
Abstract
Integrating satisfaction measures with pain-related variables can highlight global change and improvement from the patients’ perspective. This study examined patient satisfaction in an interdisciplinary chronic pain management program. Nine hundred and twenty-seven (n = 927) participants completed pre- and post-treatment measures of pain, depression, catastrophizing, anxiety, stages of change, and pain acceptance. Multiple regression was used to examine these variables at admission and discharge as predictors of patient satisfaction. Pain-related variables explained 50.6% of the variance (R2 = .506, F 22,639 = 29.79, P < .001) for general satisfaction, and 38.9% of the variance (R2 = 0.389, F 22,639 = 18.49, P < .001) for goal accomplishment. Significant predictors of general satisfaction included depression (β = −0.188, P < .001) and the maintenance stage of change (β = 0.272, P < .001). The latter was also a significant predictor of goal accomplishment (β = 0.300, P < .001). Discharge pain-related measures are more influential than admission measures for predicting patient satisfaction. Patient satisfaction is significantly related to establishing a self-management approach to pain.
Keywords
Introduction
The value of attending a chronic pain management program lies with a patient’s expectation to live a life undeterred by chronic pain. At the end of a program, patients reflect on their experiences via satisfaction questionnaires. These questionnaires prompt reflection ranging from self-assessment of improvement to further recommendation and feedback to the treatment team (1,2). Satisfaction scores reflect a patient-centered view of global improvement, and are typically used for administrative purposes and further planning. Pain is a complex biopsychosocial problem and many factors can influence an individual’s pain experience and interpretation of improvement (3 –7). The changes that patients make in a chronic pain management program may affect their evaluation of satisfaction with treatment. When patients begin a program, they may be in different stages of understanding their pain (8).
Patient satisfaction is a facet of patient-centered care (9). Patient perspectives of accomplishment and progress may differ from those of the health care provider (1). With chronic pain, patient feedback may be related to future adherence to self-management methods (10). Feedback can shed light on patients’ general attitudes toward their chronic pain as they leave the program. But health care providers may be uncertain about how well patients can evaluate their own changes, or how they compare and evaluate their past and present states (10,11).
Satisfaction questionnaires can be anchored with outcome measures to examine the value of psychological changes from a patient-centered perspective. Scores on pain-related variables, which change significantly from admission to discharge (12) can capture many aspects of patient experience. It is worth exploring how patients notice these changes in themselves.
The purpose of this study was to examine patient satisfaction in an interdisciplinary chronic pain management program. Pain-related variables assessed at admission and discharge from a 4-week program such as pain intensity, pain-related disability, depression, anxiety, catastrophizing, stages of change, and acceptance of pain were used as predictors of patient satisfaction.
Materials and Methods
Participants
Adult patients admitted into a 4-week chronic pain management program over an 11-year period (2006-2017; n = 927) participated in this study. These individuals had chronic pain of heterogeneous clinical manifestations and comorbidities. They previously attempted multiple pain treatment methods, attained no lasting pain relief, if at all, were unsure of how to cope with their pain, and had significant impairment in their daily functioning. Participants were referred to the program by the Worker’s Safety and Insurance Board, motor vehicle accident insurance companies, family physicians/medical specialists, lawyers, and Veteran Affairs/Department of Defense.
Prior to participation, all patients attended an orientation session introducing them to the program and to viewing pain as a complex biopsychosocial phenomenon rather than just a biomedical one. They were then assessed by an interdisciplinary team consisting of a physician, occupational therapist or social worker, and psychologist, evaluating the physical/medical, functional, social, and psychological aspects of their pain problems, respectively. Inclusion criteria for the program were ≥ age of 18, self-reported chronic pain for ≥ 6 months, absence of a terminal illness or psychotic disorder, independence in activities of daily living, no falls risk, and expressed intention to actively work on goals designed to improve function in areas such as productivity, exercise, recreation, nutrition, and overall health. The program has been previously described by Williams et al (2007) (13). In brief, patients attend a 4-week interdisciplinary chronic pain management program based on the biopsychosocial model of assessment, prevention, and treatment of chronic pain. Interventions include fitness, psychoeducation, group therapy, pharmacy assessment, relaxation and mindfulness sessions, yoga, and hydrotherapy, among other sessions. The interdisciplinary treatment team consists of a physician, psychologist, psychometrist, social worker, physiotherapist, occupational therapists, pharmacist, dietician, and support staff. At initial assessment, all participants signed an informed consent form allowing for the use of their information for research and program quality improvement purposes.
Measures
Patients completed questionnaires on pain-related variables at admission and discharge, a demographic information questionnaire at admission, measures of goal accomplishment, and program satisfaction at discharge.
Pain-Related Outcome Measures
Pain Intensity Scale
The Pain Intensity Scale (PIS) assesses pain intensity on a scale of 0 to 10, with 0 indicating no pain and 10 indicating unbearable pain. Patients rate their least and usual pain in the past 2 weeks. The 2 values are then averaged into one single score used for analysis. The PIS is a reliable and valid measure of the intensity of pain sensation with the average of least and usual pain found to be the best predictor of present pain (14).
Center for Epidemiological Studies-Depressed Mood Scale
The Center for Epidemiological Studies-Depressed Mood Scale (CES-D) was used to assess symptoms of depressed mood experienced in the past week (15). It consists of 20 items, with responses ranging from 0 (rarely or none of the time) to 3 (most or all of the time). The CES-D was found to be a valid measure of depressive symptoms in the general and chronic pain populations. It has demonstrated superior sensitivity in identifying differences in depression severity when compared to other depression scales such as the Beck Depression Inventory (16). While a total score of 16 indicates depressed mood in the normal population, a score of 19 suggests depressed mood in the chronic pain population, preventing significantly higher classification of depression (17,18). A score of 27 is considered to be the cutoff for classifying someone as clinically depressed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) (16).
Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCS) was used to assess catastrophic thinking, which is defined as an exaggerated negative orientation toward the threat of actual or anticipated pain. There are 13 items with responses of 0 (not at all) to 4 (all of the time) describing perceptions and feelings toward pain and pertain to 1 of 3 subscales: rumination, magnification, and helplessness. The PCS has demonstrated convergent validity with self-reported anxiety measures and strong test–retest reliability (19).
Clinical Anxiety Scale
The Clinical Anxiety Scale (CAS) measures clinical anxiety using a scale from 1 (rarely or none of the time) to 5 (most or all of the time). The CAS has been shown to be a reliable measure indicated by a high internal consistency (α = .94) and good discriminant validity (r = .77) (20).
Patient Questionnaire of the Primary Care Evaluation of Mental Disorders (PQ, PRIME-MD)
The Patient Questionnaire (PQ) of the PRIME-MD assesses physical and emotional symptoms experienced in the past month with 25 true or false questions and a self-rating of overall health as “excellent,” “very good,” “good,” “fair,” or “poor.” The PQ is a useful tool in screening mental disorders demonstrating good to excellent sensitivity across all diagnoses: mood (69%), anxiety (94%), alcohol (81%), and eating (86%) disorder (21).
Chronic Pain Acceptance Questionnaire
The Chronic Pain Acceptance Questionnaire (CPAQ) measures acceptance of chronic pain with 20 items between 2 subscales, activity engagement and pain willingness. Response options range from 0 (never true) to 6 (always true). The CPAQ has demonstrated very good internal consistency (α = 0.82 for activity engagement and α = 0.78 for pain willingness) (22,23). It has also demonstrated predictive validity for depression, pain-related anxiety, and psychosocial disability (22).
Pain Stages of Change Questionnaire
The Pain Stages of Change Questionnaire (PSOCQ) measures readiness to adopt a self-management approach to chronic pain (8). Participants rate statements using a scale from 1 (strongly disagree) to 5 (strongly agree). Each item loads onto 1 of 4 subscales: (A) Pre-contemplation: Believing that the problem is mostly medical and that pain relief is left up to physicians. (B) Contemplation: Willing but reluctant to adopt a self-management approach to chronic pain. (C) Action: Reflecting on the acceptance of a self-management approach and engageability in such treatment. (D) Maintenance: Reflecting an established self-management approach and intention to continue this approach. If the individual scores high on contemplation, action, and maintenance, they are more likely to benefit from treatment that involves learning self-management strategies. The PSOCQ has demonstrated very good to excellent reliability for each subscale: precontemplation (α = .77), contemplation (α = .82), action (α = .86), maintenance (α = .86), and excellent test–retest reliability (α = 0.74-0.88). Validity is further supported by the association with treatment outcome (24), usefulness in predicting commitment in self-management, and relationships with other pain-related measures (13).
Satisfaction Questionnaires
Pain Program Satisfaction Questionnaire
The Pain Program Satisfaction Questionnaire (PPSQ) was developed based on the Client Satisfaction Questionnaire (CSQ) used to assess patient satisfaction in mental health treatment (1). Some items from the CSQ were adapted for use on the PPSQ. Additional items were devised by one of the authors to make it more relevant for chronic pain. The PPSQ consists of 11 questions each rated on a 4-point Likert scale, and 2 open-ended sections (Online Appendix 1). Out of a maximum score of 44, patients rate their satisfaction with program services and may also provide written comments. The first open-ended section asks patients to list any problems that the program helped them with, other than pain. The second open-ended section asks patients to provide comments regarding their experience in the program. The main themes expressed by patients in these comments were impact of a strong interdisciplinary team, learning to adapt in order to manage, the program as a stepping stone, positive effects of a group effort, improved mental health, and benefits of the program (25). Internal consistency of the PPSQ (Cronbach’s alpha) has been found to be 0.87. The criterion validity of the PPSQ was assessed by examining the correlation of the total score with staffs’ and patients’ global ratings of improvement/evaluation of goal accomplishment (Self Evaluation Scale [SES]) in the program (26).
Self Evaluation Scale
On the SES, the patient is asked to rate his/her own goal accomplishment on a 5-point Likert scale 1 (poorly), 2 (fairly), 3 (well), 4 (very well), and 5 (excellent), at the end of the program. This is followed by an open-ended section titled “comments” where one may elaborate on their perceived goal accomplishment (Online Appendix 2). The SES is used to determine the participant’s perceived performance in the program. The SES was found to be reliable and valid in assessing goal accomplishment in a multidisciplinary chronic pain management program (12,26,27).
Procedure
Patients completed 2 sets of pain-related measures at admission and discharge. At discharge, they also completed the PPSQ and SES. The university and hospital integrated research ethics board reviewed the study protocol and deemed it unnecessary to obtain ethical approval for this type of retrospective data analysis.
Data analysis
Paired t tests examined change in scores for each measure from admission to discharge. Two multiple regression analyses were performed, one for each of the 2 satisfaction measures. Analyses were performed with R ver 3.6.1 (28). The psych package was used to produce summary results (29), and the QuantPsyc package was used to calculate β values for multiple regression (30).
Results
Table 1 displays the demographic characteristics of the sample.
Demographics: Descriptive Statistics and Frequencies.a.

a Note: N reflects available data for each category.
Table 2 displays the results of the t tests along with descriptive statistics for pain-related variables and program satisfaction. Paired t test results revealed significant changes on all pain-related variables from admission to discharge. The most significant differences in scores were found within the PSOCQ subscales. Descriptive statistics for the PPSQ and SES are also displayed on Table 2. The correlation coefficient between the PPSQ and the SES is 0.66 (P < .001).
Admission and Discharge Pain-Related Measures: Descriptive Statistics and Paired t Tests.
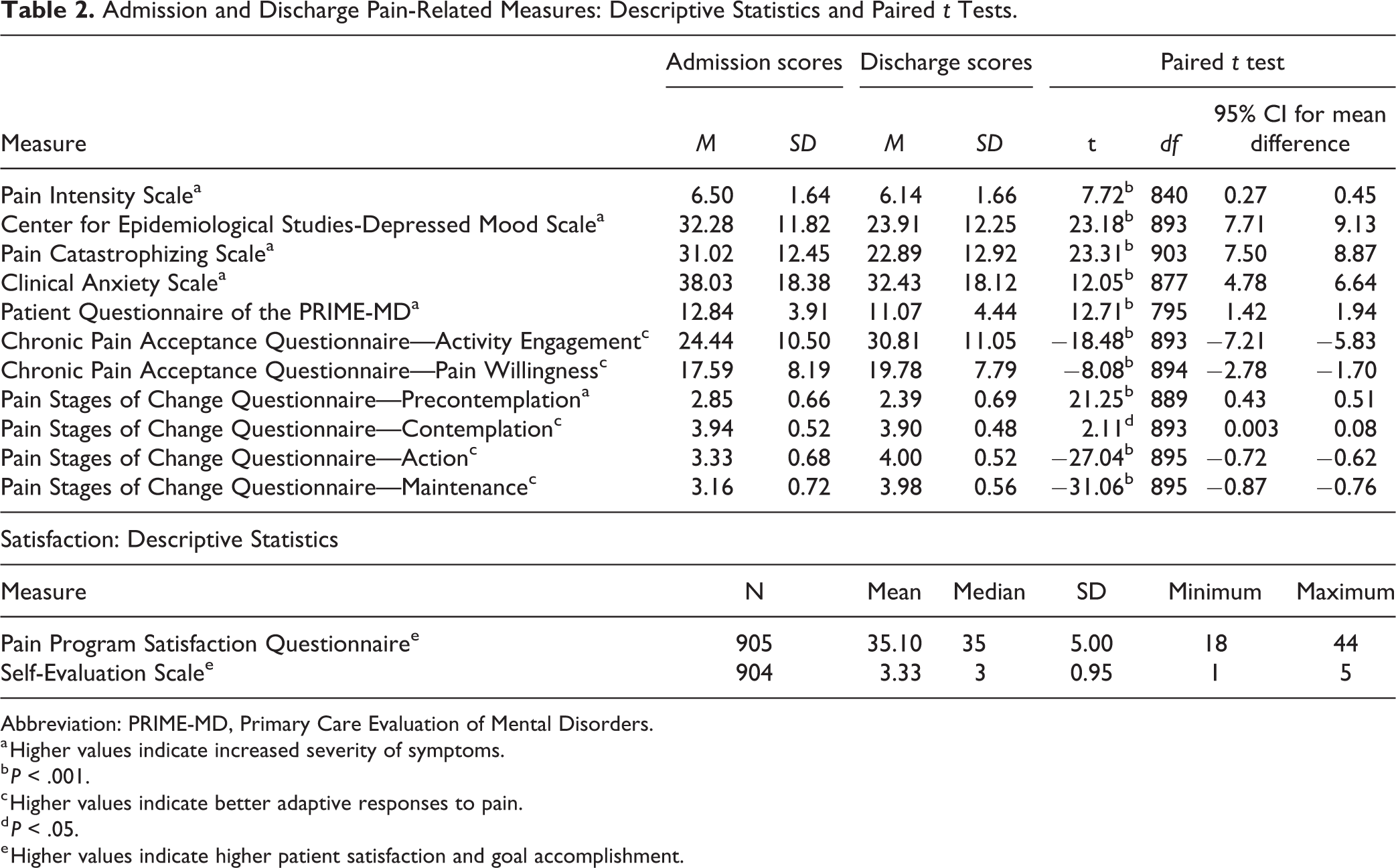
Abbreviation: PRIME-MD, Primary Care Evaluation of Mental Disorders.
a Higher values indicate increased severity of symptoms.
b P < .001.
c Higher values indicate better adaptive responses to pain.
d P < .05.
e Higher values indicate higher patient satisfaction and goal accomplishment.
Table 3 displays results of the regression analysis for the PPSQ. Admission and discharge measures explained 50.63% of the variance (R2 = 0.5063, F 22,639 = 29.79, P < .001) in PPSQ scores. Multiple subscales in the PSOCQ contributed significantly to PPSQ scores. Specifically, discharge scores in pre-contemplation (β = −0.237, P < .001), contemplation (β = 0.173, P < .001), and maintenance subscales (β = 0.272, P < .001) significantly predicted PPSQ scores. Another measure that also significantly predicted the PPSQ was discharge CES-D (β = −0.188, P < .001). Some admission measures were also significant predictors of the PPSQ, such as CPAQ pain willingness (β = −0.094, P = .009) and PQ (β = 0.091, P < .022).
Pain Program Satisfaction Questionnaire Multiple Regression Model Coefficients.

Abbreviation: PRIME-MD, Primary Care Evaluation of Mental Disorders.
a Higher values indicate increased severity of symptoms.
b Higher values indicate better adaptive responses to pain.
Results of the regression analysis for the SES are shown in Table 4. Admission and discharge measures explained 38.90% of the variance (R2 = 0.389, F 22 ,639 = 18.49, P < .001) in SES scores. Similar to the PPSQ, discharge maintenance (PSOCQ) was also a significant predictor of SES (β = 0.300, P < .001).
Self Evaluation Scale Multiple Regression Model Coefficients.

Abbreviation: PRIME-MD, Primary Care Evaluation of Mental Disorders.
a Higher values indicate increased severity of symptoms.
b Higher values indicate better adaptive responses to pain.
Of all pain-related measures used in the multiple regression analyses, data were missing at random, and consisted of 2.7% of the sample. Scores were normally distributed as examined visually through histograms, skewness, and kurtosis. Values are generally centered in distribution, with skewness values ranging from −0.52 to +0.51, and kurtosis ranging from −0.80 to 1.09.
Discussion
The purpose of this study was to examine the relationship between patient satisfaction and pain-related variables in a chronic pain management program. Satisfaction questionnaires provide an opportunity for patients to give feedback for their experience in the program. Results revealed that pain-related measures contributed differentially to the prediction of general satisfaction (PPSQ) and goal accomplishment (SES).
Pain-related variables improved from admission to discharge in line with previous findings (5,31,32). However, some pain-related variables changed more than others. Discharge scores were more influential in predicting satisfaction than admission scores. Patients may not have noticed relative changes when rating their satisfaction (33). Satisfaction was most significantly related to the discharge maintenance stage (PSOCQ), and less affected by negative mood and cognition (CES-D, CAS, PCS), even though the discharge CES-D was also a significant predictor of the PPSQ. Maintenance refers to establishing a self-management approach to pain and intention to continue with this approach. From the patient’s perspective, the leading factor in their self-evaluation of improvement is gaining agency in their pain and confidence in applying self-management techniques.
Admission–Discharge
Scores on pain-related variables changed unevenly at discharge. For example, with the PIS, admission and discharge scores were significantly different but the numerical average change was only 0.36. This is minor considering the PIS is a 10-point scale. Similar findings have been noted in previous literature (34). In contrast, scores on the CES-D differ by 26% between admission and discharge, also a consistent chronic pain management outcome (26,34,35).
In addition, scores in the action and maintenance subscales (PSOCQ) increased by 20%. Both represent latter stages in the process of attaining and actively embracing self-management approaches. After attending a chronic pain management program, patients’ pain levels remain relatively constant but significant changes occur in cognition and behavior. This pattern of change is consistent with the misdirected problem-solving model of pain (36). Patients have to overcome the perseverance loop of repeated problem-solving of overreliance on biomedical approaches. This change in problem-solving beliefs is shown with the increase in scores in action and maintenance, whereas PIS scores stay more or less the same at discharge. The pain problem has been reframed and patients now have tools for actively managing their responses to pain.
Furthermore, positive change in emotional functioning (CES-D, CAS) and attitude toward pain (PCS) suggests an overall reduction in negative mood and cognitions (37). Discharge scores on the PCS and CAS are 26% and 15% lower, respectively. It may be easier to influence change in depressed mood and catastrophizing, as compared to anxiety within the 4 weeks of the program. Anxiety in patients with chronic pain may be a more enduring state that changes more slowly over time (38,39). Patients need time to adopt and enact their newly learned pain management methods. This notion may also be reflected in the 12% increase in CPAQ pain willingness scores, which may suggest emerging long-term cognitive changes. Follow-up studies can further examine such effects.
Satisfaction Questionnaires
Two questionnaires served as final overall evaluations for patients to complete at the end of the chronic pain program. The PPSQ and the SES examined 2 different areas of satisfaction. Firstly, the PPSQ is a general satisfaction measure, combining aspects of program service satisfaction with goal accomplishment satisfaction, whereas the SES is a one-rating scale specifically about goal accomplishment. Therefore, SES results may be a subset of concepts captured by the PPSQ. This is also reflected in the moderate correlation between the PPSQ and the SES.
Pain Program Satisfaction Questionnaire
The strongest predictor for the PPSQ was the discharge maintenance score of the PSOCQ. From the patient’s perspective, the most prominent notion of change is related to gaining a sense of confidence in applying self-management approaches to everyday life. This is shown by the reduction in pre-contemplation scores at discharge and its significance as a predictor of satisfaction. From the patient’s perspective, learning these new methods may help them decrease their overreliance on biomedical solutions (8). The presence of the maintenance stage as a significant predictor may indicate that patients are actively aware of their problem-solving tendencies. Their goal of attending a pain management program is to search for other solutions. This notion is consistent with patients’ written responses in the short answer portion of the PPSQ. A common theme among their responses is using “the program as a stepping stone” (25).
Self Evaluation Scale
Overall, there were fewer significant predictors for the SES as compared to the PPSQ. Pain-related variables were less associated with goal accomplishment. The strongest predictor of goal accomplishment was also discharge maintenance (PSOCQ). Again, the maintenance stage in strong relation to goal accomplishment highlights an overarching goal of the patients, that is, to reach a point where they can self-manage their pain.
Limitations
The satisfaction questionnaires used in this study are limited to one chronic pain management program. However, a strength of this study is the long-time frame of data available, which can reveal stable long-term characteristics of individuals with chronic pain. Patients are motivated to attend pain programs after experiencing limited relief with biomedical methods (40). Results from these satisfaction questionnaires are consistent with previous findings in this program (12,25,27).
Conclusion
Patient satisfaction with pain management is related to moving away from reliance on biomedical solutions and establishing a self-management approach to pain and intention to continue with this approach. Therefore, a patient’s immediate valuable takeaways from attending a pain management program is a sense of confidence in learned skills in self-management. Further studies can examine how other pain-related variables affect patient satisfaction.
Supplemental Material
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211007834 - Patient Satisfaction With Chronic Pain Management: Patient Perspectives of Improvement
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211007834 for Patient Satisfaction With Chronic Pain Management: Patient Perspectives of Improvement by Yuelin (Cindy) Li and Eleni G Hapidou in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.