
Abstract
Amid the racial unrest stemming from the summer of 2020, in the United States, many institutions had difficult conversations about race and the impact of racism with employees, students, and patients. In January 2021 and February 2021, we recruited undergraduate students for the Peer Education Program (PEP), a voluntary program conducted at a large academic medical center, and encouraged students to have a safe space to discuss controversial topics in healthcare. From April 2021 to July 2021 four interdisciplinary healthcare students met once a month for 1 hr to discuss privilege, race/racism, leadership, and advocacy and their influence on health equity. Four students completed PEP, and three students completed the program evaluation survey. Conventional content analysis was used to code data and identify major themes to evaluate PEP. Students described privilege in a positive context, using words like “freedom,” “special right/advantage,” and “opportunity.” Race was viewed as (1) a way to discriminate, (2) a “man-made concept” used to establish racial hierarchy, and (3) insignificant due to the complexity of human beings. Students realized there are several required steps to adopt and sustain social change in healthcare, which led to the “The Four A’s of Social Change”: Awareness, Acknowledgment, Action, and Advocacy. Program strengths included topics, guest speakers, and open dialogue. Recommended changes included allocating more time for dialogue and increasing the frequency of monthly meetings. To be an influential and empathetic leader in healthcare, one must understand the impact that privilege and race/racism have on patients and equitable healthcare.
Introduction
The United States (US) has a well-documented history of medical racism and identity-based discrimination within its healthcare system (Muntinga et al., 2016). Consistent with the racialized treatment individuals experience within other social institutions—education, government, and the economy—patients of color are often the victims of exclusionary and discriminatory policies and practices, which can have deleterious effects on their lives and well-being (Evans et al., 2020). As a result, health inequities are not the result of an inherent predisposition for poor health but are the result of oppressive, institutionalized, and codified practices that result in the differential treatment of racial and ethnic minorities. This dynamic is further compounded by implicit bias, prejudice, and the racialized attitudes seen in American society (Hall et al., 2015). More specifically, implicit racial bias has been linked to healthcare providers’ preference for White patients and has been attributed to poor ratings of interpersonal care in interactions with patients of color (Cooper et al., 2012).
Learning about health inequities, implicit bias, and the social transgressions that cause them has been a growing part of curricula at many academic health centers (Blue & Fleming, 2009; Dogra et al., 2009; O’Reilly, 2020). Healthcare programs across the country have increased conversations about medical racism and have looked for ways to explore the nexus between racism, health equity, and social justice in didactic education and clinical training. With a call for healthcare providers, administrators, and biomedical scientists to be more socially responsible and culturally conscious, healthcare educators have searched for effective ways to enhance students’ learning about implicit bias, structural oppression, and social justice (Dogra et al., 2009; Nagda et al., 1999). Even further, during COVID-19, there were those who described similarities between racism and the global pandemic (Brown, 2020; e.g., redlining and social distance, respectively) or even the twin pandemics or “dual pandemics” where both race/racism and COVID-19 have negative (and more pronounced) impacts on communities of color (Jones, 2021).
Approaches to Cultural Education
Healthcare and social science educators have used various methods and theoretical approaches to teach students about diversity, institutionalized racism, and cultural consciousness. Many have championed a cultural competency paradigm where individuals strive for mastery within defined content areas, but now, scholar-practitioners recommend using a cultural humility framework where learning is a life-long commitment to self-reflection and self-critique (Lekas et al., 2020; Tervalon & Murray-García, 1998). Furthermore, cultural humility calls for providers and researchers to work collaboratively with marginalized and minoritized communities to fix power imbalances and eradicate policies and practices that lead to health inequities (Tervalon & Murray-García, 1998). Educational approaches rooted in a humility framework are dynamic, and change as attitudes, behaviors, and cultures shift; these approaches merge the continuous need for new knowledge and cultural understanding with the constant expectation for self-reflection and personal development. This fluid, self-evaluative method allows healthcare educators to best prepare their students to meet the current and future needs of an ever-evolving healthcare landscape (Lekas et al., 2020).
One pedagogical approach—intergroup dialogue centered on reflective learning—calls for educators to emphasize students’ cognitive ability in understanding complex diversity, equity, and inclusion topics while also paying attention to their emotional development (Dogra et al., 2016; Nagda et al., 1999; Nakanishi & Rittner, 1992; Van Soest, 1994). By employing didactic methods such as defining terms (i.e., bias, racism, prejudice, privilege, oppression) and incorporating experiential learning approaches like case studies and short vignettes, students are provided opportunities to examine their intellectual knowledge and personal attitudes toward course content (Dogra et al., 2009, 2016; Latting, 1990). One of the many goals is to provide dialogue focused on awareness, empathy, and respect especially when discussing potentially controversial topics.
Background
The Peer Education Program (PEP), which is a pilot study, is based on educational research conducted within a Social Determinants of Health (SDOH) course offered at a large academic medical center. During the 300-level SDOH course, students learned about several SDOH (e.g., race and racism, socioeconomic status, policy, etc.) and their impact on health outcomes and health disparities. Weekly topics included privilege as a SDOH, socioeconomic status, disability, cultural awareness, race/ethnicity, immigration status, and healthcare access. Additional information about SDOH course assignments and details are described in a prior paper (Brown et al., 2021). In the fall 2020 SDOH course, students completed several assignments, including a Modified Privilege Walk (MPW) to learn about privilege as a SDOH (Witten & Maskarinec, 2015), SDOH photography essay (Brown et al., 2023), and case study (Cantey et al., 2017) rooted in aspects of SDOH and cultural awareness (Brown et al., 2021). The SDOH photography essay gave students a chance to identify and describe SDOH in their local communities (Brown et al., 2023). The case study assignment required students to develop a scenario where a patient is seeking healthcare services. Students incorporated various SDOH and aspects of cultural awareness in their case study. The latter assignment provided an opportunity for students to distinguish between SDOH and cultural awareness. During the SDOH course, when completing the MPW, students answered questions about race and social class. Based on their responses, students received a “privilege score,” which was used to increase awareness about privilege or lack thereof. Details about how students’ “privilege scores” were calculated were published in a previous paper (Brown & White, 2020). During PEP, we paired a higher-scoring student with a lower-scoring student using percentiles. For example, the mean privilege score for the fall 2020 cohort was 13.53, with the lowest at −14 and the highest at 30. Students who participated in PEP during the spring and summer of 2021 completed the fall 2020 SDOH course where they completed these assignments and discussed how they could be more aware and empathetic to individuals from underprivileged communities. PEP is an ideal continuation of the SDOH course where students learn to have difficult conversations, learn from various human experiences, and have a chance to recognize their own biases and stereotypes that may hinder patients’ experiences in the healthcare system.
The purpose of this paper is to describe the development, implementation, and evaluation of a pilot study (PEP), which was an exploratory, voluntary program that facilitated peer learning and small group discussions on race/racism, privilege, leadership, and social justice advocacy. Using qualitative methodology, we specifically address the following research question: How do undergraduate allied health students, participating in the Peer Education Program, describe their perceptions of race, privilege, leadership, and advocacy?
Methods
Procedure
The first author [EAB] applied for internal grant funding from the Medical University of South Carolina’s Office of Humanities to develop, implement, and evaluate PEP. Two members of the research team [EAB & DP] developed an application that included an informed consent statement, program description, demographic questions, and compensation details. We entered the application in REDCap (Research Electronic Data Capture). From January 2021 to February 2021, the student service coordinator for the undergraduate program emailed 17 eligible undergraduate students (those who took the fall 2020 SDOH course) about PEP (and link to application) to recruit for the program. Additionally, one instructor posted several announcements during the same period.
When completing the application, students checked whether they wanted to voluntarily participate in PEP or not. If a student chose not to participate, the application automatically closed. In the informed consent statement, students acknowledged they would be paired with students based on their privilege walk scores from the SDOH course (partner student with a lower score with a student with a higher score) (Brown & White, 2020). Applicants provided the following demographic information: age, sex, race, and ethnicity. Applicants read program requirements (e.g., attend required meetings and read required material) and compensation details and respond if they understood that compensation was based on their participation and completion of the program evaluation survey at the conclusion of PEP. Students could earn up to $250, via check, from the university for their participation after the program concluded. Applicants were asked to check all the weekdays they could meet in the evening for 1 hr so the research team could identify the best day of the week and time to meet for the larger group meetings, which included all participants, facilitator, and guest speaker(s). Due to small sample size, we do not report participants’ demographic information.
Participants
PEP participants consisted of four interdisciplinary undergraduate, allied healthcare students at a large academic medical center in the southeastern US. All students were allied health professionals, separate from medicine and nursing (e.g., certified nursing assistants, emergency medical technicians, dental hygienists, occupational therapists, etc.). The four PEP participants were a subset of 17 undergraduate students in an undergraduate healthcare program. This study is exploratory in nature due to the small sample size.
Program Description
PEP lasted from April 2021 to July 2021 with four monthly required sessions with the larger group (all participants, facilitator, and guest speaker). Students met twice a month. The first meeting was 1:1 with their “matched” peer discussing required material and questions. The second meeting at the end of the month was held via Zoom with the larger group, which included all students, the first author [EAB], and guest speakers who served as content experts. All PEP documents were housed in a non-credit bearing course shell in D2L/Brightspace, which is an online learning platform. PEP leadership provided the following mental health resources to each student: university counseling services, state department of mental health, National Suicide Prevention Lifeline, Substance Abuse and Mental Health Services Administration (SAMHSA) National Helpline, and Crisis Text Line. Students were also encouraged to reach out to PEP leadership, Division Director, or the Associate Dean for Student Affairs for assistance if needed.
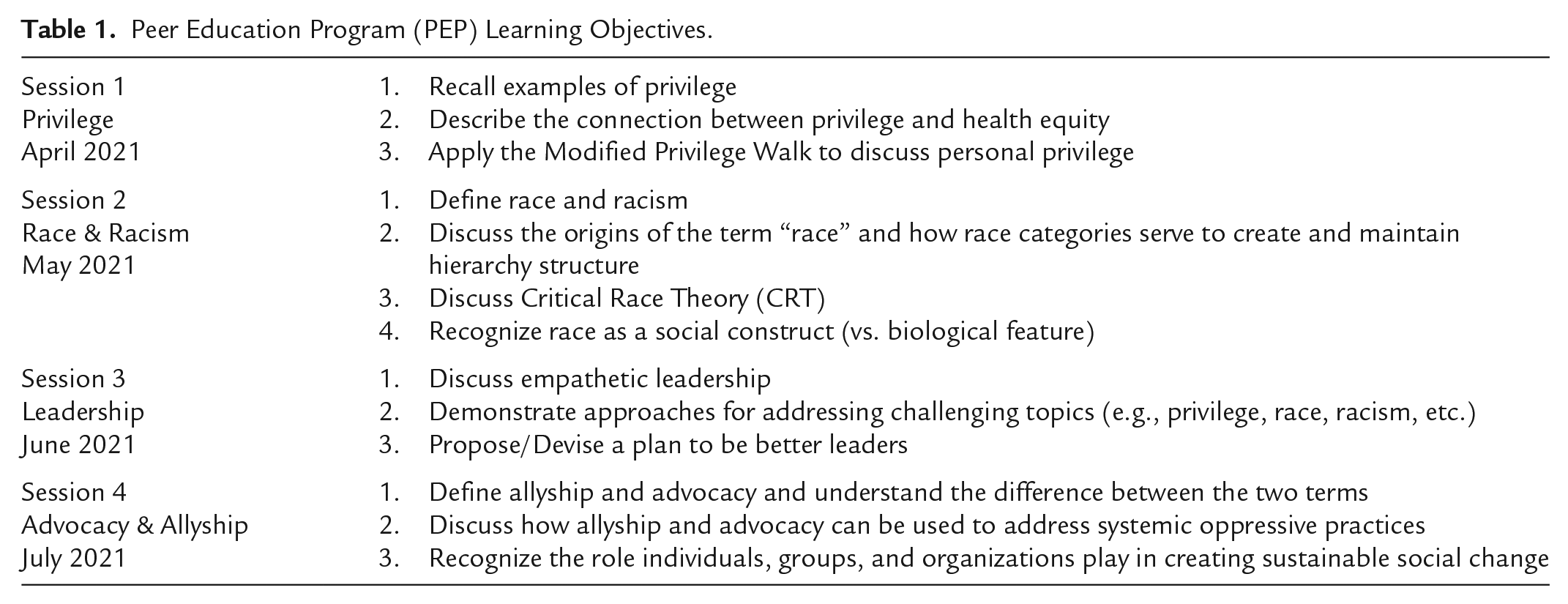
From April 2021 to July 2021 students had four sessions that covered several topics, including privilege as a SDOH, race and racism, leadership and advocacy (Table 1). Learning objectives based on Bloom’s Taxonomy were provided to students to provide structure, promote clarity, and guide student learning. Each topic had at least three learning objectives, required reading material, discussion questions, and supplemental reading material. For example, when learning about privilege, students discussed various types of privilege other than “White privilege” and if privilege could impact health equity or health outcomes (Romano, 2018). When discussing race and racism, students learned about critical race theory and discussed the origins of race in American society. Students also discussed how one researcher conceptualized the similarities between racism and COVID-19 (Brown, 2020). Hearing a story from a racially minoritized individual about their struggles regarding something as simple as the color of their skin gave students a chance to describe and discuss their feelings about racism and its effects. For leadership, students tackled more issues related to self by identifying ways they could be an empathic leader in their academic program, professional career, and personal life. Students learned about potential weaknesses in leadership and the harm to health equity and community trust (Clancy, 2015). In the last session, students learned the different approaches to allyship: ally for self-interest, ally for altruism, and ally for social justice (Edwards, 2006). Students were challenged to reflect about where they stand on the allyship spectrum.
Peer Education Program (PEP) Learning Objectives.
Data Collection
Students had the first 2 weeks of August 2021 to complete the evaluation survey. The survey asked students open-ended questions about their perception of each monthly topic since participating in the program. The following additional questions were asked of each student: (1) How is privilege connected to health equity? (2) How can leaders address challenging topics concerning racism? (3) How can individuals advocate for causes they think are important? Students were also asked to describe program strengths and weaknesses. Students were required to upload an Advocacy Pledge at the end of the evaluation survey. The Advocacy Pledge was a short (e.g., one paragraph) statement each student created to demonstrate how they planned to lead discussions surrounding various PEP topics in the future and continuously advocate for different causes and communities.
Data Analysis
One member of the research team downloaded the survey data, deidentified the data, and shared deidentified data with five coders. The students’ instructor only had access to deidentified data. The team agreed to individually code survey responses line by line to assign initial codes to meaningful units used to describe participant experiences. The team met over 3 months discussing codes, definitions, and examples (data sources), which allowed time to continuously ask questions, review codes, and establish consensus. Codes were condensed and grouped into categories by similarity or common issue. Categories were then examined for patterns and themes. One research team member kept detailed notes concerning changes in coding, categories, and areas of negotiated coder consensus using a team-based approach to open coding (Cascio et al., 2019). PEP students were asked to provide feedback regarding the findings, which is known as member checking (Tong et al., 2007). The research team developed a codebook capturing data brainstorming, initial and final codes, examples (data source), and themes or findings.
Qualitative methods focused on collecting and analyzing data to explore subjects’ experiences in various social or physical communities (Tong et al., 2007). The team used a 32-item checklist of best practices or recommendations to report qualitative research describing PEP evaluation (Tong et al., 2007). PEP students’ responses were analyzed using an inductive approach, where the analysis was data driven and not particularly focused on a framework or theory. The inductive approach allowed the research team to focus purely on students’ responses to gather new knowledge.
The research team used conventional qualitative content analysis, which is an ideal approach in describing a phenomenon when limited research literature or theories are available (Erlingsson & Brysiewicz, 2017; Hsieh & Shannon, 2005). The conventional content analysis approach begins with observation of an issue and uses text or qualitative data to form categories, leading to themes (Hsieh & Shannon, 2005). Content analysis allows for systematic and open coding to explore data and find patterns within the text (Vaismoradi et al., 2013). One of the advantages of conventional content analysis is researchers are not required to have specific categories to impose on study participants, allowing the team flexibility to describe students’ experiences as they completed PEP (Hsieh & Shannon, 2005).
Ethics Review
The Medical University of South Carolina Institutional Review Board reviewed the study and deemed the project to be analogous to quality improvement/program evaluation.
Results
All four students completed PEP and its associated monthly meetings; three of the four students completed the program evaluation survey resulting in a 75% response rate. Students perceived privilege positively, describing it as “freedom,” “special right/advantage,” and “opportunity.” Race was viewed as (1) a way to discriminate, (2) a “man-made concept” used to establish racial hierarchy, and (3) insignificant due to the complexity of human beings. Three salient themes emerged from the data analysis which summarized students’ perception of race, privilege, and inequities. Direct quotes from the anonymous program evaluation survey contributed to the emerging themes.
Theme #1: “Conceptualizing Race, Privilege, and Inequities as Products of Social Constructionism”
Participants’ data surrounding race and privilege combined to form the theme of “Conceptualizing Race, Privilege, and Inequities as Products of Social Constructionism,” which means examining how people understand the world around them through social interaction. Researchers noted that individuals may be blind to various types of privilege; however, acknowledging privilege can be used to help others. Students explained privilege as “a special right/advantage that is granted or given and cannot be worked for or obtained over time.” Based on the data, race served as an “identity,” but also a “man-made” construct. However, race could be viewed as insignificant due to the various complexities of human beings and should not be the sole predictor of outcomes. Students stated, “[. . .] race is defined by society and categorized based on similar physical and/or social attributes,” and “this man-made concept [refers] to placing [people] into a racial hierarchy based on their color, socio-economic status (SES), etc. The racial hierarchy serves to keep social injustices and inequities in place.”
Theme #2: “Leading From an Advocacy Lens”
Participants described how effective leadership blends aspects of advocacy and allyship with the principles of empathetic leadership, which led to the theme “Leading from an Advocacy Lens.” Students perceived ideal leaders as empathetic and impartial, stating that leaders should be honest and acknowledge “no tolerance” for racism when discussing challenging topics like race/racism and privilege. One student stated, “a good leader is empathetic . . . able to understand where their team members are coming from and how best to support them.” Participants deemed that advocacy meant engaging and speaking, and particularly, supporting others while collaborating with various stakeholders, including local communities, government, and lawmakers. Participants concluded that advocacy requires awareness, continuous education, and community engagement.
Theme #3: “Developing Leadership Capacity Through the Impact of Uninhibited Peer Learning on Personal Growth With Open Dialogue”
Within this theme, students also emphasized the importance of open-mindedness, having space to share perspectives honestly, and how these experiences can lead to increased leadership capacity. Students viewed having open dialogue in a safe space with diverse peers as a PEP strength. PEP completion equips participants with evidence, resources, and practice discussing challenging topics like privilege and race/racism. This practice may make students more adept to discuss these challenging topics and better advocate for minoritized patients and their communities. One student concluded that: [the] experience throughout the Peer Education Program was definitely eye opening. Hearing how everyone has experienced each topic through stories of their childhood or life experiences has really helped me in understanding that there are people going through similar situations as me and then there are people that have grown up way differently than me, but we have all wound up on the same path.
Other students stated “I loved hearing about other people’s perspectives on each topic. It was a great way for everyone to learn and grow,” and “I had a very liberating experience participating in the Peer Education Program. I have never been able to openly share my experiences prior to being in this program.”
The Four A’s of Social Change
The research team perceived that there is a want for social justice but a dire need for social change. With this perception, both concepts are needed to promote sustainability. There are several required steps to adopt and sustain social change in healthcare. During the final round of group analysis, faculty researchers and students devised “The Four A’s of Social Change” (Figure 1).
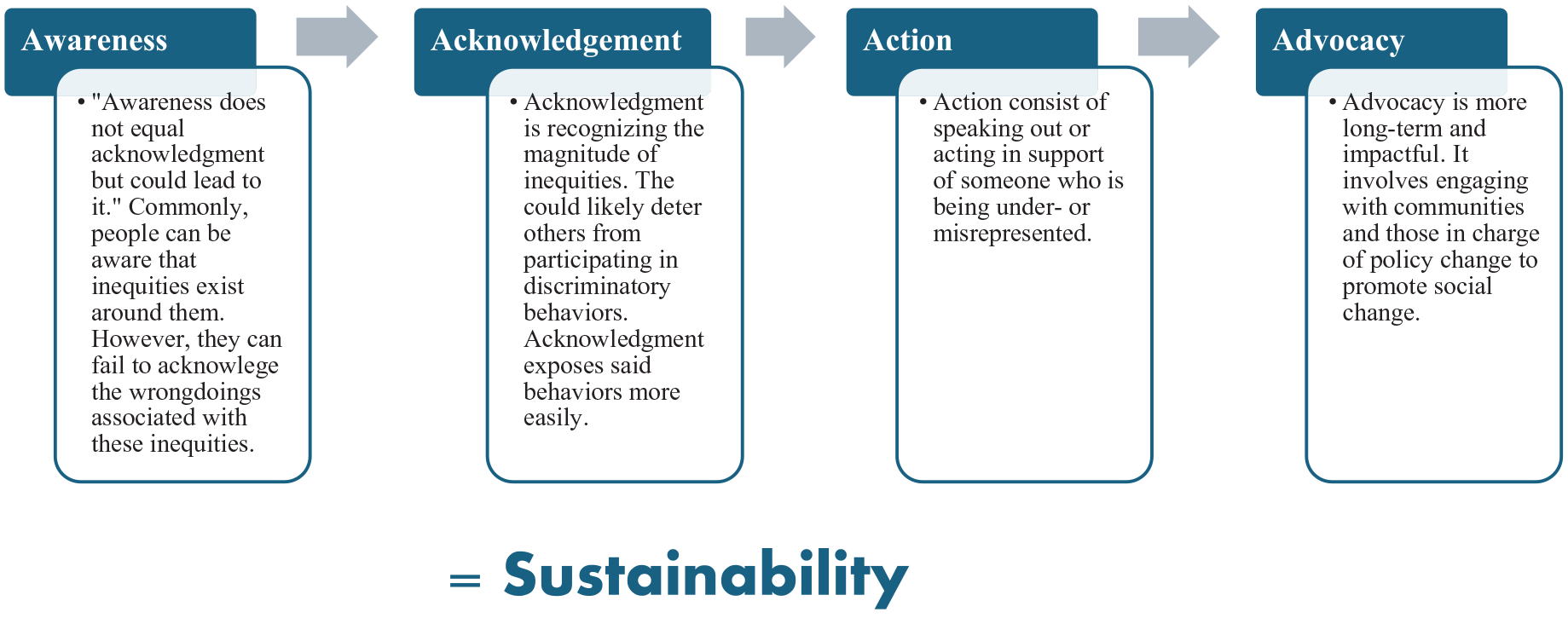
Four A’s of social change.
The research team determined that “awareness does not equal acknowledgment but could lead to it.” Students felt that people are often aware of inequities around them but fail to acknowledge the wrongdoings associated with the inequities. Acknowledgment is recognizing the magnitude of an inequity. Acknowledgment exposes discriminatory behaviors and could deter others from engaging in said behaviors. Researchers concluded that action consists of speaking out or acting in support of someone who is being under- or misrepresented. Advocacy was seen as a more long-term and impactful component. Researchers concluded that advocacy involves continuously engaging with communities and those in charge of policy change to promote social change. Combined, Awareness, Acknowledgment, Action, and Advocacy—or the Four A’s—promote sustainability where we may begin to see positive social change.
Program Recommendations
PEP students offered three recommendations to enhance the learning experience and impact of the program for future participants: (1) increase the meeting time from 1 hr to one and a half hour or 2 hr, (2) increase the number of meetings each month, and (3) invite more guest speakers. Another recommendation was to increase the number of monthly meetings to two meetings per month where the first meeting would mirror the monthly sessions facilitated during PEP (didactic learning) and the second meeting of the month would be more reflective to allow students the time and space to discuss their lived experiences where they could delve deeper into conversations and strategies.
Discussion
There is a need for healthcare students to reflect upon and discuss issues related to diversity, equity, and belonging in relation to leadership and allyship if we are to create safe spaces for students as well as patients in the healthcare setting. Students learned effective leadership can emerge from the uninhibited conversations surrounding race and privilege. While there was a small sample size for the pilot study, evaluation data was overwhelmingly positive and provided examples on how to improve PEP for future cohorts. Several themes emerged related to the construct of race and being able to lead from an advocacy lens. Further, effective leadership can come from the uninhibited conversations surrounding race and privilege.
Peer learning and education has proven to be an effective tool to teach healthcare students about diversity and social justice (Gaertner et al., 1993; Nagda et al., 1999; Zúñiga et al., 2007). When using peer learning techniques such as intergroup dialogues, “students are offered a safe environment to explore diversity and social justice issues through participation in experiential activities, individual and small group reflections, and dialogues” (Nagda et al., 1999, p. 437). In these small group educational settings, students can explore their own social identities and develop an understanding of how social identities and social group memberships in society can impact healthcare team interactions and patient-provider relationships. According to authors, deeper conversations about addressing systemic healthcare inequities and discrimination can also take place in these settings (Zúñiga et al., 2007). As the use of peer education and small group learning become more prevalent in healthcare discussions on diversity, researchers and educators can benefit from understanding students’ attitudes and experiences with these approaches.
It is important to note that the approach in which PEP leadership designed and implemented PEP may have served as an influential characteristic for students’ positive experiences. Pairing students together based on their privilege walk score from the fall 2020 SDOH course allowed us to pair students on different ends of the privilege spectrum and hopefully led to robust and respectful discussions about privilege, race, and allyship. Students used skills from the SDOH course and discussions on privilege to help with empathy during PEP. PEP modeled several characteristics that can enhance teaching diversity, equity, and inclusion: promoting a safe learning environment, creating clear and achievable learning objectives, learning from the diversity of human experiences, and teaching outside of the classroom or clinic setting (Dogra et al., 2009). As students shared their experience with privilege, racism, and other topics covered, the group supported students and equated their stories and experiences as expertise in the subject matter.
Further, PEP leadership and guest speakers encouraged experiential or reflective learning. Students’ personal experiences were respected as valid and expert testimony in our discussions (Nagda et al., 1999). Students were encouraged to talk about their own experiences and understandings that were relevant to each topic. In order to have these discussions about sometimes challenging topics, authors recognize we had to provide and maintain a safe space and support system for diverse students and guest speakers to share their stories.
Guest speakers and faculty attending meetings understood the importance of creating a non-judgmental space and by doing so they may have allowed students to mirror their behaviors in PEP and even in future settings. Such behaviors may be referred to as the “Power of Modeling” and may have a positive impact on students (Nagda et al., 1999). Encouraging students and speakers to share personal stories and narratives as a way to promote intergroup dialogue and psychological safety is consistent with best practices for incorporating diversity and inclusion into curricula (Davis et al., 2021). Constructing PEP in such a manner that supported intergroup dialogue, small groups, and safe virtual spaces may have contributed to candid findings about difficult or taboo topics healthcare students are not given an opportunity to discuss in their program curricula.
PEP leadership provided articles for students that used a storytelling component to explain issues related to privilege, racism, and leadership. Storytelling allows people to connect and share perspectives and experiences (Fitch, 2020), which are more memorable and impactful than data, facts, and figures (Passon, 2019). Students realized to be effective leaders they must be aware of social issues, be empathetic, have difficult conversations, and be an ally to various communities (Clancy, 2015). Building transparent and trustworthy partnerships in the community can help empower individuals and communities to take control of their health. As a healthcare provider and leader in the community, healthcare providers must recognize key social issues and work with patient communities to build trust to combat health disparities (Green et al., 2002). While it may be difficult to build trust immediately, learning about physical and social communities, including their past and historical injustices, may help build trust as we engage with diverse communities in the healthcare setting.
Implications
In a safe environment, healthcare students want to have uninhibited dialogue about these topics and do not want to shy away from sharing their experiences and learning from others. Knowing this information, leaders and practitioners in allied health related fields can use a model like PEP to shape interaction and understanding among students, especially those from different racial/ethnic groups or even other identities. Leaders in healthcare should be responsive to racial injustice that influence health inequities. Programs or curricula changes modeled after PEP are just one of many ways to increase awareness, empathy, and incremental change that support equitable care and social change for diverse patient populations. Last, to demonstrate to students these topics matter, faculty should be actively engaged in these conversations with their students and help students navigate encounters with diverse patient populations.
Limitations
The authors note several limitations, including a small sample size and limited generalizability, as PEP was exploratory and implemented with four undergraduate students at one large academic medical center in the southeastern US. The one undergraduate program we recruited from had more “non-traditional” students who had full-time jobs and families, so it may have been difficult to work full-time, attend school full-time, care for a family, and complete PEP, which was a voluntary program. Even with a small sample, four diverse students, in addition to diverse faculty guest speakers, brought a range of experiences and perspectives to create rich dialogue and data for analyses. Last, students did not receive academic credit for PEP, which could impact some students, especially those who need to take certain courses toward credit for graduation. Faculty may find approaches to embed PEP within a relevant credit-bearing course.
Future Direction
We better understand how to implement such an important program with undergraduate healthcare students who work with patients and anticipate conducting PEP again but with a larger sample of undergraduate students in various health or health-related programs. A Peer Education Program replica examining graduate-level students in clinical programs may be useful in learning more about what helps students engage in these conversations respectfully and how to help them become effective leaders in addressing health inequities inside and outside of the clinical setting, creating sustainable social change.
Conclusion
The results from this pilot study demonstrate healthcare students may need more time and space to describe their experiences related to race, racism, and privilege and hear from others who negatively experience racism. Key findings provide an opportunity to see how students connect awareness, advocacy, and action to leaders capable of social change. Doing so creates more empathetic providers and may inspire students to become dedicated leaders unafraid to advocate for and support underserved patients and communities. Additionally, students need to see faculty from various backgrounds and identities invested in these conversations. In short, we want to strengthen PEP and normalize these conversations by providing students with a safe and non-judgmental space to discuss topics that impact them, their families, communities, and their patients.
Footnotes
Acknowledgements
This work was supported by the Medical University of South Carolina Office of Humanities with funding from Scholars of Humanities and Arts Research and Education (SHARE) Grants. The work is solely the responsibility of the authors and does not necessarily represent the official view of the Medical University of South Carolina. Authors would like to thank the students who participated as well as the guest speakers who took time out their evening to share their expertise with us.
Author Contributions
Elizabeth Brown: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Resources, Writing-Original Draft, Writing-Review & Editing, Visualization, Supervision, Project administration, Funding acquisition; Dante Pelzer: Methodology, Validation, Formal Analysis, Investigation, Data Curation, Writing-Original Draft, Writing-Review & Editing, Visualization, Supervision; Katrina Black Reed: Resources, Writing-Original Draft, Writing-Review & Editing, Supervision; Chinieka Jackman: Methodology, Formal analysis, Writing-Original Draft, Writing-Review & Editing, Visualization; Madison Kimmell: Methodology, Formal analysis, Writing-Original Draft, Writing-Review & Editing, Visualization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Medical University of South Carolina Office of Humanities provided monetary support for the Peer Education Program with funds from the Scholars of Humanities and Arts and Research (SHARE) Grant.
Ethical Approval
Ethical approval was waived by Medical University of South Carolina Institutional Review Board in September 2020. The project was deemed Quality Improvement/Program Evaluation.
Previous Presentations
This work was presented virtually at the Perry V. Halushka Student Research Day on November 5, 2021. An adapted version was also presented virtually at the Association for Prevention Teaching and Research (APTR) Conference on March 28, 2022.