
Abstract
The adoption of Community-Based Participatory Research (CBPR) approaches has increased due to its potential to reduce health disparities through Community-Academic Partnerships (CAP). Providing community members (CM) capacity-building opportunities is a way of empowering communities and promoting social change. To support the development of CAPs, the Community Training Institute for Health Disparities (CTIHD) was created in southern Puerto Rico to capacitate community leaders in the CBPR approach and basic research knowledge through the CTIHD-Community Research Program (CRP). In 2019, six syllabi-led courses were developed and implemented utilizing a problem-based curriculum design and competency-based learning model, with 12 community members enrolled. A mixed methodology assessed satisfaction, acceptance, feasibility, retention rate, and knowledge change from cognitive debriefing with semi-structured questions (qualitative), course evaluations, attendance, program documents, and pre-and post-tests (quantitative). Results indicate high levels of satisfaction from courses and retention rates of 100% and 91%, respectively. Post-course evaluation scores exceeded 70% in five of six courses, with two courses demonstrating statistically significant results (p < .05). Cognitive debriefing results indicate the feasibility and acceptability of the curriculum with suggested modifications in practical applications, itinerary of courses, and research proposal development. The outcomes of the program include the formation of four partnerships and the development of three research proposals. Capacity-building efforts, such as those of the CTIHD-CRP, are essential to increase community participation in health research, foster the formation of Community-Academic Partnerships (CAPs), and support the development of research on health disparities in the long-term.
Introduction
Capacitating and empowering community members (CM) in research is not just about promoting social change (Allen et al., 2011) but is vital in enhancing trust building between the community and academia, improving participation in research, facilitating knowledge translation and uptake, and fostering sustainable community-academic partnerships to increase the development of relevant health disparities research (Boyd & Patel, 2014; Krishnamurthi et al., 2016; Robbins & Royer, 2015; Shah et al., 2023). Community-based participatory research (CBPR) is an equitable research approach involving collaboration between researchers, organizations, and community members throughout all stages of the research process. This collaborative approach addresses health disparities and promotes social change by combining scientific inquiry with community engagement and action (Kreider, 2018; Lachowycz & Jones, 2011). Furthermore, CBPR is founded on the principles of collaborative and participatory involvement of all members that form a Community-Academic Partnership (CAP).
Facilitating CM’s access to CBPR-based community research capacitation programs promotes community empowerment, shared power, and mutual benefits of CAP members (Andrews et al., 2013). Additionally, it reduces barriers to CAP formation, such as cultural and communication challenges (e.g., differences in terminology and communication styles, mutual presumptions) and power dynamics and equity issues (e.g., decision-making authority, equitable participation, a legacy of historical mistrust; University of North Carolina at Chapel Hill School of Government, 2023). Among the principles that guide CBPR, we identify that training community partners is critical for the integration and equal participation of all community partners during the research process for balancing power dynamics, fostering sustainable partnerships, promoting actionable health improvements, and reducing disparities through research development (Hacker et al., 2012; Jiménez-Chávez et al., 2018; Wallerstein & Duran, 2006).
CBPR curricula and programs for and between community members and academic researchers have previously been developed to support the integration of community members into research and the development of community-academic partnerships. For example, Canfield et al. (2016) piloted a CBPR curriculum focusing on environmental health research between community-based organizations and academic researchers, whereas Andrews et al. (2013) created a community-academic partnerships (CAP) training initiative for various health projects. Despite efforts to enhance community capacity building in CBPR for community members, to our knowledge, few capacitation programs have incorporated core competencies in health disparities research and are focused on Hispanic populations. Competencies associated to the CBPR approach are based on the nine key principles, which rest in the concept of cultural humility, which include recognizing the community as a unit of identity, facilitating collaborative partnerships in all phases of research, and promoting a co-learning and empowering process that attends to social inequalities. Although no competencies have been developed for community members in health disparities research, a study among professional counselors identified key areas which include knowledge (e.g., understanding key CBPR concepts), skills (e.g., listening, group and facilitating skills), attitudes (e.g., cultural humility, flexibility, persistence), and activities (e.g., community experiences; Dari et al., 2019).
In the United States (USA), racial and ethnic health disparities have persisted for chronic diseases from 2017 to 2019. This period saw a notable 15% increase in chronic diseases compared to 2011 to 2013, affecting 6 out of 10 adults with at least 1 chronic illness and 4 out of 10 with 2 or more. Involving the community proactively in health promotion or disease prevention has proven to be an effective strategy for detecting, understanding, and reducing health disparities (Ahmed & Palermo, 2010; Kilbourne et al., 2006; Minkler & Wallerstein, 2011). Evidence has demonstrated the benefits of active community participation in health research and promotion to address problems related to social and structural inequities that affect health outcomes in under-resourced sectors of the population (Banna & Bersamin, 2018; Harris et al., 2018). CBPR is recognized as a key approach to improving community health outcomes and reducing health inequities (Chanchien Parajón et al., 2021; Oetzel et al., 2018; Sánchez-Johnsen et al., 2015; Tucker et al., 2016, 2019). Engaging community members as co-researchers enhances health equity, research literacy, and community research dissemination (Salimi et al., 2012).
Our Institution features a Specialized Center in Health Disparities (Ponce Research Institute, n.d.) which includes the Community Engagement Core (CEC), a unit within the Research Centers in Minority Institutions (RCMI) that fosters partnerships between academic researchers and local communities to address health disparities. Within this framework, the Community Training Institute for Health Disparities (CTIHD) operates under the RCMI-CEC. The CTIHD’s primary goal is to increase health disparity research and improve community health outcomes in underserved Hispanic populations. This is achieved by fostering CAPs and providing health education to address identified community health needs (Morales-Torres et al., 2023).
To accomplish this goal, the CTIHD developed a program to capacitate and empower community members to address health disparities through research. This article outlines the development, refinement, and implementation of a problem-based curriculum with a competency-based learning model for the first cohort of the CTIHD-Community Research Program (CRP).
Methodology
Background: Pre-Pilot CBPR Workshops
The CTIHD—Community Research Program utilized as a base a series of six one-session CBPR training workshops developed by the research team between 2016 and 2017 for community members. It was facilitated by academics in their respective fields and included topics such as CBPR principles, health disparities, social determinants of health, translational research, ethics in CBPR, and fundamentals of research methodology. These workshops aimed to increase community members’ knowledge and skills to support their integration and collaboration with academic researchers in research activities. Once the workshops were completed, an assessment of acceptability, feasibility, and preliminary effectiveness was conducted through a mixed-method design (e.g., pre-post test, evaluation forms, cognitive debriefing [realized at the end of the workshop series]). Results indicated that the workshops could support the active integration of community members in research activities. Nonetheless, feedback suggested increasing the length for more in-depth exploration of the topics offered and adding practical activities to apply what has been learned. Based on the results obtained from the pre-pilot CBPR workshops, the subsequent phases were conducted to refine and develop the curriculum for the first cohort of the CTIHD-Community Research Program (Jiménez-Chávez et al., 2018).
Phase 1: Literature Review and Additional Resources
An in-depth literature review of peer-reviewed journal articles, website materials, and gray literature centered on community members’ capacitation on CBPR, and research was conducted to support the curriculum refinement process. PubMed, PsycINFO, Social Sciences Full Text, and Google Scholar databases were searched with terms commonly used to identify capacity-building programs for community members in CBPR (e.g., “community capacity building AND CBPR,” “community capacity building AND CBPR AND curriculum,” “community training AND CBPR”) This review aimed to support the research team’s informed decision-making on curriculum design and instructional strategies, identify key areas related to capacity building programs for community members in CBPR and health disparities research, and contextualize the curriculum within the current landscape of similar programs (Allen et al., 2011; Community - Campus Partnerships for Health (CCPH), n.d.; Detroit Community-Academic Urban Research Center, n.d.; Canfield et al., 2016, Highfield et al., 2013; B. A. Israel et al., 2010, n.d.; Leslie et al., 2012; Masuda et al., 2010; Plumb et al., 2019; University of South Florida, n.d.).
During the literature review, the research team (See Phase 2 for description of team members) identified engaging teaching strategies and resources suitable for Puerto Rican/Hispanic community trainees and considered integrating them into the new curriculum to support knowledge retention and engagement. The recommended application activities included small projects, group discussions, presentations, role-playing, brainstorming, literature review, topic conceptualization, library visits, and writing documents to apply learned concepts. For example, sections from the University of Kansas’ “Community Toolbox” were included due to its accessibility in terms of language (Spanish) and detailed guidance, such as “Toolkit #1—Creating and Maintaining Coalitions and Partnerships,” “Toolkit #2—Assessing Community Needs and Resources,” and “Toolkit #10: Advocating for Change” (Community Toolbox, n.d.-a, n.d.-b, n.d.-c).
Phase 2: Curricular Refinement: Syllabi Development, Learning Model, Curricular Design, and Core Competencies
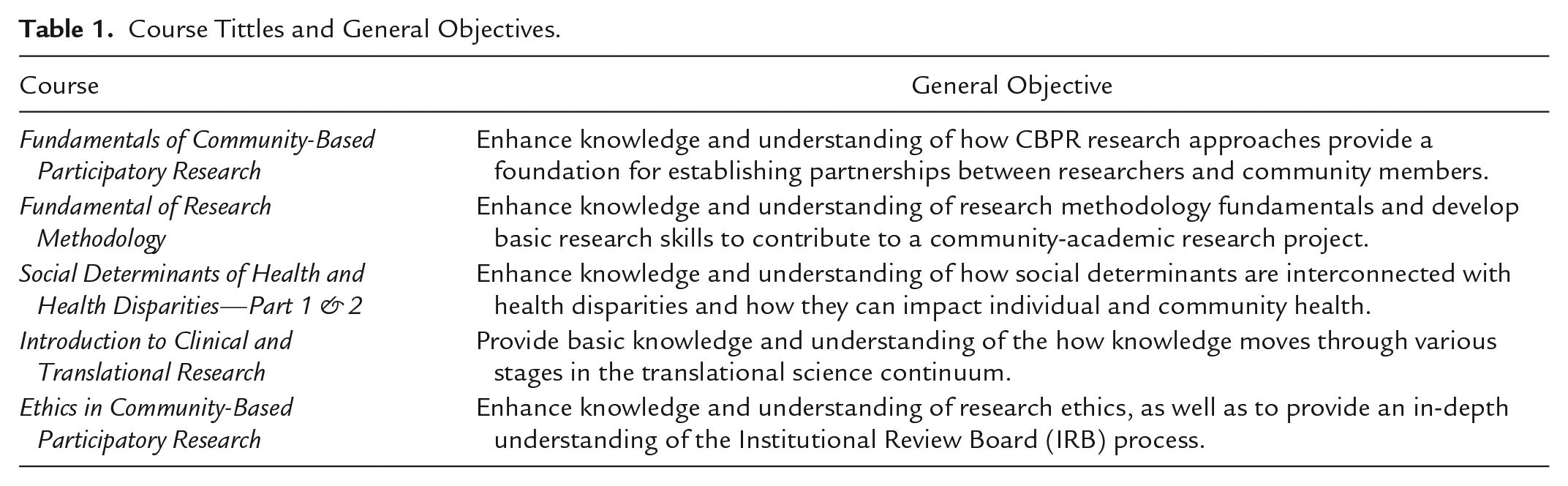
A multidisciplinary research team comprising experts in CBPR, public health, epidemiology, health disparities research, curriculum development, quantitative research methodology design, and clinical and translational research refined the curriculum and developed syllabi over approximately 10 months. The team ensured the curriculum aligned with the objective of the CTIHD-CRP through collaborative and iterative meetings. Through these meetings, based on the pilot program workshop’s initial topics, the research team developed, reviewed, and discussed the course descriptions, course objectives, course content, and activities to be integrated into each 10-session course syllabus based on the literature review and expertise of each team member. The courses aimed to enhance participants’ knowledge and skills in key areas, including CBPR, research ethics, fundamental research principles, social determinants of health, health disparities, and translational research. During these meetings, the course policies, conditions, and evaluation criteria were discussed. See Table 1 for details on the main objectives per course.
Course Tittles and General Objectives.
As no curricular design or learning models were established in the pre-pilot workshops, the research team identified that employing a problem-centered and competency-based learning model rooted in CBPR principles, emphasizing real-world problem-solving, critical thinking, and practical skills development would be fundamental to achieving the objectives of the program (Sistermans, 2020; Universidad EIA, 2020; Universidad Pompeu Fabra, 2013). All pre-pilot CBPR workshop feedback was considered for refining the curriculum and syllabi development, including the length of the courses, and more practical application during courses (See Course Structure and Resources for details).
Aligned with the program’s objectives, “Core Competencies” were identified, selected, and adapted by the research team during the iterative meetings and guided the course content development for the knowledge and skills community trainees were to achieve the expected outcomes and the tools needed to support learning. These core competencies were based on the established Core Competencies for Public Health Professionals by the Public Health Foundation, which provides a foundational framework for public health practice (Public Health Foundation, n.d.). The research team adapted the competencies most relevant to the program’s objectives, design, and learning model, thus developing the syllabi for each course in the new curriculum. A competency matrix was developed to align the specific learning objectives of the courses with the competencies they met. This approach ensured that the program’s content was grounded in recognized public health standards while being tailored to the community trainees’ specific needs in community-based research to codevelop the research proposals in a CAP. The eight competencies identified for the CTIHD-CRP curriculum are analysis/assessment, policy development/program planning, communications skills, cultural competency, community dimensions, public health sciences, financial planning and management skills, and leadership and system thinking (Table 2).
Core Competencies of the CTIHD-Community Research Program.
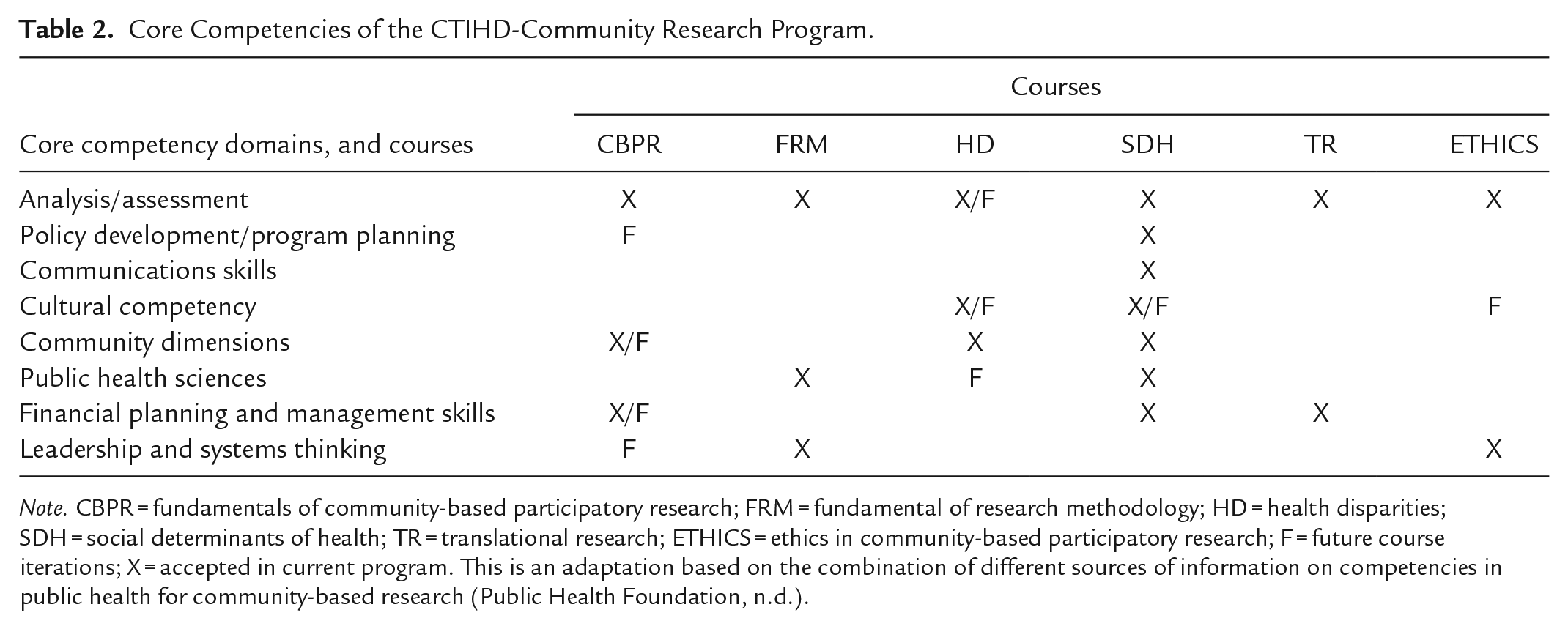
Note. CBPR = fundamentals of community-based participatory research; FRM = fundamental of research methodology; HD = health disparities; SDH = social determinants of health; TR = translational research; ETHICS = ethics in community-based participatory research; F = future course iterations; X = accepted in current program. This is an adaptation based on the combination of different sources of information on competencies in public health for community-based research (Public Health Foundation, n.d.).
Once the initial syllabi were developed, external experts (six instructors with years of experience and with backgrounds in community-level research, such as CBPR and social determinants of health) reviewed, analyzed, and further refined the syllabi to obtain the final versions. This process of expert review helped to validate the alignment of the course objectives, competencies, and content.
Following this, the Community Scientific Advisory Committee (CSAC), composed of eight community representatives trained in basic research principles, evaluated the curriculum. The CSAC’s main role is to assess the comprehensibility of educational or research materials and to confirm that they embody cultural humility and ethical appropriateness for the target audience. The committee reviewed and approved the final version of the curriculum for implementation.
CTIHD: Community Research Program Description
The CTIHD-CRP aims to capacitate community members with the basic knowledge and skills necessary to actively participate as community partners in research projects and support the development of novel research proposals through CAPSs to reduce health disparities relevant to the community. The CTIHD-CRP has eight core competencies based on the basic knowledge and skills identified that community trainees need to participate actively in CAPs and research projects. The program curriculum was organized into six virtual courses (due to the COVID-19 pandemic), with 10 three-hour sessions in a trimester system (two courses per trimester).
Course structure and resources
The structure of the CTIHD-CRP was organized so that the instructors had 3 hr of contact per session with the trainees, with 2 hr of teaching theory, and 1 hr of practical applications of the theoretical content. To guarantee uniformity and comparability between all courses in the curriculum, instructors were provided a course rubric, which included a breakdown of topics with a list of resources, the course objectives, the period duration of the course, the modality, the didactic content, the possible application activities, and a guide on how to develop the evaluation test of the trainee’s knowledge (number of questions, topics, format of questions, considerations). The community trainees were provided with educational materials, syllabi, and references related to the course content. They had access to “Moodle,” a learning management system (LMS) platform for easy access to their course material, which was monitored to ensure everyone had access to it.
The research team identified 48 active learning strategies that instructors could choose from, ranging from 4 to 17 per course, to accommodate different learning styles and support equal opportunities for trainee success. These strategies included art techniques, completing a Know/Wants to know/Learned graph (a tool to keep track of gathered information during the course), role-playing, group discussions, concept maps, and brainstorming.
Phase 3: Recruitment and Selection of First Cohort
Recruitment for the first cohort of the CTIHD—CRP began in April 2020. The research team disseminated information through participation in virtual “open houses”; sharing promotions in community-based and nonprofit organizations with community partners (internal community team members that support project objectives)and through collaborators (external entities that support project objectives); social networks and community educational activities (e.g., health fairs, talks, conferences). Promotional flyers and pamphlets were given to community leaders and strategically placed in the community (e.g., churches, pharmacies, community bulletins). Potential candidates were given orientations of the programs, which included an overall description, programs length, and requirements for completion, among others.
Every prospective community trainee candidate went through the process of completing the application and submitting the required documents: a criminal record certificate, two letters of recommendation, one essay (indicating their motivation to participate in the program), and a resume or curriculum vitae. Additionally, prospective trainees had to be 21 years or older, have completed a high school degree (or equivalent), and be an active member of a community within one of the municipalities located in the southern region of Puerto Rico (as distributed by the health regions of the Department of Health of Puerto Rico). The Selection criteria evaluated during the process were goals or objectives for participating in the programs, experiences working with communities, teamwork experience, and time availability. The Admission Committee, comprised of community partners and the research team, reviewed all documents from prospective trainees. After the documentation review, they were invited for an interview with the Admission Committee. Subsequently, the admissions committee analyzed the results and selected the cohort trainees based on the obtained scores and evaluation criteria (See Evaluation and Instrumentation section for details).
Accepted candidates, notified and confirmed by email, became CTIHD “community trainees,” and started the curriculum in October 2020. Community Trainees were informed that to receive the certification (total of 180 contact hours) granted by our institution and the Research Institute (PRI), they must complete the requirements established by the program: active participation in courses, attending 70% or more of course sessions (no more than three absences), and approve the research proposal with more than a 70% grade.
Participant consent was waived because this study was granted exemption from the IRB review and does not require consent documentation, although all participants received information about the study (IRB protocol #2201083931). No monetary compensation was provided for participating or completing the program.
Phase 4: Implementation of Curricular Sequence and Research Proposal Development
The curricular sequence was organized as follows: (a)
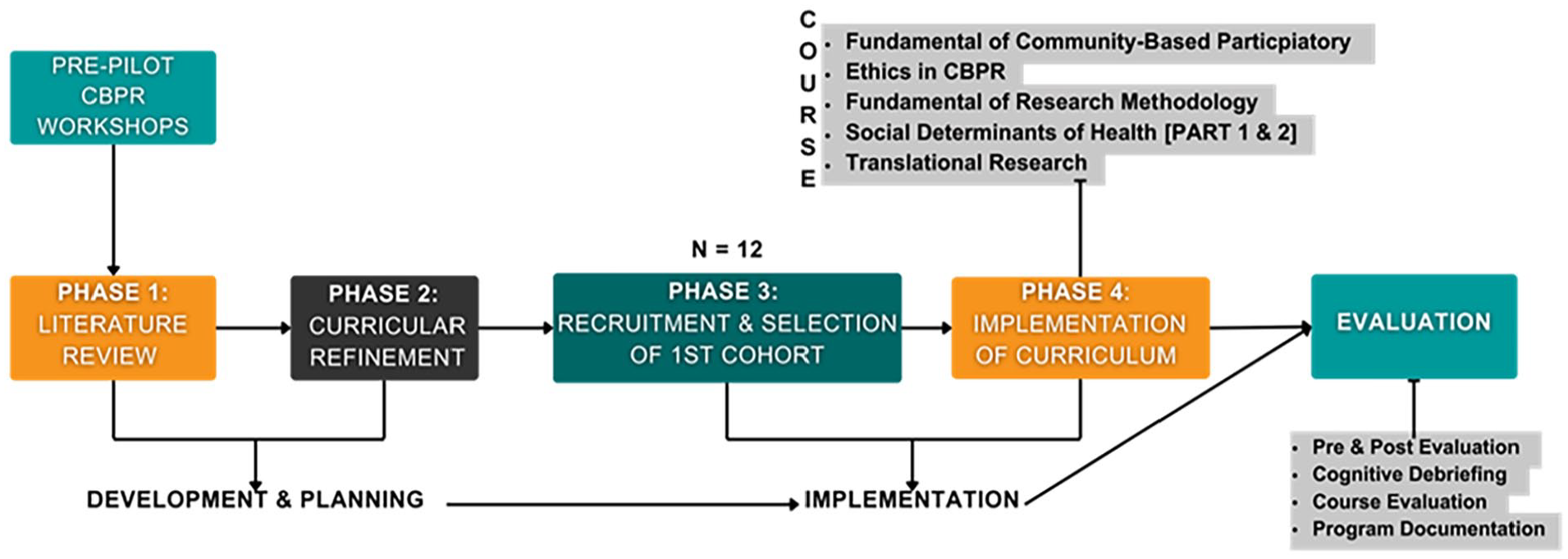
Flowchart of curriculum refinement, implementation, and evaluation.
As a program requirement for completion of the program, a group of community trainees had to co-develop, with an academic researcher, a research proposal on a topic of interest as a final integrative project. It was recommended that trainees consider topics that affect their communities to be applied. The project quick-off meetings began during the third trimester and had a timeline of approximately 6 months to be completed, equivalent to two trimesters. During this period, trainees had an initial meeting with the CTIHD director and academic mentors, during which they were oriented on the research proposal. During the meeting, due dates for the proposal, an outline of the project’s sections, and an assignment for their academic mentor were provided. Academic mentors are experienced researchers in community-based research who provide guidance and feedback on community-academic partnerships during the proposal development process, including reviewing written research proposals, assuring academic standards, supporting literature review, assisting in visual presentation preparations, and applying for funding for the proposal’s implementation.
The project groups comprised two to four community trainees, a collaborating researcher, and an academic mentor. The trainees met, as needed, with their collaborating researchers who are early-, mid-, and senior researchers in their respective fields (e.g., Medicine, Psychology, and Public Health). As professionals with research experience and proposal development, they worked hand in hand with the trainees as research partners. The collaborating researchers were matched with groups based on their expertise, academic experience, and interest in specific health disparities. This matching process occurred through various activities throughout the academic year or during a Community Forum. The Forum, held between the second and third trimesters, serves multiple purposes: project groups present their preliminary research ideas, potential research collaborators engage in one-on-one conversations, and participants discuss preliminary areas of interest. The goal of the Forum is to facilitate the development of Community-Academic Partnerships.
Data Collection and Analysis
Recruitment and Selection Process of Trainees Evaluation
The recruitment and selection process for the programs utilizes a comprehensive rubric method to evaluate candidates through document submission and interviews. The evaluation focused on various criteria, including academic background, work experience, community service, and personal goals.
During the document review phase, the admissions committee assessed submitted materials, assigning 1 point for meeting criteria and 0 points for not meeting them, with a maximum score of 65. The requirements included academics, work experience, community service, letters of recommendation, essays, and a criminal background check. Any criteria not evaluated through documents were addressed during the subsequent interview process.
The interview process employed a rubric divided into three main areas: academics, work experience/community service, and work aspects. These categories were further subdivided into 18 questions to facilitate the interview. Interviewers scored candidates on a scale of 0 to 4 points per question, with a maximum possible score of 133 points. The interviews, lasting up to 60 min, allowed for personalized questions based on the candidates’ submitted documents. If needed, interviewers were encouraged to review the previously submitted materials to create more tailored questions. The final selection of candidates was based on the combined scores and information gathered from the document review and interview process, with a total possible score of 198 points across both stages.
Course and Program Evaluation
During the curriculum’s implementation, the CTIHD-CRP used a mixed methodological approach, utilizing a cognitive debriefing with semi-structured questions (qualitative), a sociodemographic survey, a course evaluation questionnaire, and pre-and post-tests (quantitative). Additionally, data was collected from program documentation.
Quantitative Evaluation (Satisfaction, Acceptability, Knowledge Change)
To assess satisfaction, acceptability, and knowledge change of the curriculum, the following were utilized: course evaluations (satisfaction), retention rate (acceptance), and pre-and post-test (knowledge change). Knowledge change evaluations were administered at the beginning and end of each course. Course instructors developed multiple-choice questions that encompassed the core content, which were then reviewed by the research team to ensure clarity, eliminate ambiguity, and confirm rubric fidelity. Quantitative data was analyzed using SPSSv28 for descriptives and inferential statistics.
Qualitative Evaluation (Acceptability, Feasibility)
Cognitive debriefings are used to actively test representatives of the target population to determine if the respondents understand the material. In this study, the cognitive debriefing session was used to assess the acceptability and feasibility of the curriculum courses to improve the program’s quality. A trained interviewer used semi-structured questions to conduct these at the end of each trimester. A final cognitive debriefing was conducted after completing the program to gather feedback on the overall program.
The virtual session of the final cognitive debriefing lasted 40 to 60 min, depending on the length of the discussion, with approximately 8 to 12 trainees in the session, which were recorded and subsequently transcribed. The questions explored the general opinion of the program, the content and relevance of the courses, the challenges in the teaching-learning process, potential ideas to impact the community, and factors that have been supportive in the process. Two research team members independently reviewed and analyzed the recordings to classify the content. Along with the CTIHD director (principal investigator), they discussed the findings and resolved any conflicting themes.
Results
Overall Research Program Metrics: Applications, Acceptance Rate, Retention Rate, Completion Rate, and Attendance
The CTIHD-CRP’s recruitment efforts yielded 17 applications. After reviewing documentation and conducting interviews, 12 applicants were enrolled, resulting in a 71% acceptance rate. The first cohort completed their coursework from October 2020 to June 2021, excluding the research proposal phase. One trainee initially dropped out of the program (n = 1) for personal reasons), resulting in a 91% retention rate. Of those retained, one obtained incomplete (n = 1) in the research proposal development phase, resulting in an 83.3% completion rate. A high attendance percentage was obtained on the courses, ranging from 87% to 98% (see Table 3).
Overall Research Program Metrics.
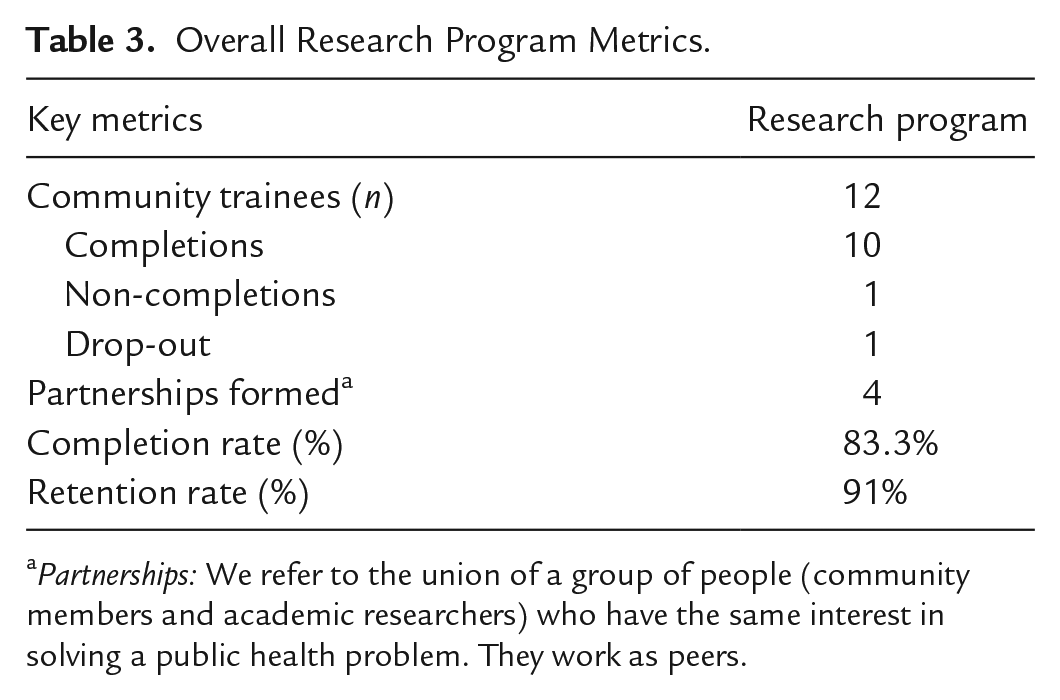
Partnerships: We refer to the union of a group of people (community members and academic researchers) who have the same interest in solving a public health problem. They work as peers.
Quantitative
Community Trainees Sociodemographic Characteristics (n = 10).
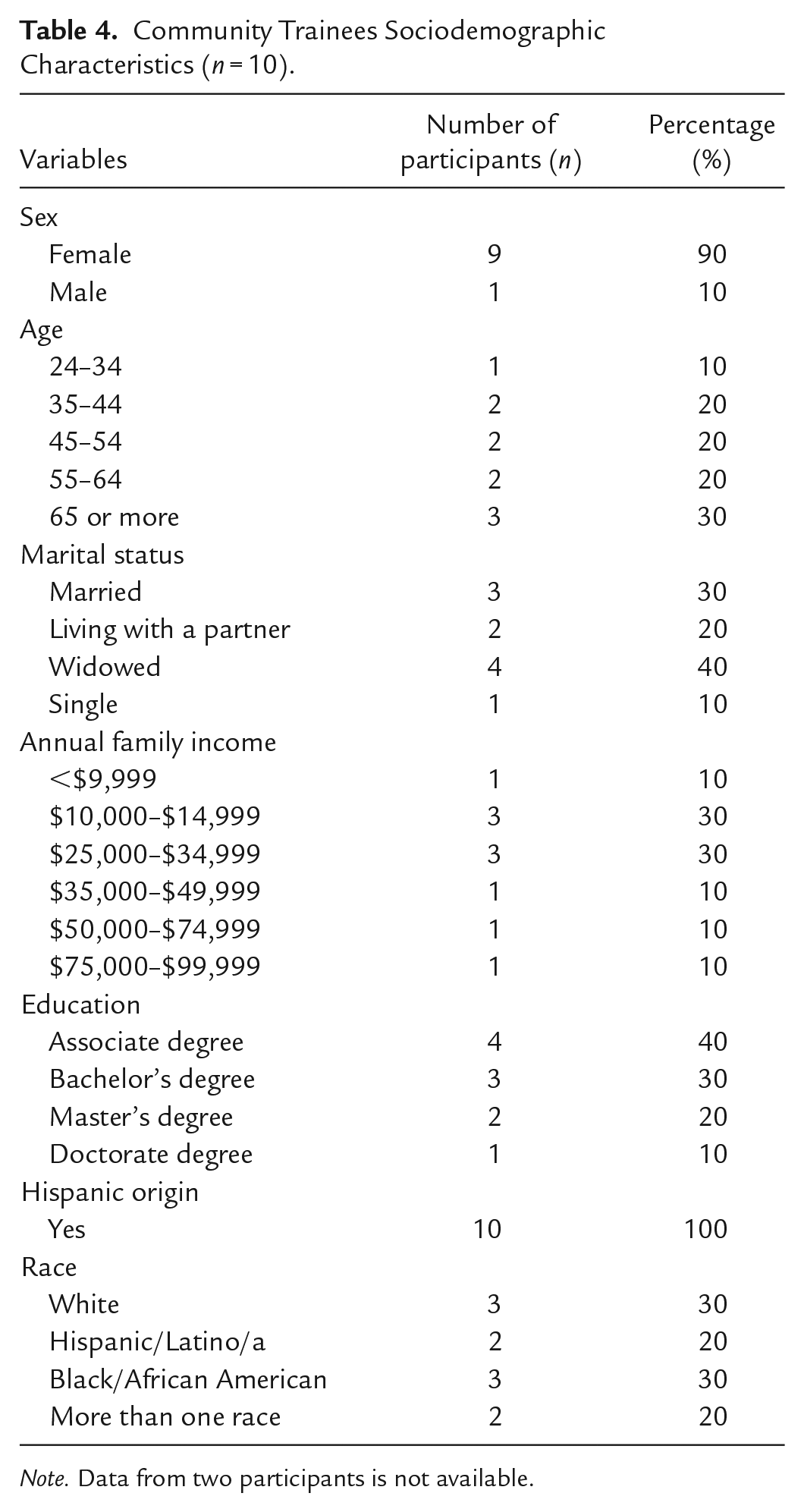
Note. Data from two participants is not available.
In the courses of Ethics in CBPR and Social Determinants of Health & Health Disparities Part 2 (p < 0.05), a statistically significant difference was observed in the change in knowledge. This is also evidenced by the increase in the averages of the pre-test and post-test scores of the Ethics in CBPR course, which increased from 6.8 (pre-test) to 8.7 (post-test). On the other hand, the Social Determinants of Health & Health Disparities Part two course scores increased from 7.7 (pre-test) to 9.8 (post-test).
In general, the average percentage of the post-test score in the curricular sequence was approximately 80% for the six courses, where eight of the 12 trainees completed the curricular sequence with a score greater than 87%.
Three individual judges evaluated these projects. The scores obtained in the proposals ranged from 72.6% to 93.85% (M = 86.60, SD = 2.59). In the individual evaluations, the three groups scored lowest for utilizing eight scientific articles in the proposal. In addition, one of the groups obtained a low score in the selection of subtopics.
Course Evaluations by Domain: Model by Criteria and Courses.
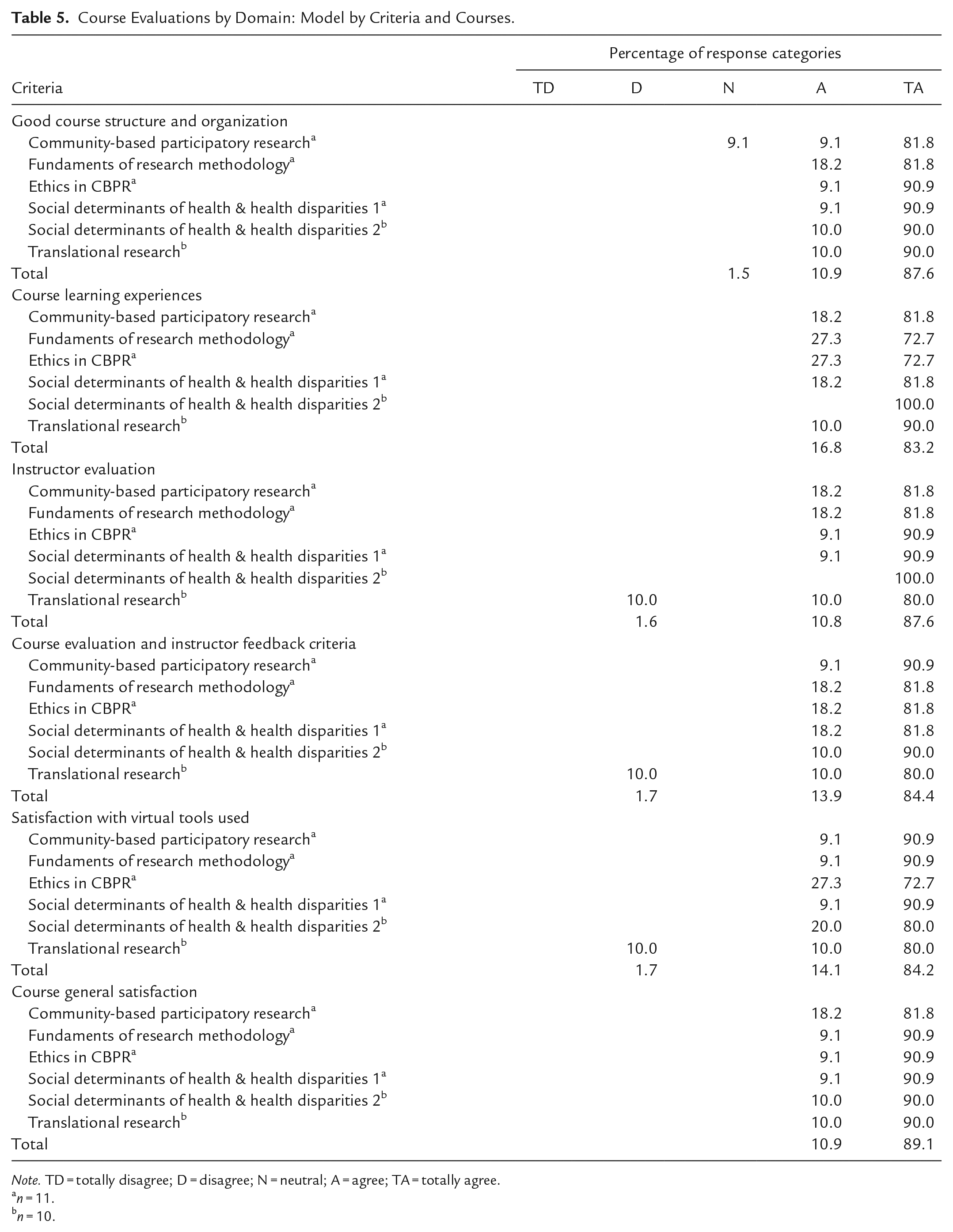
Note. TD = totally disagree; D = disagree; N = neutral; A = agree; TA = totally agree.
n = 11.
n = 10.
Qualitative
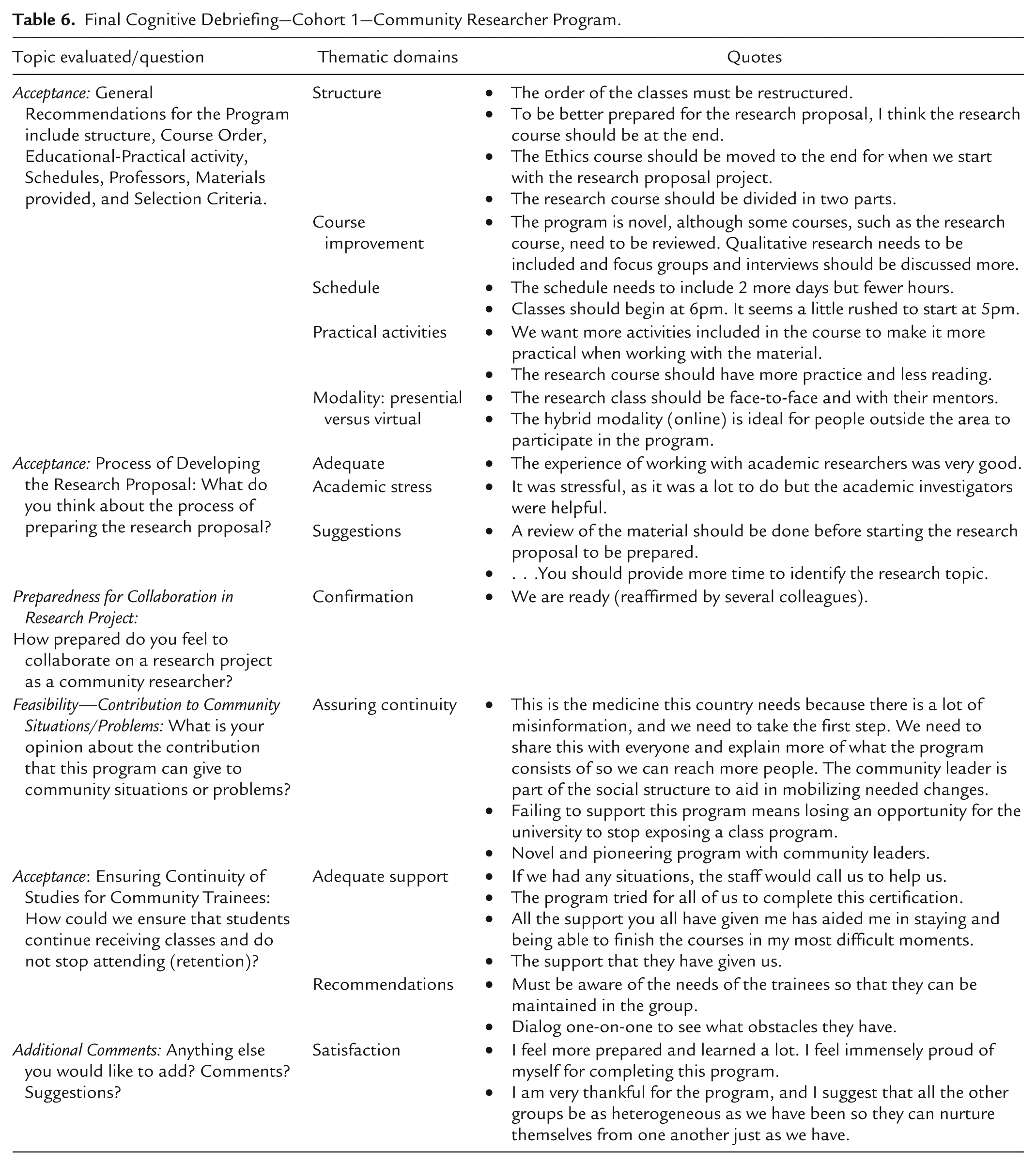
Final Cognitive Debriefing—Cohort 1—Community Researcher Program.
Discussion
Providing community members with knowledge and skills in research is essential for their integration, active participation, and sustainability in research initiatives and community-academic partnerships (Hacker et al., 2012). Through this integration, the relevance of the research to be co-constructed is amplified as it focuses on providing actionable knowledge that could be utilized for decision-making to modify current practices or governing policy to aid in reducing health disparities (Krishnan et al., 2020). The development and refinement of the CTIHD-CRP curriculum and subsequent implementation aim to provide its community trainees with the basic knowledge and skills to achieve this goal.
The results indicate that knowledge change increased for community trainees. The overall average percentage in the post-test scores was approximately 80% for all courses, suggesting a general understanding of the presented materials. Two courses demonstrated statistically significant change (p < 0.05) in scores: Ethics in CBPR and Social Determinants of Health & Health Disparities Part 2. Although most courses had increased knowledge, the Fundamental of Research Methodology course obtained the lowest score, demonstrating a need for further refinement and review. During the cognitive debriefing sessions, one participant expressed: “The research course should have more practice and less reading.” These indicators are essential to modify the course to aid better comprehensibility and ensure alignment with the needs of our trainees and future cohorts. Although difficulties in this course were identified, the course itself or lack of knowledge was not mentioned as a barrier for trainees to develop their research proposals with academic researchers co-jointly. A high retention rate (91%), the course overall satisfaction (89.1%), and the trainees’ expressions during the cognitive debriefing, such as “I feel more prepared, and I learned a lot” and “I feel immensely proud of myself for completing this program,” supports our inference of trainees’ satisfaction and acceptability of the program.
For the academic programmatic structure, the trainees offered recommendations and contributions that are fundamental for the changes to be made in the general structure of the curriculum, including the order in which the courses will be taught, the balance between theoretical and practical activities, the schedule of the program, and materials provided. It is supported by what was expressed by one of the trainees: “A review of the material must be done before starting the research proposal to be prepared.” All these recommendations will be reviewed and analyzed before implementing the next cohort of trainees, combining them with a more in-person experience with the instructors and more practical activities for better comprehension of the teaching materials and information provided, particularly in courses that presented lower knowledge change.
According to the cognitive debriefing results from the research project development process, trainees felt ready to collaborate on research projects to benefit their communities. One trainee said, “The experience of working with academic researchers was very good.” The program’s initial outcomes include forming CAPs between community trainees and collaborating researchers, as well as and the successful co-development of three research proposals adressing current community health needs. Nonetheless, some participants expressed that the experience was stressful and suggested that there should be a review of the course content before starting this process.
The cognitive debriefing results imply that community trainees found the program acceptable and feasible. One community trainee stated, “This is the medicine this country needs because there is lots of misinformation, and we need to take the first step. We need to share this with everyone and explain more of what the program consists of so we can bring more people.” Another said, “Failing to support this program means losing an opportunity where the university could stop exposing a class program.”
The geographic location of this program, Puerto Rico, suffered the consequences of the great earthquakes that occurred in January 2020 (Almond, n.d.; Central Office of Recovery, Reconstruction and Resilience [COR3], 2023). Low literacy levels and limited access to technology among some trainees were identified as potential barriers to academic engagement. These factors created disparities in participation compared to other trainees. The research team offered basic training on the technologies required and provided computer equipment to address this issue. The situation was further complicated by trainees living in rural and remote areas, where weak and unstable internet signals caused interruptions in course transmissions and trainee participation. As a solution, courses were recorded to allow trainees to watch them later if needed, and with follow-up from the instructors to ensure comprehensibility of the material.
Limitations for this study include (1) non-generalizability of results due to the non-probabilistic sampling method (purposive sampling); (2) the original programmatic structure was devised to be implemented in an in-person modality (notwithstanding modifications were realized to support a virtual environment); (3) trainees barriers in literacy and access to technology or internet; (4) participant burn-out from COVID-19 pandemic might have impacted trainees comprehensibility of material due to reduced engagement in courses (notwithstanding a counselor was provided and courses were recorded). Some of these limitations could have skewed the trainees’ change in knowledge by influencing their ability to participate fully in the courses.
The strengths of this study include the development and implementation of the program at our institution, an academic institution focused on health sciences education, which proved advantageous. Our institution diverse academic offerings, including public health, clinical psychology, biomedical sciences, and medicine, facilitated the development of partnerships between academic researchers and community trainees. This multidisciplinary environment enhanced the program’s effectiveness and provided a rich context for community-based participatory research education.
Future directions for the CTIHD-CRP program involve several primary goals. First, we aim to enhance the current curriculum by incorporating feedback to benefit future cohorts. Additionally, we plan to evaluate the program’s impact on trainees’ ability to apply their skills within their community work and their confidence in conducting CBPR and research activities. Further assessment of future community-academic partnerships will provide insights into group dynamics and opportunities to strengthen collaborative practices. We also intend to identify supportive mechanisms for existing partnerships, focusing on implementing co-developed research proposals that address health disparities and promote health equity. Through these efforts, we strive to continually increase the program’s effectiveness in advancing community-based research and improving health outcomes.
Conclusion
Strengthening community capacity is essential for effectively integrating communities into health research activities, improving health outcomes, and ensuring the long-term sustainability of health initiatives. The CRP, developed by the CTIHD aims to empower community members with essential knowledge and skills to support the development of equitable partnerships and increase research on health disparities. The community trainees found the refined curriculum acceptable and feasible, demonstrating increased knowledge despite suggested modifications. The program’s outcomes include forming partnerships and co-developing three research proposals on community-identified needs.
Through this research capacity-building curriculum, the CTIHD aims to increase community participation in health research, foster the formation of CAPs, and support the development of research on health disparities. Additionally, the knowledge obtained through the development of these community-led research projects can evidence community health needs, which guides health promotion efforts to be tailored to specific community contexts and needs. This progress represents a positive step toward reducing health disparities and building healthier, more empowered communities in southern Puerto Rico. Ultimately, the long-term impacts of these efforts are aimed at improving health equity and reducing health disparities for and with the community. We anticipate that acknowledging the significance of community empowerment will guide others in developing research capacity-building programs to enhance community partner engagement. This approach will ensure that social determinants become fundamental in shaping future research initiatives, ultimately advancing community health equity through active participation and leadership within the community.
Footnotes
Acknowledgements
We would like to acknowledge the effort and support that our community partners in the Community Trained Workforce (Annette Velazquez, Ivette Gracía, Lydia Vazquez, María Arzola, Roberto Ortiz, Zuleyma Rivera) and Community Scientific Advisory Committee (Ada Colón, Ada Rodríguez, Carmen Vélez, Elidia Rodríguez, Geraline García, Juan Pablo Rivera, Marelyn Gonzalez and Harold Martínez) provided this project to conduct these capacitation programs for our community. We would like to acknowledge Nina Wallerstein for her continued mentorship and support for this project. We would also like to acknowledge Lydia Santiago for being a source of inspiration and influence with her community-focused work.
Data Availability Statement
The data available on request due to restriction for example, privacy, or ethical. The data presented in this study are available on request from the corresponding author. The data are not publicly available due to confidential information that could identify participants; therefore, we must verify that any data shared does not have any quotes that could identify participants.
Declaration of Conflicting Interests
The authors declare no conflict of interest. The content is solely the authors’ responsibility and does not necessarily represent the official views of the National Institutes of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research Centers for Minority Institutions (RCMI-2U54MD007579).
Ethical Statement
The study was conducted according to the guidelines and approved by the Institutional Review Board of Ponce Health Science University protocol number: 5U54MD007579 approval date 14 July 2021.
Geolocation
The data were collected in the South of Puerto Rico.
Permission to Reproduce Material
All materials in this draft is original work from authors.