
Abstract
The COVID-19 pandemic has transformed the health care landscape and shifted individuals’ expectations for and interactions with essential health services, including pregnancy-related care. This study explores alterations to individuals’ pregnancy and childbirth decisions during an infectious disease pandemic. A convenience sample of 380 pregnant individuals with an expected delivery date between April and December 2020 consented to enroll and complete an online questionnaire on their pregnancy and childbirth expectations during the COVID-19 pandemic; a subset of respondents (n = 18) participated in semi-structured phone interviews. Survey data were analyzed quantitatively while interview data were analyzed using a thematic content analysis until a consensus on key themes was achieved. Respondents reported substantial stressors related to shifting policies of health care facilities and rapidly changing information about COVID-19 disease risks. As a result, respondents considered modifying their prenatal and childbirth plans, including the location of their birth (25%), health care provider (19%), and delivery mode (13%). These findings illuminate the concerns and choices pregnant individuals face during the COVID-19 pandemic and offer recommendations to engage in compassionate, supportive, and person-centered care during a time of unprecedented risk and uncertainty.
Introduction
The declaration of the novel coronavirus (severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2)) as a global pandemic on March 11, 2020, unquestionably altered the landscape of public health and health care services in the United States and across the globe. 1 Pregnant individuals face rapidly changing information about risks of COVID-19 disease during pregnancy, as well as shifting policies from health care facilities. Understanding how these factors have impacted the pregnancy and childbirth expectations among pregnant individuals is a critical effort, especially given that their decisions may be altered under the uncertainty of the COVID-19 pandemic. Most studies that explore the intersection of COVID-19 disease and pregnancy have focused on the clinical treatment of COVID-19 disease and risk factors among pregnant individuals and neonates.2–6 Prior frameworks recognize the interconnected system of biomedical, psychological, and social needs including individuals’ thoughts, emotions, attitudes, behaviors, social determinants of health, and sociocultural expectations for pregnancy and childbirth that impact perinatal care experiences, and their related outcomes. 7 A few studies have highlighted how the COVID-19 pandemic has elevated other relevant factors, including pregnant individuals’ stress,8–10 generalized fear and anxiety,11–13 and depressive symptoms.11,13 Identified risk factors for elevated mental health symptoms include women's abuse history, chronic illness, income loss due to the pandemic, concerns about changes to prenatal care, discomfort with hospital visits, having insufficient information about COVID-19 disease, social isolation, and high-risk pregnancy.8,11,13 Pregnant individuals have also reported other pandemic-related changes to their care experience including reduced prenatal appointments, changing birth locations and providers, and modifying hospital birth plans to reduce hospital stays and accommodate hospital policy changes.9,14 The goals of this study were (1) to understand how the COVID-19 pandemic has altered pregnant individuals’ perceived needs and expectations about pregnancy, childbirth, and postpartum stages, based on the patient perspective and (2) to offer emerging information to assist providers in addressing pregnant individuals’ needs for informational, structural, and social support while balancing the need for infection prevention strategies that are essential during a major pandemic event.
Methods
This study recruited a convenience sample of individuals of reproductive age (18–45 years) who were pregnant with an expected delivery date (EDD) during the months of April to December 2020. Respondents were targeted through internet fora and public social media groups for pregnant individuals during that period. Recruitment messages and social media posts were made in English and Spanish. The recruitment invitation asked respondents to share the study information with other personal acquaintances who may also qualify for the survey (standard snowball sampling methodology). 15 Survey domains included: respondent demographics, pregnancy intentions and timing, prenatal care experiences, childbirth plans and expectations, and concerns related to COVID-19 disease. The online survey was administered in English and Spanish to participants who met inclusion criteria: (1) at least 18 years of age, (2) pregnant at the time of the survey, (3) EDD between April and December 2020, (4) residing in the United States, and (5) proficient in English or Spanish. Respondents consented to participate in the study by clicking on an electronic button indicating their agreement to participate in the study protocols described on a study information page. Those who enrolled and completed the survey were entered into a raffle for a $25 gift card incentive. The survey data were analyzed descriptively, using STATA v.12 16 to report frequencies on key variables of interest. In addition, open-ended text-based questions were analyzed using a thematic content analysis 17 to inductively identify key themes related to perceptions of pregnancy and childbirth during the COVID-19 pandemic.
After the survey, participants opted-in to semi-structured phone interviews focused on pregnancy and childbirth expectations, plans, and experiences. A team of interviewers obtained verbal consent, conducted, audio-recorded, and transcribed the in-depth interviews. Through an inductive thematic content analysis, the team identified key themes that represented the central experiences of participants. Bracketing procedures 18 were used to account for the researchers’ identity as an interpretive instrument during the data collection. All study protocols were approved by the Human Subjects Review Council of Central Washington University.
Results
A total of 1,556 individuals responded to the original recruitment invitation. After applying the screening protocol, 609 respondents met the inclusion criteria for the study. Respondents with the majority of the survey completed (51% or more) were included in the final total sample of n = 380. A random selection of 42 respondents who agreed to be contacted for follow-up were invited to participate in an in-depth interview during their pregnancy. A total sample of n = 18 participants completed qualitative interviews.
Sample Characteristics
Among the survey sample, the average age was 34 years and the mean household size was 3.07. Most respondents were married or in a domestic partnership (93.2%). Nearly all respondents reported having access to health insurance (98.2%) but this varied by employer-sponsored coverage (73.8%), purchased on the individual marketplace (4.9%), and publicly insured (18.9%). Many respondents had some college-level education (55.3%) or advanced degree (37.6%) with 6.3% of respondents reporting that they had a high school degree, general equivalency diploma (GED), or less. Sample characteristics reported in Tables 1 and 2 contain select qualitative quotes organized by key themes on patients’ prenatal experiences, childbirth expectations, and priorities for pregnancy-related care during the COVID-19 pandemic.
Sample Characteristics (n = 297).

Select Illustrative Quotes on Qualitative Themes.

SARS-CoV-2: severe acute respiratory syndrome-coronavirus-2; PPE: personal protection equipment; EDD: expected delivery date; OB: obstetrician.
Prenatal Care Experiences
Most respondents reported navigating significant changes to their experience with prenatal care (Figure 1). Sixty-four percent of respondents felt that their health care provider gave them enough information on how to protect themselves and their baby from COVID-19 disease, while over one-third of respondents did not feel they had sufficient information. A majority of respondents (71%) reported that their prenatal care experience changed noticeably because of the COVID-19 pandemic, and 58% reported having used remote or telemedicine options for prenatal care. One in five respondents (20%) reported postponing or avoiding care related to their pregnancy because of the COVID-19 pandemic. Open-ended and interview responses indicated that prenatal appointments were canceled, shortened, changed in frequency, or modified from in-person to telemedicine (Table 2). Some participants expressed feeling that prenatal care was inadequate or that appointments, ultrasounds, or lab work were not prioritized.

Prenatal care experiences.
Others reported declining care to avoid potential viral exposure in health care settings.
Participants also reported dissatisfaction and a sense of loss because partners and family members were no longer permitted to accompany them to prenatal visits due to policy changes in health care settings.
Many respondents (83%) reported that their hospital or birth center facility changed at least one policy related to prenatal care and/or childbirth with 95% of respondents indicating that they were aware of policy changes that limited or restricted visitors and/or support persons during labor.
Childbirth Plans and Expectations
Respondents were asked to report their plans for delivery at the time of the survey. Among the sample, 90% reported they planned to give birth at a hospital facility, 4% at a licensed birth center, 5% at an attended homebirth, and 1% unspecified. Eight-in-10 respondents (84%) planned to deliver vaginally, 12% reported plans to deliver by cesarean section, and 5% of respondents indicated that they had not determined their delivery mode at the time of the survey.
Respondents were asked if they had considered changing their childbirth plans after the onset of the COVID-19 pandemic (Figure 2). Among the sample, 25% (n = 95) reported they considered a change in childbirth location or facility. Among those who considered a change, 23% considered switching to a hospital location (or another hospital), 14% considered switching to a freestanding birth center, 63% considered switching to a homebirth with a licensed provider, and 10% considered switching to a home birth without a licensed provider (e.g., unassisted or free birth). Three percent reported considering some other unspecified delivery location or facility. Among those who had considered changing their planned childbirth location or facility, nearly one-third (32%) had already formally made those changes at the time of the survey, representing 8% of the total sample. Almost one-fifth of those who reported considering changes to birth locations (19%) were still undecided on formalizing these changes.

Considered change in birth location or provider.
Respondents frequently cited reasons for considering changing birth locations, including a perception that settings with a higher patient volume may present a higher risk of SARS-CoV-2 virus transmission. Several respondents also felt their decisions about birth locations during the COVID-19 pandemic were constrained by other structural barriers, including insurance coverage and facility protocols. The most frequently expressed concern that motivated participants to consider a change in birth setting was related to the perception that some birth facilities would limit or prevent partners, support persons, or family members from attending the birth.
Respondents were asked if they had considered switching providers for prenatal or obstetric care (Figure 2). Nineteen percent (n = 72) of survey respondents reported thinking about seeking a different provider, with 61% of them considering a Certified Nurse Midwife, 46% considering another type of midwife (e.g. Licensed Midwife, Certified Professional Midwife), and 32% considering switching to an obstetrician-gynecologist or other physicians. Many respondents indicated they were weighing options between multiple provider types and could select all provider types that applied to this question. Among those who considered switching providers, 28% had made these formal changes to their provider at the time of the survey, which represents ∼5% of the total sample. Twenty-one percent reported still considering decisions about provider changes.
Respondents were asked if they had considered making any changes to their delivery mode (vaginal or elective cesarean section). Thirteen percent of respondents indicated they had considered a change in their preferred type of delivery at some point during their pregnancy, with nearly all (96%) indicating they preferred a vaginal delivery. Respondents cited the perception of being discharged from care earlier after vaginal delivery compared to a cesarean section as one of the motivating factors for preferring a vaginal birth.
Priorities and Concerns Related to Pregnancy & Childbirth During the COVID-19 Pandemic
Respondents were asked to report their priorities and concerns related to pregnancy, childbirth, and postpartum care during the COVID-19 pandemic (Table 3). Concerns were classified into five categories: exposure to the SARS-CoV-2 virus; hospital or birth center policies; infant feeding, personal products and supplies; financial and childcare costs; and postpartum needs and support. A significant proportion of respondents were concerned about their own exposure (88%), their infant's exposure (90%), or exposure of a family member to the SARS-CoV-2 virus (91%). The most frequent concern related to hospital or birth center policies, reported by 88% of respondents, was the possibility of being separated from their infant, if either mother or infant tested positive for the SARS-CoV-2 virus. Participants expressed a range of reactions to this possibility, including fear, uncertainty, and resistance.
Concerns Related to Pregnancy and Childbirth During COVID-19 (n = 379).
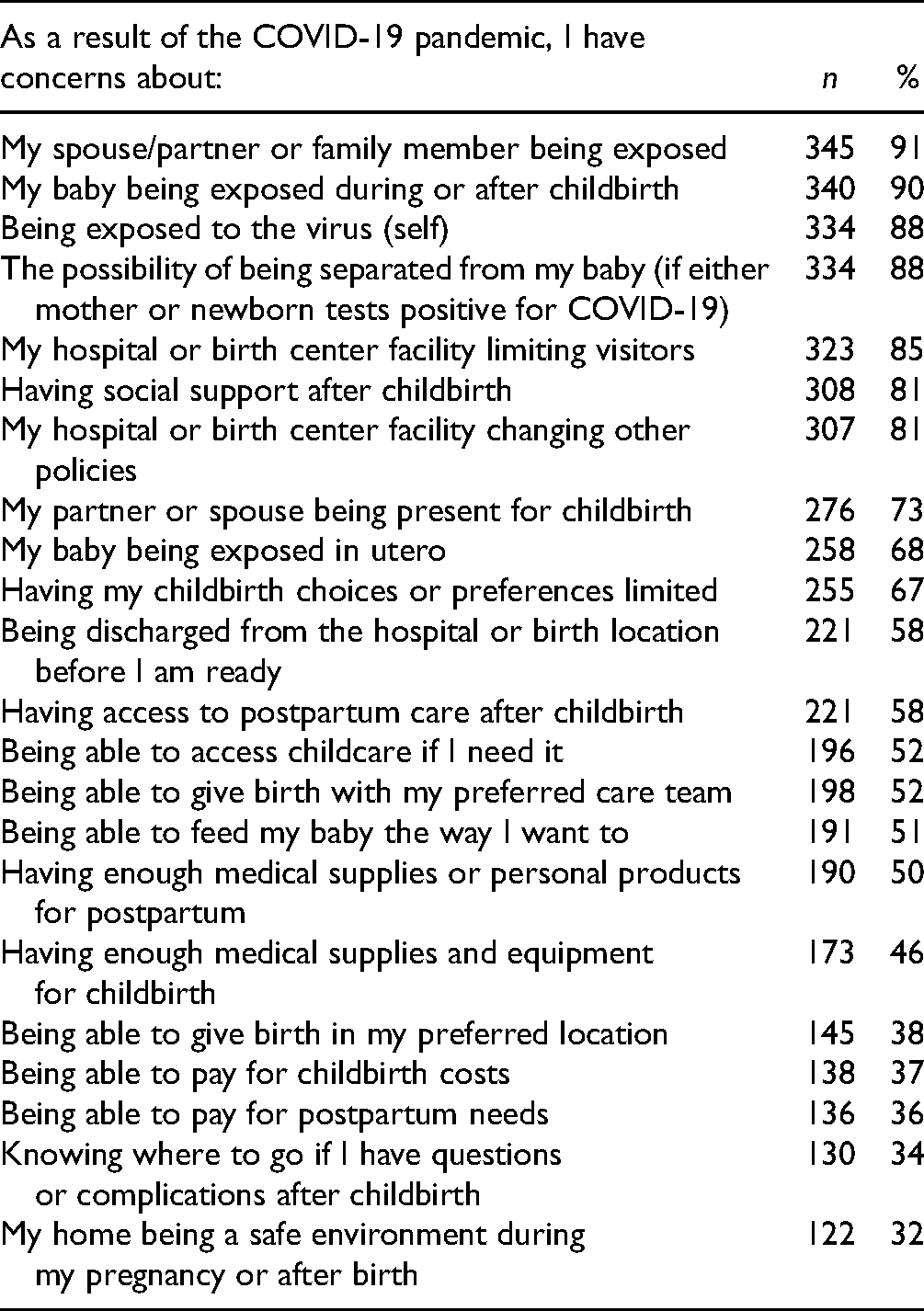
A high proportion of respondents (85%) had serious concerns about hospital policies and restrictions on visitors or labor support, with 73% of respondents being worried that their partner would not be able to be present for childbirth, and 67% being worried about having their childbirth choices limited, generally. These new policies and protocols, and their perceived impact on the birth experience elicited emotional responses from participants that ranged from fear, distress, lack of confidence, to grief, and disappointment.
Respondents shared concerns about accessing resources and support after birth. Over one-third of respondents reported financial concerns, including being able to pay for childbirth-related costs (37%) and postpartum needs (36%) while half of the respondents expressed concerns over accessing childcare (52%). Respondents were concerned about having enough medical supplies, equipment, or personal products for childbirth (46%) and postpartum needs (50%), and concerns over being able to feed their baby in the way they desired (51%). Over 80% of respondents indicated they were concerned about having enough social support after childbirth, and 58% felt concerned with their ability to access postpartum care. One-third of respondents (34%) were concerned about where to go for information or questions about complications related to childbirth and postpartum. For many participants, these barriers represented a source of unexpected stress, while for others, the lack of options simplified their decisions.
Discussion
This study highlights critical patterns in the expectations, behaviors, and experiences of a convenience sample of pregnant individuals during a major public health crisis. In particular, the COVID-19 pandemic reflects a high degree of uncertainty, to which many pregnant individuals have responded by reconsidering certain prenatal and childbirth decisions. Virtually all respondents reported having to navigate a change in one or more policies affecting their pregnancy-related care. Under these conditions, many respondents considered different options for the location of their birth and health care provider. This study revealed patterns in emerging priorities and needs related to navigating pregnancy, childbirth, and postpartum experiences during the COVID-19 pandemic; most notably, pregnant individuals’ concerns about protecting themselves and their loved ones from the SARS-CoV-2 virus, health system policies that might limit their partner or birth support person present for the birth, fears about being separated from their infant in the event of exposure, and resources and support during the postpartum phase. These results echo other findings from a survey of pregnant women in April 2020 that indicated a large number of pregnant individuals considered changes to their birth location and provider. 14 Other frequently cited concerns reflected the resource and support needs of expecting families that weigh heavily on individuals preparing to give birth during a pandemic; namely financial stressors, access to childcare, the safety of their environment, and anticipated needs for supplies, equipment, or personal products for the postpartum stage. While these concerns often exist outside of the traditional health care settings, health and social service providers must acknowledge the entirety of a birth person's needs for such supports to appropriately deliver high-quality person-centered care.
Providers should assess their patients’ priorities and acknowledge the complexity of the decisions that are laid before pregnant individuals, recognizing that the shared decision-making approach toward optimal perinatal outcomes may be even more complex during a pandemic event. Pregnant individuals may experience heightened vulnerability during the COVID-19 pandemic because of added financial, psychological, or social constraints. For this reason, individuals’ decisions and behaviors may be influenced by a different set of interconnected factors than would otherwise affect their decision-making about pregnancy and childbirth in the absence of COVID-19 disease. Providers may consider implementing screening protocols for assessing patients’ social and mental health needs at regular intervals during pregnancy, especially for those who transfer care prior to birth.19–22 Referrals to appropriate services and supports during the perinatal period are critical; careful attention should be paid to the accessibility of such care under the conditions presented by the COVID-19 pandemic.
Understanding how pregnant individuals and their families perceive their options for pregnancy and childbirth, and their intended behaviors with respect to maternity care are critical to ensuring that health systems and providers have the capacity to meet individuals’ needs with compassionate, person-centered care that supports pregnant individuals during the unprecedented risk and uncertainty of the COVID-19 pandemic. Accounting for the collective lived experiences of individuals undergoing pregnancy and birth during a pandemic event through qualitative data is an effort that has not been readily incorporated in other COVID-19 disease studies. Hearing directly from the voices of individuals is a vital component to fully understanding their experiences and to developing protocols, policies, and interventions to support person-centered pregnancy and birth care during times of public health crisis.
Despite these important contributions, some key limitations of this study should be noted. First, the study recruited subjects using convenience sampling methods and did not achieve representation as the sample skewed toward predominantly White, middle-high income, and highly educated participants. The findings of this study are best framed as a preliminary study toward building an understanding of the impact of the COVID-19 pandemic on pregnancy and childbirth experiences, and generalizations about the larger population of pregnant individuals should not be made. It is important to note the experiences of pregnant individuals who face vulnerability due to socioeconomic status; minority racial, ethnic, or linguistic identity, or other forms of marginalization that constrain their ability to access high-quality care and support during pregnancy, are only minimally included in this convenience sample. The respondents in this study, although mostly White, well-educated, and higher-resourced, still expressed significant pandemic-related distresses and needs for support in navigating the uncertainty of being pregnant and giving birth during a pandemic event, despite their fair degree of social capital and relative advantage. It is, therefore, a fundamental imperative that future studies investigate the collective experience of populations who are not adequately represented in this and other similar studies, especially when the COVID-19 pandemic may compound negative maternal health outcomes.23–27 Future efforts must reflect the representation of these individuals to provide the most comprehensive description of the realities faced by vulnerable populations.
Furthermore, the sample reflected a high proportion of pregnant individuals who reported planning an out-of-hospital birth (nearly 10%), where population estimates reflect that ∼1.5% of births in the United States occur outside of hospital facilities. 28 Whether this difference is due to sampling bias or the impact of the COVID-19 pandemic on pregnancy and childbirth decision-making is unclear, but these findings suggest the COVID-19 pandemic may play a discernable role. In addition, time effects were not accounted for in this study, as the survey asked pregnant individuals to report their point-in-time prenatal experiences and to project their childbirth expectations during a rapidly changing public health crisis. Similarly, the survey only captures the perceptions of respondents during their third trimester, but does not estimate further their gestational age. Most notably, the evolution of the COVID-19 pandemic and response efforts at the community, state, and federal level has significantly changed, and would assuredly be reflected in respondents’ experiences if they were expressed longitudinally.
Conclusion
The purpose of this study was to gather preliminary information on pregnancy and childbirth expectations, decisions, and experiences during the COVID-19 pandemic in the United States. The findings illustrate the concerns, priorities, and decision-making factors that lead pregnant individuals toward or away from certain experiences during their pregnancy in the context of a major pandemic event that carries emerging, yet significant risk for pregnant individuals. This effort is vital to ensuring that the US health system is prepared to meet pregnant individuals’ unique needs and to adequately extend support and services in a person-centered model, in the context of community-mitigation strategies against an infectious disease pandemic event.
Footnotes
Authors’ Note
This study was approved by the Human Subjects Review Council at Central Washington University. All of the procedures involving human subjects were conducted in accordance with the Human Subjects Review Council's (2020-085) approved protocols. This article does not contain any studies with animal subjects. Informed consent was obtained from the patient(s) for their anonymized information to be published in this article. Respondents documented their informed consent by clicking an electronic button indicating they agree to participate in the online survey as it was described on the study information page. For procedures involving qualitative interviews, participants gave verbal consent.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Central Washington University Internal Research Award.