
Abstract
For children with cystic fibrosis (CF), enzymes are essential with meals to absorb nutrients and ensure adequate growth. When hospitalized, CF patients typically rely on nurse-administered medications. Recently, a pediatric hospital unit began allowing adolescents with CF enzymes at the bedside. Postimplementation, a satisfaction questionnaire was administered to participating patients and nurses measuring patient and nurse satisfaction with access to bedside enzymes versus nurse administration and overall time for enzyme delivery. The survey utilized a 5-point Likert scale. The wait time for pancreatic enzymes decreased for self-administered enzymes when compared to those that were nurse administered. All (11/11) patients and 86% (12/14) of nurses preferred the self-administration of enzymes. Hospitalized pediatric CF patients and nurses had higher levels of satisfaction with enzyme self-administration. Immediate access to enzymes in room safes impact patient autonomy, reflecting home self-care practices. Decreases in wait times optimize nutritional growth and healing while hospitalized. As a result, a new limited scope policy allowing patient-administered enzymes is now in place in the pediatric inpatient CF unit.
Keywords
Introduction
Cystic fibrosis (CF) is the most common chronic, life-threatening autosomal recessive disease in the United States (1). Self-management skills are developed over time by increasing the patient’s knowledge and self-management skill set with the intent to empower patients to take the lead in their own health. Self-management processes include the focus on illness needs which incorporates self-administration of medicines, activation of resources, and the capability to live with chronic illness (2). Cystic fibrosis self-management responsibilities should start during childhood and increase to full autonomy into adulthood. Pediatric patients with CF begin self-managing care by acquiring knowledge for prescribed medications and an understanding of daily routines, airway clearance techniques, and physical therapy activities for their CF symptoms (3).
In CF, a defect in the cystic fibrosis transmembrane regulator occurs, inhibiting epithelial ion transport and increasing thickened mucus in the exocrine glands such as the lungs, pancreas, sweat glands, and gastrointestinal tract (4). Pancreatic insufficiency (PI) is caused by the increased mucus production and an inability to discharge enough enzymes needed to promote digestion. As the large majority of patients with CF have PI, taking pancreatic enzymes before eating is required (5). A key indicator of health status for patients with CF is forced expiratory volume in once second (FEV1), which is typically higher in individuals with a body mass index (BMI) in the 50th percentile or greater (6,7). As a higher BMI is correlated with improved lung function, the importance of taking the enzymes with all meals and snacks is paramount for optimal health (8).
When hospitalized with a chronic illness, pediatric patients often trade their autonomy for dependence on healthcare professionals. This is problematic since pediatric patients with CF are often unable to perform autonomous care, such as pancreatic enzyme self-administration, within the hospital setting. The treatment plan for patients with CF admitted to the hospital should provide both the continuing capability to self-manage their illness and an active transition plan to prepare for adult healthcare (9). As such, this project sought to enhance patient autonomy with self-administration of pancreatic enzymes during hospitalization, to survey patient and nurse satisfaction with the self-administration process, and to facilitate patient transition to self-management.
Background
The American Academy of Pediatrics, American Academy of Family Physicians, and the American College of Physicians jointly recommend integrating health care transition programs into routine preventive care (10). Chronic disease self-management responsibilities should start during childhood and increase to full autonomy into adulthood (10 –12). The Cystic Fibrosis Foundation adult consensus guideline recommends developing a plan for effective interventions to facilitate transition from pediatric care to adult care. One criterion addressed in the assessment is the patient’s transition readiness related to medication management. Pediatric patients with CF begin self-managing care by acquiring knowledge for prescribed medications and an understanding of daily routines, airway clearance techniques, and physical therapy activities for their CF symptoms (3). Failure to adhere to prescribed medical plans increases the risk of complications such as pulmonary exacerbations. Ultimately, nonadherence to daily care leads to increased medical costs associated with advanced disease. It also decreases the quality of life for patients with CF and lead to premature death (13).
Published studies continue to reveal adverse effects associated with the lack of structured transitions into adult-oriented healthcare. These include medical complications, treatment issues, and medication adherence, along with patient dissatisfaction and increased emergency department/hospital use with compounding costs. This lack of preparation for transition has been reported in hospitalized adolescents and among children’s hospitals (10).
During hospitalizations, patients with CF can self-manage, as they likely do at home, to encourage autonomy with decreasing parental involvement or oversight from their medical team (14). Increasing disease-specific knowledge often sets the stage for future independence and success with prescribed treatments. For those with CF, patient self-management includes self-administration of some medications, mixing aerosol treatments, and assisting with therapies (3,15). The optimization of self-management skills in patients with CF is important throughout the individual’s lifetime. Lewis and colleagues studied patient’s ages 6 to 41years indicating medication-related skills had not been fully operationalized by young adulthood; therefore, providing opportunities for self-management skills may improve knowledge and development allowing patients with CF to manage their care, advocate for themselves, and successfully complete their daily treatment regimen in the future (16).
A study of more than 40 pediatric patients with CF showed that 31.6% considered self-management skills as the most important proficiency for successful treatment; however, few seem to be following transitional guidelines (17). For example, many patients with CF self-manage medication and treatments at home but rely on registered nurses for care during hospitalization (15).
A European study of 1269 adult patients reported an increase in patient satisfaction, from 35% to 79%, and a decrease in time required for medication administration when patients administered their own routine nonopioid medications when hospitalized (18). Similarly, it is possible for those with CF to manage their enzymes and to match their home routine even while hospitalized. Appropriate individual self-management skills must promote continued adherence with pancreatic medications to maximize the nutritional goals necessary for improved outcomes in this chronic disease (8,19).
Methods
The aim of this quality improvement project was to promote a self-management intervention for pediatric patients with CF by offering oral pancreatic enzymes at the bedside on a designated hospital unit and to measure patient and nurse satisfaction with the intervention. This project compared the current practice of nursing administered pancreatic enzymes to those self-administered by the patient with the goal of developing a policy for self-administration of enzymes at the bedside for pediatric patients with CF. The project utilized the plan-do-study-act (PDSA) model to implement the project’s change from a nurse-initiated practice to a patient-driven practice. The PDSA cycle is a widely accepted methodology for healthcare improvement (20).
A multicampus pediatric healthcare organization in the southeastern United States offers comprehensive care for a large population of patients with CF. The hospital where this project was implemented has a designated respiratory unit where all patients with CF exacerbations are admitted. On this 35-bed unit, the population of pediatric patients range in age from newborn to 20 years old.
A cadre of nurses, including the unit’s nurse educator, developed expertise caring for patients with CF and would serve as the primary nurses for this patient population. These nurses received special training on CF when onboarding to the specialized unit, as well as extensive continuous education on the topic. The nurse educator noticed an inconsistency between patients self-administering their medications at home while relying on nurses to perform the same function when hospitalized. The administration of pancreatic enzymes was particularly problematic as patients and families frequently complained to their primary nurse and nursing management about extended wait times for enzymes when ready to eat.
After appraising the scientific literature and grading the evidence, the nurse educator determined there were few studies on self-administration of medication by hospitalized patients with CF, with none in pediatrics. Additionally, the evidence indicated the importance of individuals with chronic disease learning to manage their conditions autonomously. While summarizing and appraising the literature, the nurse educator was challenged to improve the care of these patients by assisting them with age-appropriate disease management when hospitalized.
The nurse educator and nurses with CF expertise wanted to implement a medication self-administration project for hospitalized patients with CF on their unit. The nurses reasoned employing a self-management intervention would have an impact on patient, caregiver, and nurse satisfaction. An interprofessional team comprised of nurses with CF expertise, pharmacists, and pulmonologists was formed. Additional input was solicited from the CF clinic program manager, policy practice council members, child life specialists, security, and risk management. This project did not receive any form of monetary support. It was approved by the hospital’s institutional review board as nonhuman subjects research.
To take part in the self-administration pilot, the following inclusion criteria were established: patients with a CF diagnosis taking pancreatic enzymes, age 10 years and older, and children under 10 years, if the healthcare provider deemed the patient adherent. The exclusion criteria included patients with CF with pancreatic sufficiency and nonadherent patients.
Prior to implementation of the project, the nurse project leader educated the unit’s nurses on the project with training at staff meetings, utilizing teach-back methods and allowing time for the unit nurses to ask questions. Educational components included how to store pancreatic enzymes in the patient room safe for use at the bedside; patient eligibility criteria; the required provider communication; how to bar code and mark pancreatic enzymes as “pending,” then time and sign off the medication in the automatic medication dispensing system; and troubleshooting of the room safe. The nurses were also educated to audit the room safe for remaining pancreatic enzymes during transfer of care and upon discharge to ensure no enzymes were left after patient discharge. At each shift, the nurse who assumed primary care of the patient with CF would determine that the room safe was working properly and then instruct the patient on its use. If the patient was not tall enough to access the room’s wall safe, a rolling safe was utilized. As part of the implementation, the project limited the safe to a 12-hour supply of enzymes. It was reinforced to all parents that the patient was responsible for self-administration of all pancreatic enzymes. Before meals and snacks were delivered to the hospital room, the nurse would query the patient on time of enzyme dose. Timing medication administration was self-reported by the patient. A count of remaining medications in the room safe was also performed by the nurse. Removing the pending hold of the medication in the Pyxis would complete the nurse’s required documentation. Lastly, a questionnaire was conducted at discharge to assess patient satisfaction with enzyme self-administration. Similarly, the unit nurses completed questionnaires during the discharge period.
This project was implemented from April 2015 to August 2015. There were 14 patients with CF who met the inclusion/exclusion criteria during this time. To measure satisfaction with the intervention, a questionnaire was developed and offered to the participating patients and all the nurses who cared for them. The patient satisfaction questionnaire consisted of 11 questions (Supplement 1). Of the 11 questions, 3 pertained to demographics and 8 directly related to satisfaction using a 5-point Likert scale format. Participants also had a free text option for comments.
A specific process measure was the difference in wait time for self-administration of pancreatic enzymes and the traditional nurse-administered wait time. Participants were asked to pick an enzyme delivery time ranging from less than 5 minutes to greater than 30 minutes. The nurse satisfaction questionnaire had 11 questions (Supplement 2). Two questions were related to prior experience with nurse administered enzymes, one on the timing of enzyme delivery, obstacles, and patient compliance issues. Project variables to determine satisfaction level included timing of access to enzymes, a sense of autonomy, and availability of providers to order the self-administration practice.
Results
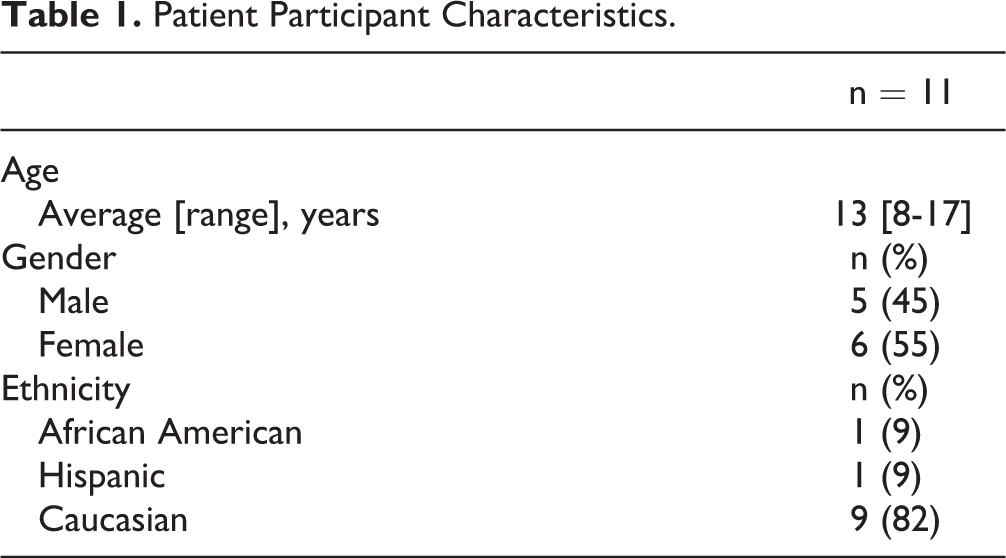
A total of 13 patients with CF consented to participate in the project. However, 2 patients with CF had significant nutritional deficits noted at admission. The healthcare team determined the patients who are ineligible and therefore excluded from the project. The remaining 11 ranged in age from 8 to 17 years and included 5 males and 6 females. The majority (82%) of the patients were Caucasian. One patient (9%) self-identified as Hispanic and 1 (9%) as African American (Table 1). Survey completion was 11/11 (100%) among participants.
Patient Participant Characteristics.
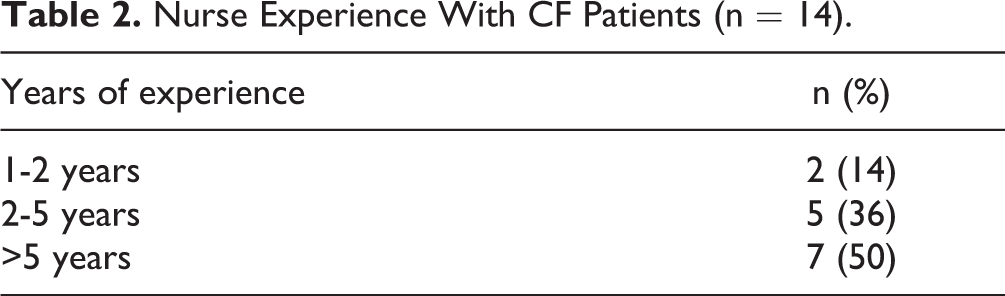
A total of 14 nurses care for these patients over the study period. Of these nurses, 50% (7/14) had over 5 years of experience caring for CF patients, 36% (5/14) had 2 to 5 years’ experience, and 14% (2/14) had 1 to 2 years’ experience (Table 2). Among these nurses, 100% (14/14) completed the nurse satisfaction survey.
Nurse Experience With CF Patients (n = 14).
Wait Times
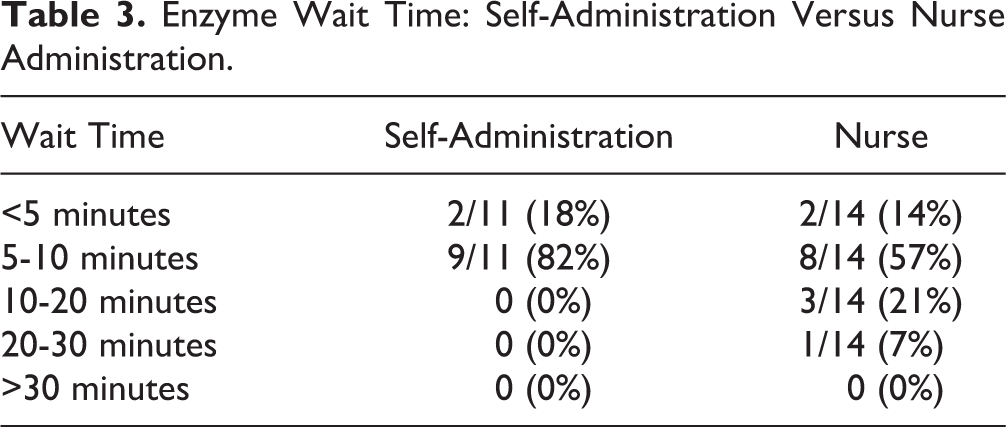
The nurse-administrated enzymes delivery ranged from less than 5 minutes to 30 minutes, with 57% (8/14) being delivered in the 5- to 10-minute window, 21% (3/14) delivered in the 10- to 20-minute window, and 7% (1/14) taking 20 to 30 minutes. For self-administered enzymes, no patient waited longer than 10 minutes to access their enzymes, with 18% (2/11) taking less than 5 minutes and 82% (9/11) taking 5 to 10 minutes (Table 3).
Enzyme Wait Time: Self-Administration Versus Nurse Administration.
Satisfaction
Patient satisfaction with enzyme self-administration was higher when compared to traditional nurse administration. All (11/11) preferred self-administration of enzymes to nurse-administered enzymes. Of those with enzyme self-administration, 73% (8/11) of the patients reported the experience as “excellent” and 27% (3/11) considered the practice “very good.”
The nurses who cared for these patients also highly preferred enzyme self-administration, with 86% (12/14) preferred the new practice of enzymes at the bedside compared to 14% (2/14) who preferred traditional nurse administration. In addition to a timelier delivery, another benefit of enzyme self-administration noted by staff on the survey is the ability to monitor the pediatric patient’s adherence to administration of enzymes in real time to the CF healthcare team. If enzymes were not self-administered on a timely basis, it was noted by the primary nurse in the medical record. In addition, this served as another source of data for the CF team to use when considering overall success with daily self-care.
One question on the survey elicited feedback from the patient on their experience with enzyme self-administration. The following free text survey comments were transcribed: “I love having immediate access to enzymes,” and “why can’t I do more of the regular scheduled medications as self- administration?” These responses reinforce satisfaction with enzyme self-administration.
After questionnaires revealed high satisfaction from patients and nurses with enzyme self-administration, and a preference for self-administration as the desired delivery method for pancreatic enzymes, the intraprofessional team met to draft a limited scope policy. The final draft of the policy was submitted to the organization’s Clinical Practice Council for review and was approved. Hospital administration believed the policy was beneficial for this patient population and approved it, as well.
Discussion
Currently, adolescent adherence to pancreatic enzyme supplementation is below 50%, but it has found to be lower with snacks than meals (21,22). Poor medication adherence has been linked to a decline in health outcomes such as pulmonary exacerbations and a decline in baseline pulmonary function. Thus, medications at the bedside may promote consistency in medication use and improve those outcomes for the patient with CF. Additionally, there is a high level of satisfaction with the ability to continue self-care reported by patients with CF practicing pancreatic enzyme self-administration at the bedside (22). Adolescents in particular want to be engaged in their care and have greater autonomy. Therefore, this intervention may sustain self-management and increase adherence because of no lapse in medication self-administration by the patient with CF.
Goodfellow et al examined advancing age in patients with CF and reduced adherence to medical therapy because of privacy concerns and time pressures as major barriers to adherence. This further reinforces self-administration of pancreatic enzymes may aid in removing those barriers. As a result of this quality improvement project, eligible patients with CF may participate in the innovative practice of self-administration of a medication while hospitalized to aid the successful transition from pediatric healthcare to adult-oriented healthcare while improving health outcomes, adherence, and self-management of CF as a chronic illness.
Limitations
As noted, the sample size was small for the project as it was only piloted on the designated respiratory unit where CF patients receive care. The only measure chosen was enzyme wait time and satisfaction for patients and nurses. In retrospect, other outcome measures such as reports of abdominal pain, amount of weight gain, and length of stay could have been included. Finally, the initial discussion period was spent forging consensus from various stakeholders that a new limited scope policy would ultimately be required if bedside self-administration of pancreatic enzymes proved beneficial to patients and nurses. Consensus among key stakeholders to this limited scope policy and updates unexpectedly took more time than anticipated as this was a major departure from traditional nurse administration of all medications.
Conclusion
The implementation of self-administered pancreatic enzymes at the bedside for patients with CF proved successful on a designated respiratory unit as evidenced by an increase in patient and nurse satisfaction and a decrease in maximum wait time for enzymes by those self-administering enzymes. The implication for nursing is that care of hospitalized patients with CF should mirror home self-management practices to increase patient satisfaction as well as nurse satisfaction. Immediate access to prescribed pancreatic enzymes with bedside storage in a room safe increases patient autonomy and decreases wait time for prescribed enzymes, optimizing nutritional growth and healing for the patient. This practice change validates that patients with CF are active participants on the healthcare team and in the management of their care. As a result, reinforcement of self-management practices whether at home or hospitalized could aid in the transition readiness process toward self-care skill acquisition leading to independence into adulthood.
Future Implications
Healthcare professionals must advocate for pediatric patients with chronic illness and provide care that supports adherence with medical treatment plans and a transition process that will allow for success in the adult-oriented healthcare system. Pediatric patients with CF must be provided a transition program that promotes education and opportunities for age-appropriate self-management skills to increase autonomy and higher quality of life. This mirrors the Cystic Fibrosis Foundation’s recommendations (23). Opportunities for age-appropriate disease self-management can improve satisfaction while promoting autonomy even while hospitalized in the pediatric setting.
Supplemental Material
Supplemental Material, sj-docx-1-jpx-10.1177_2374373520981490 - Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration
Supplemental Material, sj-docx-1-jpx-10.1177_2374373520981490 for Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration by Brandi Middour-Oxler, Margaret Gettis and Betsy Dye in Journal of Patient Experience
Supplemental Material
Supplemental Material, sj-docx-2-jpx-10.1177_2374373520981490 - Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration
Supplemental Material, sj-docx-2-jpx-10.1177_2374373520981490 for Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration by Brandi Middour-Oxler, Margaret Gettis and Betsy Dye in Journal of Patient Experience
Supplemental Material
Supplemental Material, sj-pdf-1-jpx-10.1177_2374373520981490 - Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration
Supplemental Material, sj-pdf-1-jpx-10.1177_2374373520981490 for Decreased Wait Time and Increased Satisfaction With Bedside Pancreatic Enzyme Dosing for the Inpatient Adolescent With Cystic Fibrosis: A Quality Improvement Project Comparing Enzyme Self-Administration to Nurse Administration by Brandi Middour-Oxler, Margaret Gettis and Betsy Dye in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.