
Abstract
Behavioral health integration (BHI) changes the paradigm of primary care delivery by integrating behavioral healthcare into primary care. Thus, BHI likely alters the shared experiences of both patients and providers in an interrelated manner; however, their experiences are usually evaluated separately. The purpose of this study was to analyze these shared experiences together within patient–provider pairs in integrated clinics. First, patient interviews were conducted using semi-structured interview guides and transcripts were analyzed for major themes of patient experience. Next, providers named in patient interviews were interviewed around these same themes. Thematic analysis was performed on 18 transcripts (11 patients, 7 providers). Common themes included BHI experience, pain management, feeling heard by providers, and health care experiences. Areas of alignment included positive perception of BHI, an absence of long-term care, and a desire to share decision-making. Pain management was a persistent area of conflict, and the differing experiences were consistent with a change in the psychodynamic patient–provider model. This conflict highlights a gap in BHI and a need for provider education about psychodynamic relationship models.
Keywords
Introduction
Health systems have increasingly integrated behavioral health and primary care to improve access to, and normalize treatment for, behavioral health challenges (1–5). In the past, the paradigm of primary care involved a two-party relationship (primary care provider [PCP] and patient). With behavioral health integration (BHI), the model is changed such that the PCP works jointly with a behavioral health specialist (e.g., behavioral health care manager and/or psychiatric consultant) to care for patients receiving behavioral health services (6). By involving more people in primary care and distributing the burden of care between three types of providers, BHI is thought to alter the experiences of both patients and providers. However, patients and providers/staff have typically been studied separately. For example, in a large study of 542 patients in a primary care BHI setting, patients rated the “therapeutic alliance” (a concept covering agreement on shared goals and mutual bonding (7)) with their behavioral health provider higher compared to previous studies of nonintegrated outpatient psychotherapy (3.64 ± 0.55 vs. 3.19 ± 0.58, respectively) (8). Separately, 96% of 86 primary care staff in primary care clinics integrated since 2011 reported that BHI was a “worthwhile investment” and “ensures that patients receive appropriate care” (9).
There are few studies about the impact of BHI on shared experiences within patient–provider pairs. The quality of this relationship is foundational to behavioral health because it influences “patient activation” (essentially, being self-managing (7)), which in turn drives positive behavioral health-related behaviors (7). Conversely, when a patient–provider relationship is impaired due to patients feeling unheard, disrespected, or out of partnership with their physicians, measures such as frequency of visits, adherence to treatment, patient satisfaction, and pain are impacted (10).
As part of a larger study that sought to examine the association of BHI on patient-reported and claims-based outcomes (11,12), the aim of this qualitative study was to characterize the shared experiences of patients and providers in a primary care BHI setting. There were two objectives: (1) identify experiences that were important to patients and (2) compare these experiences to those of corresponding providers.
Method
Study Design
This study was performed as part of a larger project evaluating patient experiences with BHI integration. A convenience sample of patients and providers from the same primary care clinics that had adopted BHI were enrolled in the study. Briefly, a two-stage interview approach was used (Figure 1). Patient interviews were conducted first, and themes of patient experience were analyzed. An interview guide for providers was then developed based on patients’ themes of experience; this ensured that both sets of interviews were inherently interrelated. The providers selected for interviews were individuals who had been named by patients. The semi-structured interview guides are shared in Supplementary Material. These guides were designed to employ a multiple case study approach for understanding a phenomenon (experience with patient care) within a specific, bounded setting (BHI clinic) using multiple sources of data (patients and providers) (13). For both sets of interviews, the average time to complete an interview was about 30 min. Cash incentives were provided for all patients. Providers did not receive any monetary incentive.

Interview process driven by patient domains of experience.
Patient Interviews
The patient interview guide was semi-structured, allowing the interviewer to guide the conversation and explore unique lines of inquiry for each patient (n = 11). Themes addressed in the patient interview guide included health, healthcare experiences, experiences of stigma, and the provider relationship. Specific questions were developed with a Patient Advisory Team, a group of patients who experience physical and mental health challenges and who agreed to participate as partners in the research design.
Provider Interviews
For provider interviews (n = 7), a complementary semi-structured interview guide was developed based on themes that emerged during the patient interviews. Themes listed on the provider interview guide included relationship with patients, BHI, the health care system, and trends in healthcare (including the opioid crisis). The interview guide sought to expose providers’ general tendencies and outlook on patient experience. Interviews were conducted in-person or over the phone based on the preference and availability of the provider.
Analysis of Themes and Themes of Experience
Interview transcripts were coded using Atlas.ti version 8. Thematic analysis approach was used to code and analyze the interview data (14,15). A codebook was generated from the interview guide questions (deductively) as well as from the data (inductively). The research team ensured reliability by reviewing coding and discussing any discrepancies at reoccurring research meetings. A similar codebook was used from both patient and provider interviews, with new provider-specific codes being added as they arose in the data. There were two rounds of analysis. The first round consisted of general patient and provider themes. The second analysis compared and contrasted patient and provider experiences. Similarities and differences between patient and provider experiences were summarized by the four main themes: BHI, pain, feeling heard, and health care. Transcripts were analyzed for similar and contrasting experiences.
Results
Participants
Eighteen transcripts from individuals in patient–provider relationships were analyzed (7 providers and 11 patients). The seven providers included both PCP and mental health providers (Table 1). Most of the participating patients (73%) reported having at least one behavioral diagnosis, and all patients identified as non-Hispanic White (Table 2).
Provider Characteristics.

Notes: Characteristics of providers interviewed for this study. Urbanicity was determined based on the location where providers practiced.
Patient Demographics.
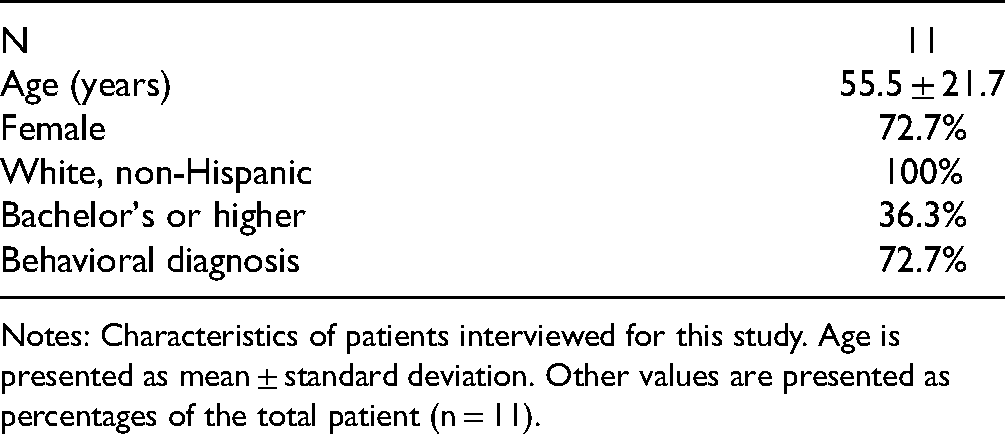
Notes: Characteristics of patients interviewed for this study. Age is presented as mean ± standard deviation. Other values are presented as percentages of the total patient (n = 11).
Patient Themes
Patient Perspectives on Behavioral Health Integration
Patients’ experiences with BHI were generally positive. Improved two-way communication between the patient and their PCP was noted as a strength of care provided in BHI clinics. Patients reported that their PCP was more “prepped” for their visits, eliminating the need to repeat information to multiple providers. Patients also reported that they perceived receiving “whole-person” care. Additionally, about half the patients saw a behavioral health consultant based within the clinic on an as-needed basis and appreciated that they were at the same location as their PCP. One patient stated: “I felt relieved that I wasn't dealing with people in compartments and I felt a sense of security in that if they were noticing things that they wouldn't talk to me directly about, at least they could talk to one another about them. It's just the circle was wider.”
Patient Perspectives on Pain
Patients who had been taken off pain medications reported a range of experiences. In some cases, providers fully explained the rationale, and patients understood the decision, but nevertheless felt their providers were not doing enough to provide alternative care plans. Others did not report receiving an explanation and felt their providers lacked compassion. Some patients reported feeling stigmatized by their providers, which only increased if they used other substances to cope after discontinuation of pain medicine. One patient recalled: “[Provider] said ‘honey, I can't -- I do a different type of pain relief, and from what I can see you’ve got a lot going on right now, and you’re in a lot of pain, and I can't -- I’m not into prescribing the pain, chronic pain. I’m not chronic pain.’ She took away my Klonopins. And just dropped me off them just like that.”
Patient Perspectives on Feeling Heard
Feeling heard by providers played a pivotal role in patients’ perception of provider relationships. Patients who felt they were heard reported that this contributed to a good rapport with their provider. Feeling heard was related to provider listening, which comprised of hearing what the patients had to say, affirming they had been heard (e.g., asking questions or repeating back to them), and then explaining options or courses of action based on what the patient explained. Feeling heard was also important to patient perceptions of treatment decisions. As one patient put it: “At one point when I was talking to [Provider], I was saying, ‘I don't want to go back on medicine, it was hard to get off of it, I didn't like the side effects, I don't want to go on this.’ He was listening, and then he listed off some things that were definite symptoms for me. But for him to then say, ‘Now you’ve just told me this. Why, given these three or four things, would you not want to take medicine?’ To have someone mirror like that, there's a sense of safety, like he heard what I said. […] He helped me make a decision that was critically important, and it felt like [my decision] even though he was definitely probably advocating for it. But it felt like my choice.”
Patient Perspectives on Health Care
Several patients reported being “shuffled around” due to provider promotions, retirements, or resignations. Often, these patients were switched to providers who removed or tapered them off their pain medications, prompting immediate dislike or distrust and leaving patients feeling that their new providers had to “start all over again.” For some, this turnover made them lose confidence in health care: “I’ve had quite a few doctors come and go in the last five to eight years. I had [Provider 1]. [Provider 1] left. I had [Provider 2]. I didn't like [Provider 2]. Then I got [Provider 3]. [Provider 3] left. Then, I got [Provider 4], we actually had a relationship. […] I felt like [Provider 4] got me and we had a good relationship. I felt like I was definitely cared for and then, [Provider 4] left. I’ve never quite been able to establish the same rapport with [Provider 5]. Although I know [Provider 5] is excellent and I like [Provider 5] but my attitude is I’d rather just stay away from the medical establishment, to be honest.”
Provider Themes
Provider Perspectives on Behavioral Health Integration
Like patients, providers also had a generally positive view of BHI. Nevertheless, providers pointed out important gaps in BHI in primary care settings, particularly the absence of long-term behavioral health care.
Provider Perspectives on Pain
Providers often referred to the opioid epidemic as a crisis that had been created in the healthcare system, and that it was up to healthcare providers to solve it. One provider stated: “I, like many of your older PCPs, saw this thing evolve before my eyes. The change, the shift, the getting comfortable with giving more narcotics to patients, I participated in that. Then once you’ve done that, a) you kind of own the patient, and b) trying to get them to see a new direction for pain management is extraordinarily hard.”
Some providers perceived this medicalization of pain as the creation of addicts who did not view themselves as such. This characterization of patients led to providers refusing to prescribe or tapering patients off opioids. Some providers found the process challenging to begin. In the words of one provider: “I would say the worst part about my job is having those conversations. Because there's a lot of, like, emotion attached to those medicines. And patients are scared about decreasing those meds because they’re scared of being in more pain. And a lot of times they’re dependent on them.”
One provider highlighted concern about repercussions: “I think because of fear, like not wanting your name on a prescription, sometimes PCPs probably don't take an -- approach that's -- would be perceived as compassionate. But I think they feel backed into a corner. So that's hard.”
All providers reported that their clinics had some sort of an opioid policy, which ranged from refusing patients completely, to prescribing if the patient met certain criteria, and most frequently, the use of pain contracts. Providers described these contracts as a signed agreement between themselves and their patients that describe the adverse effects of opioids, stipulates the number of pills prescribed, the frequency of refills, a cut-off date (if there was one), and reasons for ending the contract. Enforcement of contracts varied. Some patients who broke the terms of their contracts were given second chances while others were immediately cut from their prescription.
Provider Perspectives on Feeling Heard
Providers frequently reported that attentive listening and repeating back was an important tenet of their practice that enhanced relationships with patients. Providers also recognized the importance of involving the patient in their healthcare decisions, such as explaining diagnoses or results, providing them with an explanation of why they preferred their recommended course of action, or coming to a consensus together on decisions for a plan of care. One provider recalled an example of this: “I always just try to say, ‘We’re here to help you. […] This is your health care.’ And I try to let them know we don't have to do anything that you don't want to do, and you don't have to take anything you don't want to take.”
Patient buy-in was important to initiate a plan of care and build trust. For some providers, a lack of patient buy-in meant a discontinuation of their services. “I would say it's probably about 20% of people where I might get pushback or hesitancy or where I just feel like they’re not in a place to receive kind of any interventions from me. Most people I can get the buy in of what are your goals.”
Another provider added: “Sometimes it works, and sometimes it doesn't. Sometimes you lay out the plan, and this is the plan I see for you, and like I said, patients are like ‘No. I’m not doing that.’ It's kind of like we say goodbye and that's, to me, no harm, no foul. What's really hard is when you say you have a choice of A or B, and the patient keeps picking C, which isn't an option.”
Provider Perspectives on Health Care
The theme of provider burnout emerged from several interviews. Some providers shared their own experiences of exhaustion while others mentioned witnessing it among colleagues by noting earlier retirements or surprise departures. Reasons cited were burdensome amounts of tasks during patient visits and limited amount of time with each patient. A provider shared their experience here: “It gets a bit overwhelming for all the things that we’re asked to do. A person's coming in for a wart, and we’re trying to do as much as we can. We’re trying to – ‘you’re due for this and that immunization.’ We have to do [different screenings]. We have to do this. We have to do that. […] It's what we need to do, but it really impacts the number of patients we can see. I think in order to continue it, it runs up against issues with we’re going to make it more successful without burning out providers.”
Similarities and differences between patient and provider experiences were summarized by the four main themes: BHI, pain, feeling heard, and health care.
Discussion
Patient and provider interviews highlighted areas of alignment and areas of conflict in integrated healthcare. Both patients and providers were aligned in their desire for communication and shared decision-making, and each group generally felt that these areas were improved by BHI. Patients also described receiving “whole-person” care in the integrated setting. This feedback could be interpreted to mean that patients received multidimensional healthcare (16) that met their physical and psychosocial healthcare needs in a harmonious way. Despite these positive changes, however, BHI did not eliminate conflict over pain care, which remained an area of conflict and frustration for both patients and providers.
Psychological interventions are important determinants of the impact of chronic pain on disability; therefore, chronic pain management is a major focus of BHI (17). However, our interviews suggest that BHI may not alleviate patient–provider conflict over pain management strategies. Patients perceived being stigmatized or ignored by providers. Meanwhile, providers reported that it was difficult to converse with high-need pain patients. Providers identified opioid use as a provider-made problem and recognized patients’ hesitancy and fear of non-opioid pain management strategies. Nevertheless, many providers also engaged in victim blaming, recalling that their patients were in denial of their addiction or were not trying hard enough to stop. Our interviews suggest that patients sense these attitudes and beliefs from their providers. These findings agree with our previous report that 27% of patients in integrated clinics experience stigmatization and these patients are over three times more likely to report communication problems with their providers (11).
The mutually frustrating experiences of patients and providers in negotiating pain care may be explained in terms of common psychodynamic models in healthcare. Specifically, our interviews suggest that both patients and providers prefer to operate within the mutual participation model, which involves consensual decision-making and power sharing, but that negotiations over pain management often involve a switch to the guidance-cooperation model (10,18). The guidance-cooperation model eliminates negotiation and requires the patient to cooperate with the provider's greater knowledge and power. Such a switch explains providers’ experiences of discomfort and conflict and patients’ experiences of disempowerment and being ignored. This change is also directly contradictory to encouraging patient activation, which is foundational to mental health management (7). Thus, our findings suggest that providers in BHI settings may need education about model switching during interactions with pain patients.
An important limitation of this study is that the entire patient population self-identified as non-Hispanic White adults. White individuals are more likely to report depression and less likely to report chronic pain compared to Asian and Black individuals, whereas Black individuals are more likely to have comorbid depression and chronic pain (19). Furthermore, the participants in this study were a convenience sample from a larger BHI study. The absence of non-White experiences, the limited nature of the sample, and differences in interview setting (in person vs. over the phone) limit the depth and representativeness of the results. Additionally, the fact that the population was sampled from seven outpatient clinics means that the results may not be generalizable to other care settings. Finally, the data were not analyzed to look at any differences by self-reported behavioral diagnoses; this could be an area of future research.
Conclusion
Our findings suggest that BHI improves both patients’ and providers’ experiences with communication but may not eliminate tension over pain management. Patients with pain, especially chronic pain, may require additional specialist care and perhaps alternative care providers. Additionally, these data suggest that patients and providers may unconsciously change from consensual negotiations to a less cooperative dynamic during pain management conversations, suggesting that education in these negotiations is needed.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211063296 - Supplemental material for Evaluation of Shared Experiences Among Patients and Providers Following Behavioral Health Integration in Primary Care
Supplemental material, sj-docx-1-jpx-10.1177_23743735211063296 for Evaluation of Shared Experiences Among Patients and Providers Following Behavioral Health Integration in Primary Care by Natalie Kenton, Nicole Bouranis, Emily J. Cox, Laura Jacobson and Bill J Wright in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Patient-Centered Outcomes Research Institute (grant number IHS-1310-08388).
Ethical Approval
Ethical approval to report this case was obtained from Providence Health & Services Institutional Review Board (approval #14-247A). Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Providence Health & Services Institutional Review Board (approval #14-247A) approved protocols.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.