
Abstract
The primary goal of patient and public involvement (PPI) in healthcare is to improve individual and population health outcomes. This study reports on the successful training of patients to be involved in patient education as peers and clinical research at Grenoble Patients’ School (GPS). GPS was founded by patients as an independent association to train patients to the above objectives tasks. The training team was multi-professional and included expert PPI who were part of the professional team. Medical faculty members and 45 patients, 59% females, 52 ± 6.4 years old, trained between 2016 and 2017, showed high satisfaction at the end of the training courses. Almost all the trained patients were involved as peer educators and 4 were involved in clinical research projects at different stages under the guidance of medical teams. Patient involvement at GPS provided strong benefits to trainees and had some impact on education and obtaining research grants. The outcome of this patient training program resulted in the creation of a Patients’ Department within the Medical and Pharmacy Schools at the Université Grenoble Alpes in 2020, https://medecine.univ-grenoble-alpes.fr/departements/departement-universitaire-des-patients/.
Keywords
Introduction
The main and benefit of patient and public involvement (PPI) in healthcare is to improve individual and population health outcomes (1,2). This public and patient involvement (PPI) is accompanied by a paradigm shift in the way health education and clinical trials are viewed as activities that are done “with” or “by” patients or the public rather than “to,” “about,” or “to” them (1). The most integrated model is the co-called Montreal model where patients are true partners whether in care, in the organization and delivery of health services, in teaching, and in research (3). For PPI in health education, it ranges from the creation of teaching materials to a formal position in a medical school, according to a proposed 6-level scale (4,5). In France, patients are allowed to intervene in multi-professionals health education programs as partners if they have completed the so-called 40-h session for health educators. In the field of clinical research, there is increasing evidence that clinical trials have difficulty attracting and retaining patients for the duration of trial (6). PPI in health education and clinical trials has been one of the ways to address the above problems. Indeed, PPI can be involved in recruiting patients for clinical trials, developing clinical protocols with clinicians, participating in ethical review, or steering committees with medically qualified staff.
In the United Kingdom, the number of PPIs has significantly increased as it is associated with funding procedures whereas, in the United States and Europe, initiatives are rare and not a priority in the universities studied (4). Among the many barriers to the PPI in teaching and research (1) are poor medical literacy and a potential lack of training in healthcare (4).
There is strong evidence that PPI is associated with a high degree of satisfaction among peer educators, patients, and health professionals, while short- and long-term benefits in healthcare are at this stage being less assessed (4,7,8). Networks such as those involved in mental health (9), the National Health Service in the United Kingdom (2) or the Haute Autorité de Santé in France (10) indicate the added value of having PPI in education, guidelines development, clinical trials, and research. However, they do not provide much detail on whether and how PPIs are trained. Indeed, publications on PPI training are rare and the first to do so were on arthritis education (11–14). In France, patient schools within or outside Universities training PPIs in health care were founded in Paris in 2009 (15), Marseille in 2012 (16), and Grenoble in 2014. However, reports on PPI recruitment and training are scarce (14).
This publication aims to report the successful training of PPI in health education and clinical research at Grenoble Patients’ School (GPS) to subsequent intervention as peer educators. A primary objective was to evaluate the success of this training based on the satisfaction of trainees and faculty members including PPI experts. A secondary objective was the impact that trainees had on education and clinical research.
Methods
History of the GPS
GPS was created as an association on October 6, 2014, following the law of 1901 (17) in Grenoble. The founders were 5 patients, headed by the first author of this manuscript, a patient with a long, continuous, and strong history of commitment to healthcare and to democratic values in healthcare. The President of the Université Grenoble Alpes (UGA), as well as the Deans of Medicine and Pharmacy schools of the UGA, the Director of Centre UGA (CHUGA) were implicated from the beginning in helping GPS. GPS remained independent from UGA and CHUGA.
Selection of Patients Trained at GPS
Patients were invited to join GPS training programs through the internet, magazines, patient associations, or their health professionals. These volunteers showed a clear willingness to join GPS to help patients and were interviewed individually to be accepted into the program. As long as no personality or psychiatric problems were identified or raised during the interview, they were accepted as volunteers. Patients with a history of mental health and psychiatric disorders were interviewed in more detail to ensure that they could complete the training and volunteer task. No qualifications were required of the patients and their own experiences in health and social fields were the most important criterion. Most applicants’ fees were funded by public health agencies or patient organizations and honoraria were available for the teachers outside UGA or CHUGA.
GPS Training Programs
Two training programs were available for the patients in the health field (Tables 1 and 2). The first in the field of chronic somatic disease was entitled: Becoming a peer educator for chronic somatic conditions, Table 1, and the second in the field of mental health was entitled: “Becoming a peer educator in mental health,” Table 2. In both programs, patients received training in peer health education. They were introduced to the French health system and the rights and obligations of patients. This was followed by principles of health communication, training, and education through slide shows, publications, and multiple exchanges. Teaching techniques, mostly borrowed from patient education techniques (18) involved the use of photographs, flowcharts, narrative practices, forum theatre, websites (19), and facilitation methods. These teaching tools were used either in plenary sessions or in small groups (18). Validation of the training required participation in all courses and presentation of the health educators’ projects to all students and the teaching staff.
Becoming a Peer Educator for Chronic Somatic Conditions in GPS, Syllabus and Teaching Tools.

Becoming a Peer Educator in Mental Health, Syllabus and Teaching Tools.

Becoming a Peer Educator in Chronic Somatic Conditions
The objectives were to (Table 1):
Discover the goals and methods of empowerment and education for patients with chronic somatic diseases. To accompany the health education in their future project during the 4 modules with a shared plenary presentation of each personal future health educator project on day 8. Offer to follow an additional university course if necessary at the UGA. Promote social reintegration through participation in health education, patient associations, initial, or continuous education, public institutions such as hospitals, universities, or health public agencies. The teaching team was multi-professional and included experts patients, members of GPS, the Transversal Unit for Therapeutic Patient Education (UTEP) of the CHUGA (20), the French-speaking Association for the Development of Therapeutic Education (Afdet) (21), the network for prevention, accompaniment and therapeutic education of liver diseases (Prométhée) (22) and teachers from the CHUGA (23) and the UGA (24). Teaching was organized around 4 modules of 1 to 2 days, plus a 2-day training session on setting up a health educator project, all within 4 to 6 months. The participants worked mainly in small groups and experienced different facilitation techniques that they will use when involved in patients education (18,19).
Becoming a Mental Peer Educator
The objectives were to (Table 2):
Acquire personnel skills like active listening and motivational interviewing. Act in a collaborative project as a peer in mental health networks as a carer or as a research participant. The teaching team was again multi-professional including PPI expert from GPS and the Centre Ressources Métiers et Compétences en Psychiatrie (25). Teaching was organized over 11 independent days plus 2 days of training sessions related to the peer educator project of the future students. All was delivered within 6 months. The items and themes were partially common with the previous program concerning facilitation, exchanges techniques, and the potential of peer education in mental health. Specific themes included the unique role of PPI alongside health professionals, the value of shared experience between PPIs and patients. PPIs contributed to the destigmatization of mental illnesses or disorders, developed an understanding of mental health recovery, and promoted recovery based on their own experience, Table 2.
Course Evaluation by Trainees and Faculty Members
We conducted a one-line survey to assess trainee and faculty satisfaction. We also a specific survey on of trainees’ new commitments after their training. Everything was done in compliance with the regulations on the security of personal data rules at CHUGA. Questions to trainees dealt with their profiles as age, gender, knowledge, and practice of patients’ education before and after training. Satisfaction with the course, current, and future involvements according to the 6-level scales (4), a choice to take additional academic courses at UGA were assessed. Free comments were encouraged. Fort the faculty members, additional specific items were asked to their professional situation, the student selection process, and their involvement in the courses.
Participation in Research
Members of the UGA faculty were asked to volunteer to participate in various research projects. It varied from defining objectives, design, collection of data, and participation in analysis and/or dissemination of results as expected in an ongoing trial where patients were involved in all stages (26).
Ethics
Written and informed permission to conduct such a survey was obtained from the legal authority in charge of data protection and confidentiality at the CHUGA. Everything was done in compliance with the regulations with the CHUGA regulations on personal data security.
Results
Patient Participation and Satisfaction with the GPS Training Courses
A total of 45 patients were trained between 2016 and 2017, 35 attended the program “Becoming a peer educator for chronic somatic conditions at GPS” within 4 classes of 8 to 9 students. Ten students followed the program “Becoming a peer educator in mental health” in one class.
They were 45 students, 52 ± 6.4 [26–71] old, 59% female, some retired, most were unemployed due to disability; they were from Isère 59%, Savoie 11%, and Lyon 11%, France. Out of 45 participants, they were 3 drop-outs during the course, 1 death after the course, we lost track of one of them and one did not wish to participate in the course survey. A total of 24 students out of 40 that were contacted completed the online survey after 2 reminders. Students approached the GPS through either website, magazines, or personal relationships in 27%, or with patient associations in 52%, or 31% after the advice from health professionals. The satisfaction of both participants and faculty was very high, Table 3. Verbatim reports from students and faculty were reported; see representative ones in Online Supplemental Material.
Satisfaction of Patients Trained and Teachers of the Grenoble Patient School Centre (GPS).

Results are expressed in % of 24 out 45 trained patients and in 8 out 12 faculty members.
Involvement of Trainees Before and After Their Participation in GPS
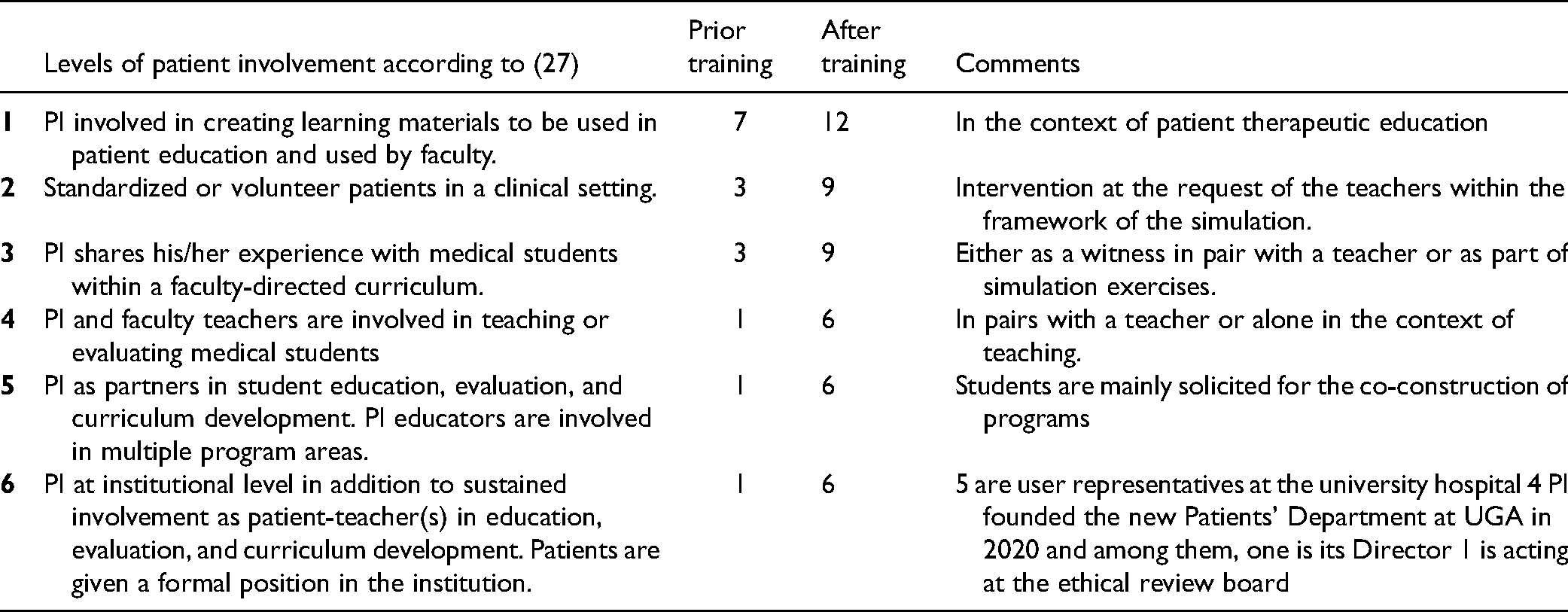
Before training, 16 patients were involved mainly in patient education, and most of them after training were involved in educational/research activities. After training, 5 patients reached the “highest level” according to the 6-levels PPI classification in health education (27): one as an active member at our institutional review board and 4 in the new UGA medical and pharmacy school patient department https://medecine.univ-grenoble-alpes.fr/departements/departement-universitaire-des-patients/ opened by the end of 2020 thanks to the success of GPS (Table 4).
Changes in Patient Participation Before and After Training at the Grenoble Patients School Centre.
PI in Research
Four students and almost all patients’ faculty members at GPS have contributed to research projects at different stages. Representative examples are displayed in Table 5 among increasing solicitations.
Patients’ Participation in Collaborative Research Projects After GPS Training.
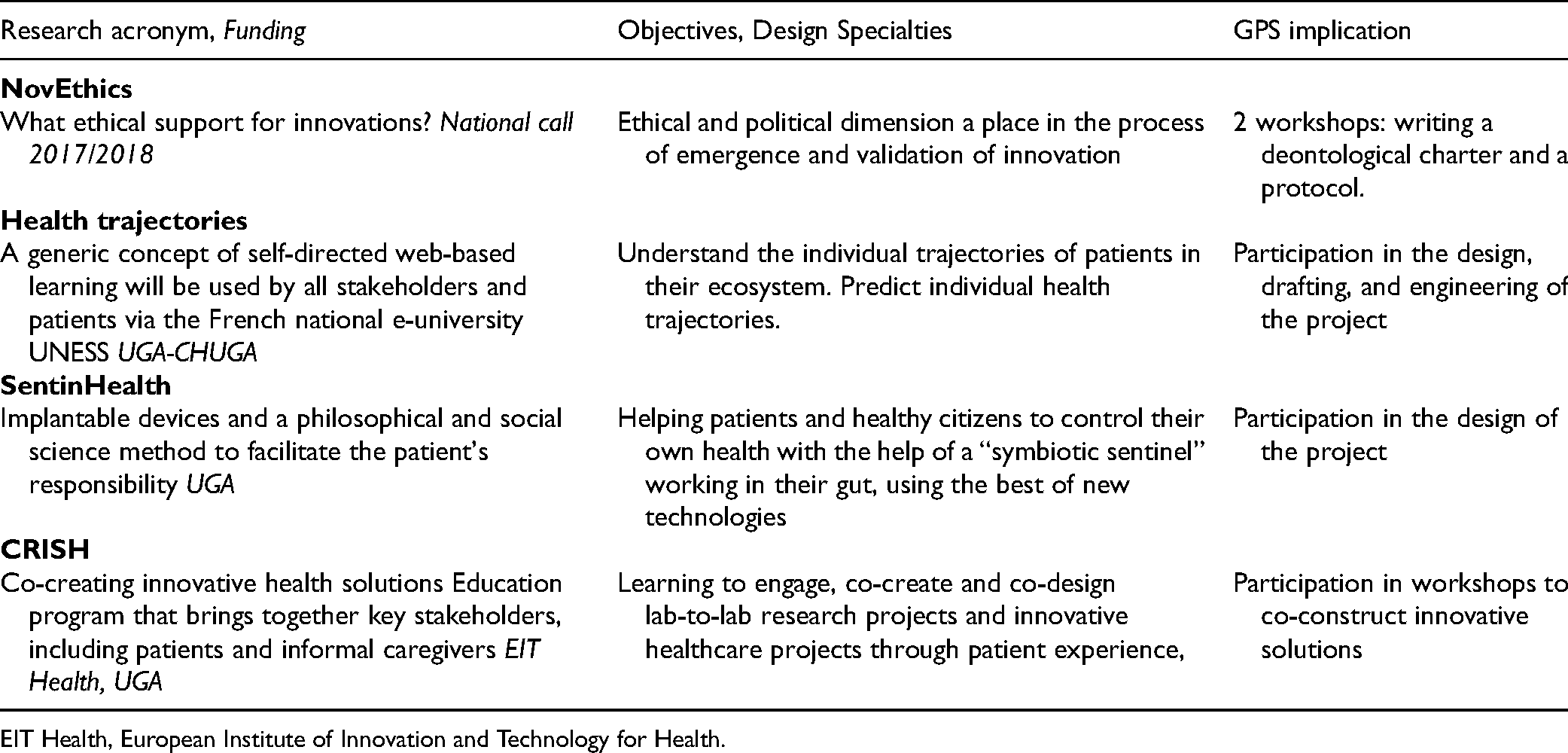
EIT Health, European Institute of Innovation and Technology for Health.
Discussion
This study showed the success of training PPI to become peer educators in somatic chronic and mental conditions within GPS. GPS was an independent association founded by patients and linked to UGP and Centre Hospitalier Grenoble Alpes. Training the first 45 PIs was very successful with a high degree of satisfaction from the trainees and the teaching staff. In addition, thanks to these 2 training, PPI has significantly increased their interactions with patients in the field of health and mental education. A new PPI department was created in 2020 within the UGA Schools of Medicine and Pharmacy following this successful PPI training and its significant results.
It is now recognized that PPI is essential to improve the quality and efficiency of health systems (1–4,27,28). To support PPI, education is crucial, and more and more universities, patient organizations, and medical societies are organizing patients education to teach (4,29).
The high levels of PPI satisfaction in this training course were probably related to its novelty, the multidisciplinary teams, and the involvement of expert GPS patients. Above all, the main originality was the central role played by patients who founded the GPS and who lead this project with a strong collaboration with the university and its hospital (1). Satisfaction of PPI and faculty members in such training programs have been reported by others in Europe, the United Kingdom, or the United States of America (1,4,8,11,12,30,31).
It is far too early to measure the impact of PPI training on the healthcare system. However, preliminary results in terms of post-course health on the PPI itself and its effects on health professionals are very encouraging. Indeed, studies such as ours report overwhelming benefits for patients and no negative effects (32).
Beyond satisfaction reported in most of the PPI studies, we believe that tools are needed to monitor and report the work of PPI in healthcare. The GRIPP2 (Guidance for Reporting Involvement of Patients and the Public) has already established a checklist with different elements to clearly report the role of PPI in research (33). We believe that similar tools should be in place and followed for work done when patients are taught and when they intervene. Indeed, there is little or no reporting of PPI studies on how they are trained if not at all reported. Previous PPI training ranged from a few hours of information, leaflets, simulated interaction, focus group, and up to 50 h of teaching within 6 weeks for PPI in rheumatoid arthritis (11–13).
This study gives a picture of how PI are recruited and trained in Grenoble. We believe it is important to understand why, how, in what context and for whom, and why PPI agrees to be trained. Our detailed GPS training schedule and methods have resulted in participant satisfaction and high participation in teaching and, to a lesser extent, involvement in research projects. It should be noted that there appears to be a marked scepticism or a low priority of PPI in healthcare in Europe with the exception of the United Kingdom. A 2011 survey on “Can patients be teachers?” showed, in general, patient/user involvement in the education of health professional education was not high on the agenda of influential leaders in health professional education, either at the institutional or national level (4). This is probably related to many issues such as funding, knowledge, but also a lack of reporting on how PPI is implemented and its supposed benefits for patients and the health system. Sharing and strengthening the interactions between these initiatives to learn how best to implement PPI would go a long way to demonstrating the beneficial role of PPI in healthcare.
We recognize several limitations. Results may be skewed by survey self-selection although dissatisfied people are more likely to testify in such satisfaction surveys. We trained a limited number of trainees within 2 years from 2016 to 2017 and one of our priorities is to recruit and train more trainees. The real impact to these new peer health educators at CHUGA, for example, is not yet measurable.
Conclusion
Our training of PPI has brought strong benefits to the trainees. The number of PPI who are trained and involved in healthcare should increase steadily with the establishment of a department of patient education and counseling within the medical and pharmaceutical schools in Grenoble. Grenoble Patients’ School has moved from being a patient association to a formal university department “Département Universitaire des Patients Grenoble Alpes” within the UGA schools of medicine and pharmacy by the end of 2020. This department is now led by 4 patients including the director, 2 professors, one in medicine and one in pharmacy, vice deans for the curriculum of schools of medicine and pharmacy, and 2 CHUGA directors responsible for innovation and user relations respectively. We are now well set up to initiate new courses and research projects.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211069810 - Supplemental material for Successful Training of Patients to Intervene in Health Education and Clinical Research at Grenoble Patient School
Supplemental material, sj-docx-1-jpx-10.1177_23743735211069810 for Successful Training of Patients to Intervene in Health Education and Clinical Research at Grenoble Patient School by Raymond Merle, Jean-Louis Pépin, Olivier Palombi, Albane Pariset, Benoît Allenet and Christophe Pison in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735211069810 - Supplemental material for Successful Training of Patients to Intervene in Health Education and Clinical Research at Grenoble Patient School
Supplemental material, sj-docx-2-jpx-10.1177_23743735211069810 for Successful Training of Patients to Intervene in Health Education and Clinical Research at Grenoble Patient School by Raymond Merle, Jean-Louis Pépin, Olivier Palombi, Albane Pariset, Benoît Allenet and Christophe Pison in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agir pour les Maladies Chroniques, http://fonds-apmc.org/ (grant number for PhD, ANR-12-TECS-0010, ANR-15-IDEX-02).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.