
Abstract
Chronic lymphocytic leukemia (CLL) often requires consideration of multiple treatment options. Shared decision-making (SDM) is important, given the availability of increasingly novel therapies; however, patient–provider treatment conversations vary. We examined relationships between patient–provider discussions of new CLL treatment options and sociodemographic, clinical, and patient–provider communication variables among 187 CLL patients enrolled in Cancer Support Community’s Cancer Experience Registry. Factors significantly associated with self-reports of whether patients’ providers discussed new CLL treatment options with them were examined using χ2 tests, t tests, and hierarchical logistic regression. Fifty-eight percent of patients reported discussing new treatment options with their doctor. Patients with higher education were 3 times more likely to discuss new treatment options relative to those with lower education (OR = 3.06, P < .05). Patients who experienced a cancer recurrence were 7 times more likely to discuss new treatment options compared to those who had not (OR = 7.01, P < .05). Findings offer insights into the correlates of patient–provider discussions of new CLL treatment options. As novel therapies are incorporated into standards of care, opportunities exist for providers to improve patient care through enhanced SDM.
Keywords
Introduction
Chronic lymphocytic leukemia (CLL) is the most common form of adult leukemia, accounting for one quarter of all new leukemia case (1). CLL starts in lymphocytes in the bone marrow and progresses with time, such that patients may receive treatment several times. Initial CLL treatment tends to be conservative given that, oftentimes at diagnosis, patients show few symptoms with no signs of significant disease progression (2). Patients often enter a period of “watch and wait” (active surveillance) to monitor disease progression (3). With disease progression, patients commonly undergo active treatment and return to active surveillance until a second line of treatment is indicated. Thus, over the long term, CLL requires consideration of treatment options at various points along the care continuum. Heterogeneity in CLL treatment experiences across patients is further complicated by the increasing availability of novel CLL treatments approved by the Food and Drug Administration, including targeted therapy and immunotherapy options (4). Although treatment outcomes for recently approved therapies are promising—including the potential for long-term, disease-free survival (5,6)—the efficacy of such treatments is highly dependent on patient characteristics such as age, cytogenetic profiles, comorbidities, and overall health (7).
Given the rapidly changing CLL treatment landscape, patients may not be fully informed of their treatment options nor adequately prepared to make treatment decisions (8). An absence of tools to evaluate treatment options can hinder shared decision-making (SDM) (9). In turn, patients may rely on health care providers for CLL treatment information to make individualized treatment recommendations. Indeed, providers play an important role in the decision-making process through the discussion of new treatments and provision of up-to-date information (9), thereby supporting SDM. The very nature of CLL requires long-term consideration of multiple treatment options, such that each line of therapy represents an additional opportunity for continued education on CLL treatment options and SDM (10).
Amid the evolving CLL treatment landscape, there is a need for better understanding of patient-reported experiences that may inform patients of all available treatment options and prepare them to engage in SDM. The implications of patient–provider communication (PPC) are far-reaching, particularly for quality of life and psychosocial outcomes among individuals with CLL (8,11). There are several potential barriers and facilitators to effective SDM. Prior research in other patient populations indicates that sociodemographic factors such as gender identity, race/ethnicity, and cultural background may influence PPC and SDM (12 –15). Such work demonstrates that sociodemographic concordance between patients and providers can facilitate communication and decision-making, while differences can hinder communication and subsequent SDM. Other research has shown that clinical and provider factors, such as provider communication style, content, and time constraints, may positively or negatively impact PPC (16,17), thereby influencing SDM.
Given limitations in SDM in oncology (9), this research endeavors to enhance understanding of communication barriers for patients and providers, thereby elucidating where to target efforts for improved communication and SDM. This study aims to examine the sociodemographic, clinical, and communication factors that distinguish CLL patients who have conversations with their providers about new treatment options from those who do not and to identify which of the aforementioned factors are related to having conversations about new treatment options.
Methods
Data and Sample
Data were drawn from the Cancer Experience Registry® (CER) of the Cancer Support Community (CSC), an online survey designed to examine the social, emotional, and practical impact of cancer on individuals who have ever been diagnosed with cancer. All respondents were invited to complete a core survey; those reporting a diagnosis of CLL were invited to answer additional questions specific to CLL. Participants were recruited through an extensive outreach program including CSC’s network of community-based affiliates, online communities, toll-free Cancer Support Helpline, partnerships with advocacy organizations, and social media. Ethics approval for the study was received from Ethical and Independent Review Services (Independence, MO). Participants provided informed consent electronically prior to participation. From March 2013 through December 2017, 243 individuals registered for the CER, reported CLL as their primary diagnosis, and began the survey. The analytic sample for this study included 187 participants who reported CLL as their primary diagnosis.
Measures
Doctor discussed recent treatment
The dependent variable was a single-item, dichotomous, patient-reported indicator that asked, “Have you and your doctor ever discussed using any of the newer treatments recently approved for CLL, for example, ibrutinib, idelalisib, or obinutuzumab?”
Sociodemographic characteristics
Sociodemographic characteristics included age, gender identity, race (recoded dichotomously as White or AIAN/Asian/Black/Native Hawaiian/Pacific Islander/Other/multiple races), Hispanic ethnicity, annual income (collapsed to 3 categories: <US$39 999, US$40 000-US$99 999, US$100 000+), educational attainment (high school or less, some college, bachelor’s degree, graduate degree or higher), and urbanicity (urban, suburban, rural).
Clinical and treatment characteristics
Time (years) since diagnosis was measured continuously. Dichotomous treatment variables included whether the patient was currently on “watch and wait,” reported ever having received chemotherapy, and reported experiencing a cancer recurrence. Self-reported history of biomarker testing was captured via 3 dichotomous variables: patient reports of a deletion 17p, 13q, or 11q mutation. CLL risk was identified by patient self-report of how their doctor estimated their CLL may progress over time, measured with a categorical variable indicating low, intermediate, or high risk.
Patient–provider communication
Patient involvement in treatment decision-making, patient satisfaction with their doctor’s explanation of treatment benefits, patient satisfaction with their doctor’s explanation of treatment risks and side effects, and patient satisfaction with how much their doctor and health care team spoke to them about the financial costs of each treatment option were each measured on a 5-point Likert-type scale (not at all, a little bit, somewhat, quite a bit, very much). Two dichotomous communication variables asked patients whether their health care team explained their (the health care team’s) goals of treatment with the patient and whether the patient discussed their own treatment goals with their health care team.
Analytical Approach
Independent sample t tests and χ2 tests were used to detect statistically significant differences in the occurrence of conversations about new CLL treatments across a range of variables. Hierarchical binary logistic regression was employed to estimate the likelihood of providers discussing new treatment options with patients by key sociodemographic, clinical, treatment, and PPC characteristics. In regression models, the reference group for CLL risk was low.
Missing data were imputed for 22 variables (17 from the logistic regression model and 5 auxiliary variables) using the Markov Chain Monte Carlo computational method. Forty imputations were run to obtain adequate efficiency (18). Missing data for individual variables in the regression model ranged from 18% to 47%. All individual cases for which the dependent variable or >50% of data on regression model variables was missing were excluded from imputation; this resulted in a final sample size of 145 participants for the regression models, which report pooled estimates from multiple imputation. Descriptive and bivariate analyses were completed using the initial sample of 187 respondents.
Results
Sample Characteristics
Descriptive statistics for study participants are reported in Table 1. The sample of CLL patients (N = 187) was 48% female, 96% White, and averaged 62 years of age (SD = 10), with a mean time since cancer diagnosis of 7 years (SD = 5). A total of 37% of participants reported having a deletion 17p, 46% reported having a deletion 13q, 54% reported having ever received chemotherapy, and 19% reported recurrence of their CLL. Fifty-eight percent of the sample reported discussing new treatment options with their doctor (Table 2).
Participant Sociodemographic and Clinical History Descriptive Statistics (N = 187).a

Note: n’s vary due to missing data; SD = standard deviation.
Abbreviation: CLL, chronic lymphocytic leukemia.
a Number (n) vary due to missing data;
Differences in Patients Who Reported Discussing New CLL Treatment Options (N = 187).a

Abbreviation: CLL, chronic lymphocytic leukemia.
a Number (n) vary due to missing data.
b Higher scores indicate greater satisfaction and/or involvement.
c P < .05.
d P < .01.
e P < .001.
Differences in Patients Who Reported Discussing New Treatment Options
Table 2 reports results from bivariate tests examining differences in the occurrence of conversations about new treatments across a range of variables. There was a statistically significant difference in the level of educational attainment between patients who had and had not discussed recent CLL treatment options with their provider, such that patients with more education were more likely to have discussed treatment options, χ2(3) = 13.27, P < .001. There were also significant differences in treatment status, where those in “watch and wait” status were less likely to have discussed recent CLL treatment options, χ2(1) = 19.16, P < .001, and those who were currently in (or had completed) their second treatment were more likely to have discussed recent CLL treatment options, χ2(1) = 19.96, P < .001. Patients who had received chemotherapy were significantly more likely to have discussed recent CLL treatment options, χ2(1) = 20.90, P < .001. Estimated CLL risk was significantly associated with such discussions, such that those with low risk were significantly less likely to have discussed recent CLL treatment options, χ2(2) = 12.14, P < .01. Additionally, patients who had been diagnosed with cancer more recently were significantly less likely to have discussed recent CLL treatment options, t(133) = −2.15, P < .05.
Bivariate results also demonstrated significant differences regarding PPC factors and the discussion of new CLL treatment options. Patients who were more satisfied with their doctor’s explanation of the risks and side effects of each treatment option were significantly more likely to have discussed recent CLL treatment options, t(60) = 2.30, P < .05; those who were more satisfied with their doctor’s discussion of the financial costs of each treatment option were significantly more likely to have discussed recent treatment options, t(83) = 2.76, P < .01. Patients who had discussed their own treatment goals were significantly more likely to have discussed recent CLL treatment options, χ2(1) = 3.97, P < .05, as were those who reported they had discussed the provider’s goals for treatment, χ2(1) = 5.13, P < .05.
Factors Related to Conversations About New Treatment Options
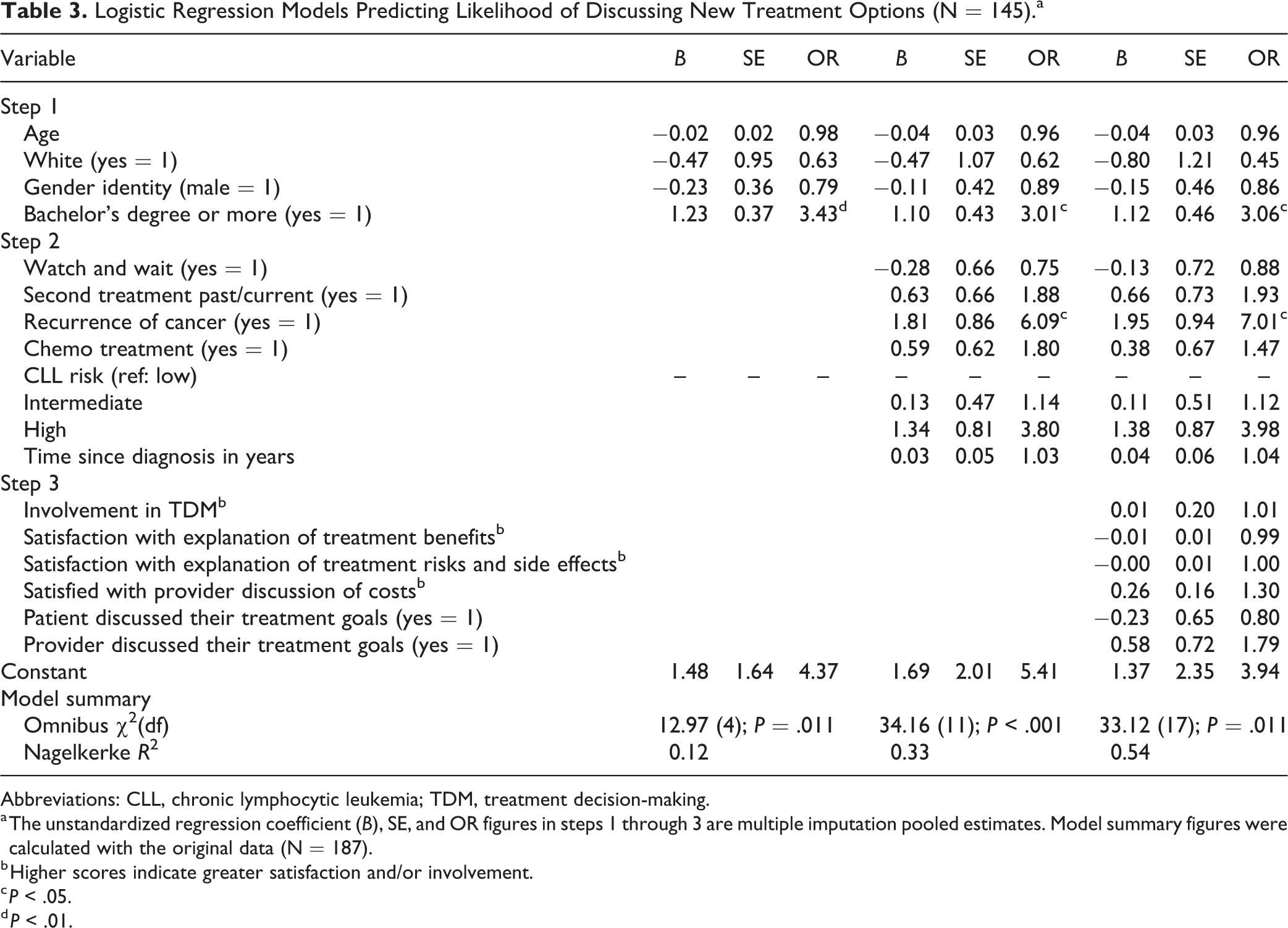
Results from all regression models are presented in Table 3. In step 1 (sociodemographic variables), the overall model was statistically significant, χ2(4) = 12.97, p = .011, with only educational attainment significantly associated with discussion of recent CLL treatment options. Patients with a bachelor’s degree or higher were significantly more likely to have discussed recent CLL treatment options (B = 1.23, OR = 3.43, P < .01). In step 2 (sociodemographic + clinical + treatment variables), the overall model was statistically significant, χ2(11) = 34.16, P < .001. Education level and cancer recurrence were significantly associated with discussion of recent CLL treatment options. Patients with a bachelor’s degree or higher level of education were significantly more likely to have discussed recent CLL treatment options relative to participants with less education (B = 1.10, OR = 3.01, P < .05). Those who reported having experienced a recurrence of cancer were significantly more likely to have discussed recent CLL treatment options (B = 1.81, OR = 6.09, P < .05). In step 3 (sociodemographic + clinical + treatment + PPC variables), the overall model remained statistically significant, χ2(17) = 33.12, p = .011. Education and cancer recurrence remained the only significant predictor variables. Results demonstrated that patients with higher levels of educational attainment were 3 times more likely to discuss new treatment options relative to those with lower education (B = 1.12, OR = 3.06, P < .05), and patients who experienced a cancer recurrence were 7 times more likely to discuss new treatment options compared to those who had not (B = 1.95, OR = 7.01, P < .05).
Logistic Regression Models Predicting Likelihood of Discussing New Treatment Options (N = 145).a
Abbreviations: CLL, chronic lymphocytic leukemia; TDM, treatment decision-making.
a The unstandardized regression coefficient (B), SE, and OR figures in steps 1 through 3 are multiple imputation pooled estimates. Model summary figures were calculated with the original data (N = 187).
b Higher scores indicate greater satisfaction and/or involvement.
c P < .05.
d P < .01.
Discussion
The treatment landscape for CLL specifically, and cancer more broadly, is rapidly changing. The introduction of novel treatments affords opportunities for improved patient outcomes. Given the implications of PPC for improving health outcomes, treatment satisfaction, quality of life, and psychosocial outcomes among CLL patients (8,11), we sought to identify correlates of PPC regarding new CLL treatment options. Our results show nearly half of our sample reported no discussion about new treatment options with their provider, consistent with previous findings that when making medical decisions, providers only ask about cancer patient preferences half of the time (19). These findings raise questions about whether CLL patients are adequately informed about all available treatment options in the era of novel CLL therapeutics. Although patients with higher educational attainment and those who experienced a cancer recurrence were significantly more likely to report discussing new treatment options, findings suggest substantial gaps remain regarding CLL patient awareness of new treatments. Even when controlling for factors indicative of patient-reported involvement in SDM and satisfaction with communication, education and cancer recurrence remain the only variables significantly related to whether patients are informed of the most recent CLL treatments. Together, findings indicate a need for more research into associations between specific communication factors and patient awareness of new treatments.
SDM requires that patients be informed of available treatment options and potential outcomes and are able to incorporate their personal values and/or preferences in the decision-making process (20). Therefore, PPC about new treatment options is critical to ensure patients have relevant information needed to engage in effective SDM. Our results, however, suggest that individuals without a college education are less likely to have discussions with providers about new treatment options than patients with higher levels of educational attainment, and thus may be missing potential opportunities to participate in shared treatment decision-making, thereby perpetuating existing disparities in cancer care (21). To encourage SDM, future research could develop and evaluate patient- and provider-focused interventions aimed at increasing awareness of CLL treatment options and focus on training providers to engage patients of all education levels more effectively.
Results also show that discussions about treatment options are more frequently reported by patients who have experienced a recurrence. The first line of treatment for CLL offers an opportunity for patients to delay further disease progression and maintain current quality of life (22), and recently approved CLL treatments have demonstrated effectiveness when implemented as first-line therapy (5,23). Thus, provider-led discussions and education on newly available treatment options may contribute to positive treatment outcomes for CLL patients facing the first line of therapy. Our results, however, suggest that provider-led discussions about new CLL treatment options more frequently occur following a cancer recurrence and, accordingly, are discussed less frequently (or not at all) during initial treatment decision-making conversations. Further research could explore PPC about novel treatment options for CLL for first-line therapy and the potential impact of such discussions on SDM and patient outcomes.
The success of SDM does not rest solely on patients’ knowledge and ability to understand their options. Health care providers are in a critical position to engage patients in SDM, as patients want to actively participate in treatment decision-making but also want their providers to make recommendations based on personal preferences (24). Patient uncertainty about cancer treatment decisions is a barrier to SDM (25), and not being informed of newer treatment options could enhance treatment decision uncertainty among patients, thereby negatively impacting SDM. However, SDM also relies on the empowerment of patients to engage in conversations with their health care teams (26). For example, doctors provide less information to patients who do not ask questions, express concerns, and make assertions (27). Providers have an opportunity to foster health- and treatment-related discussions in the service of promoting health equity and to engage in strategies that ensure all patients have adequate information to participate in SDM. From a practical perspective, one such approach for empowering and engaging patients may be to engage “lay” or peer navigators in discussing CLL treatment options (10).
This study has limitations that should be considered when interpreting findings. Participant survey data were cross-sectional, limiting our ability to make causal inferences. We relied on patient-reported data of patient–provider conversations, thereby only capturing one perspective. As we relied on patient experience data from a voluntary web-based survey, some selection and/or recall bias may be present in our results. We did not collect information about time since most recent medical provider visit; future research could examine the impact of recency of medical visit in patient perceptions of treatment conversations. Our sample was predominantly White and highly educated; future research could evaluate PPC around new CLL treatment options with a more diverse sample, with attention to reevaluating the roles of patient satisfaction with health care team communication and discussions around goals of care, as patient expectations relevant to these factors may be influenced by their cultural norms (14). It is worth noting that the sample demonstrated balanced gender representation and diversity in household income and urbanicity. Finally, the average time since diagnosis for our sample is approximately 7 years (range: 0-25 years), whereas approvals for select new therapies have been more recent. Although we do not expect that patients diagnosed prior to treatment approvals explored unapproved treatment options with their providers, results suggest that, regardless of the timing of the decision process, patient education and treatment experience relate to the extent to which new treatment options are discussed.
Conclusion
These results provide important information regarding SDM and the extent to which CLL patients are provided the information needed to fully participate in their treatment decisions. As new CLL treatments are incorporated into standards of care, greater efforts are needed to enhance SDM across the care continuum. For patients with lower education levels and/or those in first-line treatment, there is a need for stronger patient education and enhanced communication with providers around new treatment options. These findings constitute an important step toward understanding how patients are informed about new treatments, which impacts SDM for CLL and treatment choices for patients and is critical given the overwhelming number of treatment options available. Increased patient education and PPC around new treatment options for CLL has the potential to improve the engagement of disadvantaged groups in treatment decisions (28) and maximize quality of life (22). Further, while these results focus on CLL treatment conversations, they may have implications for other cancers or illnesses in which rapid therapeutic advances in treatment are leading to a more chronic experience for patients, including long-term surveillance and management of disease. To this end, cancer patients facing first—and subsequent—lines of therapy should be educated on all available treatment options to encourage SDM. Given the evolving treatment landscape and increasingly chronic nature of many cancers, oncology providers are in a unique and important position to engage patients actively and continually in discussions about treatment options, including novel agents and recently approved therapies.
Footnotes
Authors’ Note
Participants provided informed consent electronically prior to participation. Participants were informed that this research study would be published and consented to publication. No animals were involved in the conduct of this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional research policies and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
1. Elissa C. Kranzler is currently at Fors Marsh Group, Arlington, VA, USA.
2. Shauna McManus is currently at OPEN Health Evidence & Access, Bethesda, MD, USA.
Declaration of Conflicting Interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Financial research support was granted to the CSC and not individual study authors. CSC retains full control of all primary data. CSC shares control over data analyses and reporting of results with AstraZeneca, one of several project funders. Potential conflicts of interest are as follows. Dr Kranzler: Astellas Pharma US, Inc, Janssen Oncology, Jazz Pharmaceuticals, Pharmacyclics, Inc, Takeda Oncology (institutional research support). Dr Buzaglo: Concerto HealthAI (employee). Dr Zaleta: Astellas Pharma US, Inc, Gilead Sciences, Inc, Novartis, Pfizer, Inc, SeaGen Inc. (institutional research support). Drs Olson, Nichols, Yuen, and Ms. McManus have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by AstraZeneca. Funding for the Cancer Experience Registry was provided by AstraZeneca, Genentech Inc, Janssen Oncology, Novartis, and Pharmacyclics, Inc