A few participants reiterated that they drew strength from having the purpose to live for their significant others or for other purposeful endeavors including voluntary work. The hope of starting a family is a strong motivator for many female patients to be adherent to their treatment. Female participants were aware that therapeutic iron level might lead to better pregnancy outcome.
Positive reinforcement of minimal therapy when iron level is under control
Patients looked forward to needing only minimal therapy if they can get their serum ferritin level within the target range.
Having goals
Participants mentioned when they were able to set small goals for themselves and achieved it, that aided to their sense of accomplishment. Participants suggested incentives such as organizing a competition to reward patients who were able to lower their serum ferritin the most. Participants who have life goals, which include getting married, being successful in career, pursuing their hobbies, were more likely to persist with therapy.
Positive identity and optimism
Participants felt they are “normal,” despite having thalassemia. They were motivated to keep their iron level under control to avoid changes in their outer appearance and skin bronzing, so they may also look “normal” to others. Participants also narrated being hopeful for better treatment in the future and staying optimistic.
Theme 3: Low medication burden
Most patients (66.7%) claimed that being compatible with the medications, having alternative infusion regimen, and having readily constituted deferoxamine or shorter infusion needle can lower the perceived burden from medication use.
Theme 4: Enabling environment
Social support and modeling
Majority of participants stated that good social support, particularly family support, is the pillar for good medication adherence. Quite notably, the construct of having a peer role model as facilitator highlighted the importance of support group and modeling. In addition, flexible working environment was also quoted as an enabling factor for better medication adherence.
Good patient–health care provider relationship
Participants reported that good rapport with health care providers, open communication between patient and health care providers, clear charting of treatment plan in health records, and honesty in broaching difficult topics helped patients feel involved in their health management.
Discussion
To the best of the researcher’s knowledge, this is the first study conducted in Malaysia to explore both the barriers and facilitators to medication adherence among TDT adult patients using qualitative methodology. In line with Leventhal’s Common-Sense Model (26), it is increasingly important to understand patient’s perspectives of their illness condition that may influence their medication taking behavior, so health care policy makers can respond more appropriately.
Our study highlights that barriers and facilitators to ICT adherence are multidimensional. The elimination of certain barriers, specifically modifiable factors, can help patients to better adhere to ICT. Heightened understanding of facilitators, especially in self-efficacy and motivation, provides interesting options for future strategy. Most of these subthemes can be further explored in future researches.
Patients-related barriers are the most reported barriers with strong emphasis at deficit of psychological capacity and motivation, particularly low perceived self-efficacy, to engage in medication adherence behaviors. This is reflected by participant’s lack of confidence in their capabilities to self-administer complex regimen and to self-regulate complex emotions. Many studies supported that self-efficacy has mediating role in medication adherence, through development of multidimensional resilience, even among patients with psychological problems (27 –29). It is one of the most important acquired skills for patient empowerment to self-manage the various facets of their complex illnesses (30). It is worrying that many young adult participants in this study have basic cognitive knowledge but have low perceived self-efficacy. The possible reason includes conventional thalassemia patient education is more cognizant based, mainly focusing on information giving and techniques teaching. This emphasizes the need to include pragmatic self-management interventions and programs as advocated by World Health Organization to empower persons with chronic illness to manage their health and health care (31).
High level of concerns about medication and suffering from adverse drug reactions emerged as the most compelling medication-related barriers to ICT adherence. Asian patients had higher levels of concern about chelation compared to white patients (13). According to Necessity-Concern Framework, unaddressed high concerns about medications predispose patients to problem of nonadherence (32). The occurrence of drugs-related problems, specifically adverse drug reactions, is disruptive to patients’ quality of life and affects their adherence, evident from the many studies conducted among thalassemia patients (4,6 –8). It is, therefore, important to address not only patients’ knowledge but also their beliefs and concerns about medications, as emphasized by the UK National Institute for Health and Care Excellence (NICE) (33). Pharmacists play strategic role to recognize and to address these medications-related barriers commonly associated with iron chelators. Addressing these concerns may require a more in-depth, nonconfrontational and collaborative approach, such as through motivational interviewing (34,35), while supporting efforts to enhance patient’s perceived self-efficacy on symptoms management.
This study also highlighted the theme of enabling environment, particularly good patient–health care provider relationship and social support and modeling, in facilitating chelation adherence. According to COM-B framework, improved patient–health care provider relationship can provide the environmental and social influence that enhances opportunity for medication adherence (36). Patients are more likely to disclose to their physicians important information such as their concerns and self-adjustments made to their medications when positive therapeutic alliance is formed (37,38). This finding emphasized the need of concerted effort to strengthen patient–health care provider relationship and to align current practice with person-centered approach advocated by organizations such as NICE (39,40). Participants also highlighted the importance of role models and patient group. The establishment of a holistic specialized multidisciplinary adherence program, incorporating health-coaching initiatives, may be beneficial in this aspect.
There are some limitations to this study. Patients who refused to participate and those who could not speak English, Malay, or Mandarin language might have other important barriers or experiences that were not captured in this study. Being an interview-based research, social desirability and recall bias can undermine the quality of the data. However, this methodology is best to elucidate participant’s perspectives and provide richer spectrum of barriers and facilitators encountered.
Conclusion
This study provides insights into various influencing factors of medication adherence for Malaysian TDT patients contextual to the local setting. Understanding of barriers and facilitators to ICT among these patients provides interesting options for future multifaceted interventions.
Footnotes
Authors’ Note
This study was approved by the medical research and ethics committee of the Ministry of Health, Malaysia (NMRR-19-73-45840).
All procedures in this study were conducted in accordance with the medical research and ethics committee of the Ministry of Health, Malaysia, approved protocols.
Written informed consent was obtained from the participants for their anonymized information to be published in this article.
Acknowledgments
The authors thank Hospital Ampang for providing the facilities to conduct this project as well as hematology nurses at the specialist clinic and thalassemia daycare center for their help.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.