
Abstract
Emergency department (ED) utilization changed notably during the coronavirus disease 2019 (COVID-19) pandemic in the United States. The purpose of the study was to gain a more thorough understanding of ED patient experience during the early stages of the COVID-19 pandemic. This study used the consensual qualitative approach to analyze open-ended responses from post-ED patient experience surveys from February through July 2020. Comments were included in the analysis if they pertained to care during the pandemic (eg, mentioned “the virus,” “masks,” “PPE”). A total of 242 COVID-specific comments from 192 unique patients were analyzed (median age 49 years; 69% female). Six themes were identified: visually observed changes, experiences of process changes, expressions of understanding or appreciation, sense of security, COVID-19 disease-specific comments, and “classic” satisfaction comments that align with previous literature on patient experience. The COVID-19 pandemic has challenged health care systems across the world in unique and unprecedented ways. This study identified six themes that better elucidate ED patient experience during an unprecedented public health crisis.
Introduction
Patient experience in the emergency department (ED) is a continuously growing area of research and focus of health care leadership (1,2). High patient experience scores are associated with improved patient-oriented outcomes and value-based financial incentives, including profitability, competitive marketplace positioning, and optimized reimbursement (3). Further, improvement in patient experience has been suggested to improve patient adherence to recommended care (4), readmission rates (5), health outcomes (4), and mortality (6).
The complexity and depth of ED patient experience are particularly critical to understand, as the ED serves as the initial access point to the health care system for many and up to 67% of hospital admissions present through the ED (7). However, ED patients’ experiences and satisfaction with care generally perform lower compared to other health care settings. This lower satisfaction is likely due to a myriad of factors unique to the ED, including overcrowding, wait times, ineffective communication, and lack of patient privacy (1,2,8 –11).
Emergency department utilization and presentation of disease changed notably during the coronavirus disease 2019 (COVID-19) pandemic in the United States. Overall ED utilization decreased, while COVID case presentations increased remarkably (12 –15). Researchers theorize that prospective ED patients were hesitant to seek out emergency care unless absolutely necessary due to fear of COVID-19 exposure as well as the unintended consequences of public health recommendations to minimize nonurgent health care, stay-at-home orders, and lifestyle changes (12,15,16). As a result, major medical organizations launched advertising campaigns encouraging people to avoid delaying medical care (17,18). During this period of overall decreased ED utilization, a significant improvement was seen in measurable scores of ED patient experience compared to typical performance trends, despite the unprecedented stress experienced by the ED and overall health care system (19). As such, it is important to better understand the ED patient experience during the COVID pandemic to identify the possible areas for intervention and optimization of emergency care delivery in the future. The purpose of the study is to better understand patients’ experiences of ED care during the early stages of COVID through qualitative analysis of responses to open-ended patient experience survey questions.
Methods
Study Design
This study used the consensual qualitative approach to analyze open-ended responses from patient satisfaction surveys from ED visits during the early stages of the COVID pandemic. The study was reviewed and approved as non-human subjects research by the institutional review board.
Study Population
ED Press Ganey (PG, Press Ganey Associates) patient satisfaction surveys were the data source. The PG surveys were sent electronically (via email) to discharged patients who visited a large, urban, academic medical center ED in Chicago, Illinois, as part of routine postvisit quality improvement processes (∼94 000 annual visits in fiscal year 2019). Patients received the PG survey link three days after their visit if a valid email address was recorded within the health system electronic record. Patients were excluded from receiving the survey if they were admitted to the hospital, were discharged to a location other than home (eg, prisoners), if they had visited the ED and been surveyed within the prior 30-day period, or if they previously indicated they did not want to be surveyed. Analyzed surveys were those returned from March 1 through July 8, 2020, representing ED visit dates from February 16 through July 7, 2020.
Measures
The PG survey has six survey sections: arrival, doctors, nurses, personal issues, family or friends, and overall assessment. Each section has both closed-ended questions and an open-ended (free text) comments section. The open-ended comments section states: “Comments (describe good or bad experience).” For this analysis, closed-ended questions were not analyzed. All open-ended survey responses were compiled and reviewed independently by two reviewers (DMM, TML) to determine the final sample for analysis. Comments were included if they pertained to COVID, based on a set of key phrases related to the pandemic (eg, COVID, pandemic, the virus, isolation, distancing, 6-feet, mask, cleaning, visitor restrictions). Comments were excluded if they made no reference to the pandemic or related concepts. Discrepancies between reviewers were resolved through conversation to reach consensus.
Patient sex, age, race, ethnicity, visit time of day (check-in 7
Analysis
The free-text comments were analyzed using qualitative content analysis employing a consensual qualitative research approach (20). The consensual qualitative method utilizes a primary coding team and a secondary audit team. For this study, the primary coding team consisted of one attending ED physician (DMM) with expertise in qualitative methodology and three ED resident physicians (VPK, DAL, SBK). The secondary audit team (TML, TAD) have expertise in ED clinical operations and patient experience.
Using an inductive content approach, the primary coding team independently coded a 20% subsample of comments. Each text passage could have more than one code applied. The team subsequently reconciled their codes and developed an initial coding framework. Iterative rounds of independent coding and group review and reconciliation continued with modifications of the coding framework as appropriate until all data were coded.
The primary coding team then determined themes; all text, codes, and themes were submitted for secondary audit team review. Themes were revised based on audit team feedback. Themes are presented with description of their definition and sample quotes; however, proportions of responses within a given theme are not routinely used in this form of qualitative inquiry. Strategies used to increase the trustworthiness of the analysis were analyst triangulation (both with the initial coding team and by the use of an audit team), memoing, and reflexive journaling. Demographic characteristics are reported using descriptive statistics as appropriate.
Results
A total of 1851 patient comments from 660 patients were collected during the study period. After initial review, 242 comments from 192 unique patients met inclusion criteria as being COVID-specific comments. The median age of respondents was 49 years (interquartile range 38-64 years) and 69% were female (Table 1).
Characteristics of Survey Respondents.
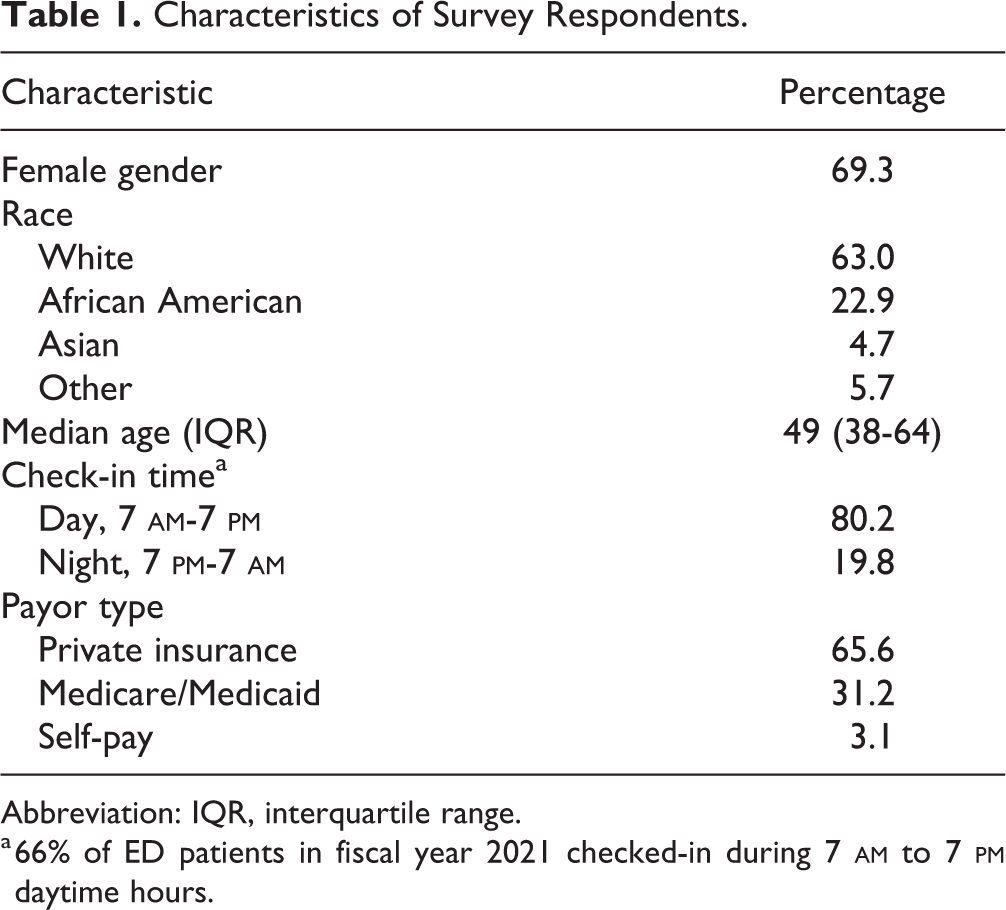
Abbreviation: IQR, interquartile range.
a 66% of ED patients in fiscal year 2021 checked-in during 7
Twenty-one codes were identified which ultimately resulted in six themes. The audit team found no additional independent themes; however, did influence the wording of the themes and added nuance to their interpretation.
Themes
Each of the six themes and representative quotations are presented in Table 2 and described in brief below.
Themes and Representative Quotes.

Abbreviations: COVID, coronavirus disease; ED, emergency department; PPE, personal protective equipment.
Visually observed changes
Patients commented on the measures of disease prevention they could observe (or did not observe) during their visit. These changes included the use of personal protective equipment (PPE) as well as cleaning and social distancing practices and were both positive and negative in tone. For example, one patient noted “it was comforting to see the chairs spaced so far apart.” Comments related to PPE were often observations of missing PPE (“noticed a few staff not wearing masks”) or appeals to get more PPE for staff (“PLEASE GET THEM FACE SHIELDS FOR DOING THOSE TESTS!”). Comments related to cleaning practices tended to note their presence in general terms (“I felt safe with the care the staff took in handling my admission with social distancing and cleanliness of the check in process”), but their absence with specific details (“No Lysol wipes available to wipe off seats” or “no evidence of recent cleaning or disinfection of patient waiting area immediately before or during the 2 hours I waited”).
Experiences of process changes
Patients noted how new process changes within the ED were affecting their experience. These changes included visitor restrictions, patient isolation, limiting staff in rooms, an outside waiting area implemented for distancing, as well as a dedicated “COVID testing tent” in the ambulance bay. Comments ranged from simple statements of fact (“we had to wait outside”) to voicing accompanying opinions of the process changes (“I had to wait outside in the cold for over ten minutes due to the assessment of my symptoms being incorrect. This was absolutely horrible.”). Comments further conveyed feelings of loneliness and frustration associated with the changes in visitor policies. One patient poignantly noted, “I know we are all learning during the pandemic but I was not comforted or talked to much. I was mostly left alone and not told much.”
Expression of understanding or appreciation
Patients included statements expressing both their understanding of how their care was being delivered and appreciation for ED staff. Patients used terms such as “understandably” or “appropriately” seeming to acknowledge that while not the norm or ideal, the rationale behind the process changes was understood. For example: I gave it a very good experience even though I was waiting outside because I understand the time we are living and circumstances that it’s understandable why we wait outside until we are called.
Sense of security
Patient comments highlighted their fears of coming to the ED during the pandemic, but also discussed their sense of safety within the ED. Patients reported feeling “comfortable and safe within the waiting area,” based on distancing practices. Thoughts of fear and anxiety about presenting to the ED during a pandemic were also captured, such as: Because of the COVID 19 threat, I was afraid to go to the ER. My fears was [sic] assuaged, things could not have been more sanitary and efficient. I was handled with great efficiency and taken to a treatment room almost immediately.
COVID disease-specific comments
Patients commented on the symptoms of and testing for COVID, or on the amount of focus placed on the virus within the ED. For example, one patient was “frustrated with decision made not to test” for COVID, while others noted how “very uncomfortable” the actual testing procedure was. Additionally, patients perceived “care providers were too concerned about COVID-19” and were not focusing on their individual symptoms. For example: She is a long time patient of [hospital], possibly over 30 years! Never experienced the lack of focus on what the real problem may be when coming to the ER. Understanding the seriousness of Covid…it became the only thing they were willing to focus on.
Classic satisfaction comments
Although not unique to the current pandemic, comments that otherwise met inclusion criteria additionally had content related to “classic” patient satisfaction categories such as communication, interpersonal skills, and wait time. One patient noted he “wasn’t informed of any delays…I was surprised when someone came to give me an x-ray, because it hadn’t been mentioned”; whereas others described positive interpersonal interactions with staff (“The doctor were [sic] awesome and my first nurse…had a good sense of humor and helped my anxiety greatly!”).
Discussion
This qualitative analysis of ED patient experience comments during the early phases of the COVID-19 pandemic resulted in six themes related to both the observed changes and personal experiences of care during a pandemic. To our knowledge, comments about the types of changes patients were able to “visually observe” as well as their “experience of process changes” have not been identified previously in the literature related to the COVID-19 pandemic. Although increased attention to these topics is understandable given the transmissibility of COVID and preventative measures in other facets of life (eg, grocery store), they are nonetheless worthy of discussion as they confirm that patients are perceptive of the presence or absence of these measures. Given the newfound public awareness to disease transmission and processes to mitigate risk, targeted communication of patient safety policies and procedures as well as targeted staff education that these behaviors are closely observed may improve the patient experience.
Targeted communication could also be a strategy to improve negative experiences in the “COVID disease-specific” theme. A recent study, outside of the context of COVID, suggests that confusion about care procedures is an important factor in the patient experience (9). The negative experiences stemming from lack of testing or testing discomfort align with the oft cited “disconfirmation paradigm,” which suggests that perceptions of a service encounter are characterized by either confirmation or disconfirmation of expectancies (21). In contrast, disappointment or confusion with not receiving testing and discomfort with the swabbing procedure itself are less likely modifiable by communication, as these negative experiences are linked to the outcome (eg, no test or discomfort) being misaligned with the patient expectation.
The “sense of security” theme extends findings from prior ED patient satisfaction studies during nonpandemic times (22), and further underscores the importance of addressing the patients’ psychosocial and emotional needs. Emotions of fear and isolation, safety and security, as well as understanding and thanks were seen across several of the themes. The pervasiveness of the comments also suggests that proactively addressing these needs may be even more important during times of disease outbreak, pandemics, and disaster, when clinician attention is likely diverted to the more “immediate” medical concerns, and psychosocial and emotional needs might be inadvertently deprioritized.
The “classic satisfaction comments” theme similarly replicates findings from prior ED patient experience studies (1,8,22,23) but may hold new meaning during the COVID-19 pandemic. One of the classic topics, wait times, has long been identified as a key driver of patient satisfaction in the ED (1,8,23 –25). Positive wait time comments may have stemmed from the aforementioned disconfirmation paradigm (21), where patients were expecting even worse wait times because of the pandemic but were met with shorter times as perceptions of wait time are more predictive of satisfaction than actual waiting times (26 –28). Comments similarly underscored the significance of interpersonal interactions, which is also supported in previous studies (22,26,29,30) and perhaps heightened during times of disaster and pandemics. All of these “classic” comments serve as a reminder that, even in extreme times, the core drivers of satisfaction persist.
A recent publication by Jehle and colleagues described the trend of increased patient satisfaction scores amidst the pandemic (19). One possible explanation for the increased satisfaction and the positive themes identified in this study is the perceived acuity of visits during COVID-19. With increasing level of acuity, patients’ satisfaction improves (26,31). This phenomenon, labeled the ‘‘point of view paradox,’’ describes that as the severity of illness increases, a converse decrease in patient expectations regarding nonclinical service factors occurs (32). Even for those patients without a personal high level of acuity, it is possible that the positive comments and expressions of understanding stemmed from the perceived “acuity” of the general pandemic situation and well-publicized stressors on the health care system.
This study has several limitations. It was a single-center study relying on post-visit patient comments and thus is limited in generalizability and subject to recall bias. There is no way to ensure that the patient themselves responded rather than a family member. The PG survey itself has been previously questioned regarding representativeness of opinions of the ED patient population, it’s validity, and that several factors may influence survey response rate (eg, patient age, sex, insurance status, physician characteristics) (33 –37). Although limited, PG surveys have been shown to identify similar qualitative information to online reviews from patients (38). Responses may have been richer and follow-up questions could have been asked if the study was conducted prospectively or with a customized interview guide rather than utilizing data originally collected for quality improvement; however, this prospective strategy was not feasible for our study team during the early stage of the pandemic. Additionally, the sampling frame was determined based on survey return date rather than ED visit date, so a response rate was not calculated; however, the average survey return rate for our health system is 75%.
As with all qualitative studies, the study team’s views and opinions may have influenced comment inclusion in the final sample, coding, and thematic analysis. To combat this potential bias and maximize the inclusion of responses in the final sample, we used a double coding process for comment inclusion and consensual coding techniques including an audit team for analysis. Additionally, the coding teams had gender, role (resident, attending), and subspecialty training (operations, research) diversity and incorporated a non-physician with expertise in patient experience to mitigate any bias. Finally, no quantitative satisfaction scores were analyzed for this sample, limiting the ability to draw conclusions about how patients “weighted” these comments in their overall satisfaction with their experience. The choice to focus on qualitative data was deliberate and offers the ability to more deeply understand the patient experience rather than looking at experience as a lens to satisfaction. Evaluating patients’ words alone allows one to obtain a more detailed understanding of their experience than one obtained from quantitative approaches, which are inherently reductive and limit the patients’ voice.
Conclusion
The COVID-19 pandemic has challenged health care systems across the world in unique and unprecedented ways. This study identified six themes that better elucidate the patients’ experience in the ED during an unprecedented public health crisis. These themes support the idea that, in this crisis setting, patients were observant of safety procedures and the context of the pandemic, while also still commenting on more traditional satisfaction domains, such as communication. Although the pandemic has placed great stress on the health care system, this stress can act as a crucible for change, during which new study can identify areas for intervention and galvanize change, such as improved communication about safety policies and procedures.
Footnotes
Authors’ Note
This study was approved by the Institutional Review Board (IRB Study #STU00213059). All procedures in this study were conducted in accordance with the Institutional Review Board (IRB Study #STU00213059) approved protocols. Informed consent is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.