
Abstract
Teaching the components of health advocacy is straightforward, but fostering young people’s self-efficacy to be health advocates for themselves, others, and their community is more complex. This complexity sometimes renders advocating for health, the basis of National Health Education Standard (NHES) #8, challenging to teach. We utilized a pedagogical approach called biblioguidance to teach this skill to 10th-grade students. The premise of biblioguidance, also called bibliotherapy, is that information, guidance, and even solace can be found through reading and vicariously living story events. To implement this approach, we consulted the literature and created a six-step framework to guide the design, development, and evaluation of a health advocacy curriculum, including young adult novels, guided reading prompts, electronic journals, and small group discussions. Our pre/post-assessment, rooted in NHES #8, evaluated the impact on students’ (N = 168) self-efficacy to health advocate for themselves, others, and the community. Results revealed a significant change (p < .001), particularly in advocating for community health. Further, the teachers found that the curriculum facilitated the discussion of health-related topics in subsequent units. We will continue using the curriculum but expand it to include opportunities for authentic application and qualitative data evaluation techniques.
Keywords
Introduction
The National Consensus for School Health Education (2022) describes advocacy skills as identifying needs, formulating an action plan, creating messages, and applying strategies to promote health. Teaching these components is relatively straightforward, but fostering young people’s self-efficacy to perform them on behalf of themselves, others, and their community is more complex. This complexity sometimes renders health advocacy, the eighth National Health Education Standard (NHES), challenging to teach.
This article demonstrates how biblioguidance, a form of creative arts therapy, can be a pedagogical approach to promoting students’ self-efficacy to perform complex health behaviors like NHES #8. We begin with a dive into this standard and an overview of self-efficacy. Next, we introduce biblioguidance and a six-step process we developed to guide the design, development, implementation, and evaluation of a 10th-grade health advocacy curriculum. Finally, we present our evaluation results and discuss the implications.
Background
The Complexity of NHES #8
When we teach young people how to advocate, we enable them to secure conditions that support the health and quality of life for themselves and others. This idea is the basis of NHES #8: Students advocate for behaviors that support personal, family, peer, school, and community health (National Consensus for School Health Education, 2022). Upon close examination, the standard requires students to apply other NHES skills, including accessing valid and reliable information, decision-making, analyzing influences and social norms, and interpersonal communication (Benes & Alperin, 2022). This is apparent in these NHES indicators:
8.12.2 Create an action plan with advocacy strategies related to a position that promotes personal, family, peer, school, and community health.
NHES 8.12.3 Create a persuasive advocacy message about a position using peer and societal norms, supported by valid and reliable sources, that influence the health of self and others.
Additionally, there is an altruistic component and understanding of others possibly unlike oneself, as evidenced in this indicator:
8.12.5 Demonstrate confidence when using advocacy messages and strategies to persuade others to engage in actions that enhance the quality of life and promote equitable health opportunities for all.
Given these “layers,” students might feel overwhelmed and choose not to advocate. As made clear in the third edition of the NHES (National Consensus for School Health Education, 2022), health education teachers should foster students’ self-efficacy to perform the NHES skills. How can teachers best do that with NHES #8? To answer that question, we need a better understanding of self-efficacy.
Self-Efficacy
Self-efficacy is an individual’s belief in their capacity “to organize and execute the courses of action required to produce given attainments” (Bandura, 1997, p. 3). This belief includes learning and performing tasks to achieve goals and influence events affecting our lives (Centers for Disease Control and Prevention [CDC], 2022). Ultimately, self-efficacy affects one’s choice of activities, engagement, persistence, and affective reactions. For these reasons, it is one of the most powerful predictors of health behavior (Bandura, 1997). Per Bandura, there are various sources of self-efficacy, including opportunities for successful skill performance, vicarious experiences (i.e., modeled or observed), and social persuasion. Knowing these sources, teachers can incorporate them into their pedagogy. Biblioguidance could be one such approach.
Biblioguidance
The premise of biblioguidance, also called bibliotherapy, is that information, guidance, and solace can be found through reading (McNicol & Brewster, 2018; Shrodes, 1960). Benefits include insight into personal dilemmas, a new appreciation for one’s own and other’s cultures, improved coping and interpersonal skills, improved self-esteem, new hope, a sense of agency, empathy, feelings of empowerment, and increased self-efficacy (Banas, Valley, & Chaudri, 2021; Byrd et al., 2021; Heath et al., 2017; Kiser, 2017). When coupled with reflective journaling and discussion, young people can explore their feelings and attitudes and build connections to their lives (Chisholm et al., 2017; Ryan & Hurst, 2021). This is particularly the case with fiction.
When reading fiction, readers observe characters who find support, transcend challenges, and perform behaviors they otherwise might not have thought themselves capable of. This phenomenon is like the vicarious experience that Bandura (1997) suggested fosters self-efficacy. In the case of health-related advocacy, readers might see a character take a stand on behalf of themselves, another, or their community in a way they had not thought themselves capable of. Witnessing this behavior modeled, readers might choose to do the same in a similar situation.
Books also provide readers with new perspectives and insights into others’ “worlds” (Eekhof et al., 2021; Heath et al., 2017; Lucas et al., 2019; Pulimeno et al., 2020; Tijms et al., 2018). For example, in Reading for Action, Boyd and Darragh (2019) demonstrated how young adult literature helps students understand and learn how to address complex social issues like bullying, mental health, health disparities, gender and sexual orientation, and environmental health. This experience could serve as a form of social persuasion, another source of self-efficacy (Bandura, 1997). Given these findings, biblioguidance could be a method to foster self-efficacy to advocate for health.
A Six-Step Process to Implementing Biblioguidance in the Classroom
There is no universal framework to guide a biblioguidance approach; however, several researchers have proposed essential steps (McPherson-Leitz, 2018; Pardeck & Pardeck, 2021). We adapted these for a classroom setting. Our final product was this six-step framework:
a. Determine learner characteristics, including relevant knowledge, attitudes, skills, socioeconomic status, and experiences.
b. Enlist other personnel who might assist.
a. Determine desired knowledge, attitudes, skills, and behaviors.
b. Select, modify, or develop appropriate measurement tools.
a. Decide when the curriculum will take place.
b. Develop learning experiences to elicit desired outcomes.
c. Plot pacing of reading and learning experiences.
a. Select reading materials.
b. Arrange students’ access to the reading materials.
a. Present reading materials in a book talk.
b. Present the desired outcomes, learning experiences, and assessments.
c. Implement the unit per the pacing plan.
a. Assess student performance.
b. Evaluate assessment results and reflect on the experience.
c. Refine unit for future implementation.
In the remainder of this section, we describe our implementation of Steps 1 to 5. We cover Step 6 in the Methodology and Discussion.
Step 1—Identify the Audience, Setting, and Supportive Personnel
The project took place during the 2021 to 2022 academic year in a required 10th-grade, semester-long health education course at a suburban school in Illinois. Illinois Report Card (2022) showed this school’s enrollment to be ~1,500 students, of which 86% identify as white, 6% as Hispanic, 4% as Asian, and <1% each as Black, American Indian, or Pacific Islander. Economically, the majority of the school’s community is middle or upper-class.
The lead author, an academic researcher, chose this school based on an existing research partnership with the second author, the school’s health curriculum coordinator. Two other health teachers also participated. As for supportive personnel, we identified the school librarian, an English language arts teacher, and a school counselor. In later steps, we describe their roles.
During the 2021 to 2022 academic year, there were eight class sections and 215 students. Students were exposed to the curriculum early in the semester after an introduction to wellness unit. This meant they only had a basic foundation of health concepts and skills. General academic levels varied as students were not “tracked” into class sections by level.
Step 2—Determine Desired Outcomes and Acceptable Evidence
Our goal was to impact students’ self-efficacy to act as health advocates. We could not locate an existing measurement tool, so we created our own. See Figure 1. This pre-/post-assessment comprised 16 belief statements rooted in the NHES #8’s 9th-12th grade performance indicators. We grouped statements into three subscales: self, others, and community. For each statement, students rated their agreement on a 4-point scale, ranging from a lot true for me to not true for me. We modeled the statements’ phrasing and scale after the Social Skills Improvement System Social-Emotional Learning survey, which has been widely used with 3rd–12th graders (Gresham et al., 2018; Gresham & Elliott, 2008). After administering our assessment (n = 168), we tested its reliability. The Cronbach’s alpha reliability coefficients for each subscale were: advocacy for self (α = .850), others (α = .872), and community (α = .898). These values are above 0.70, suggesting a high internal consistency (Hair et al., 2006).
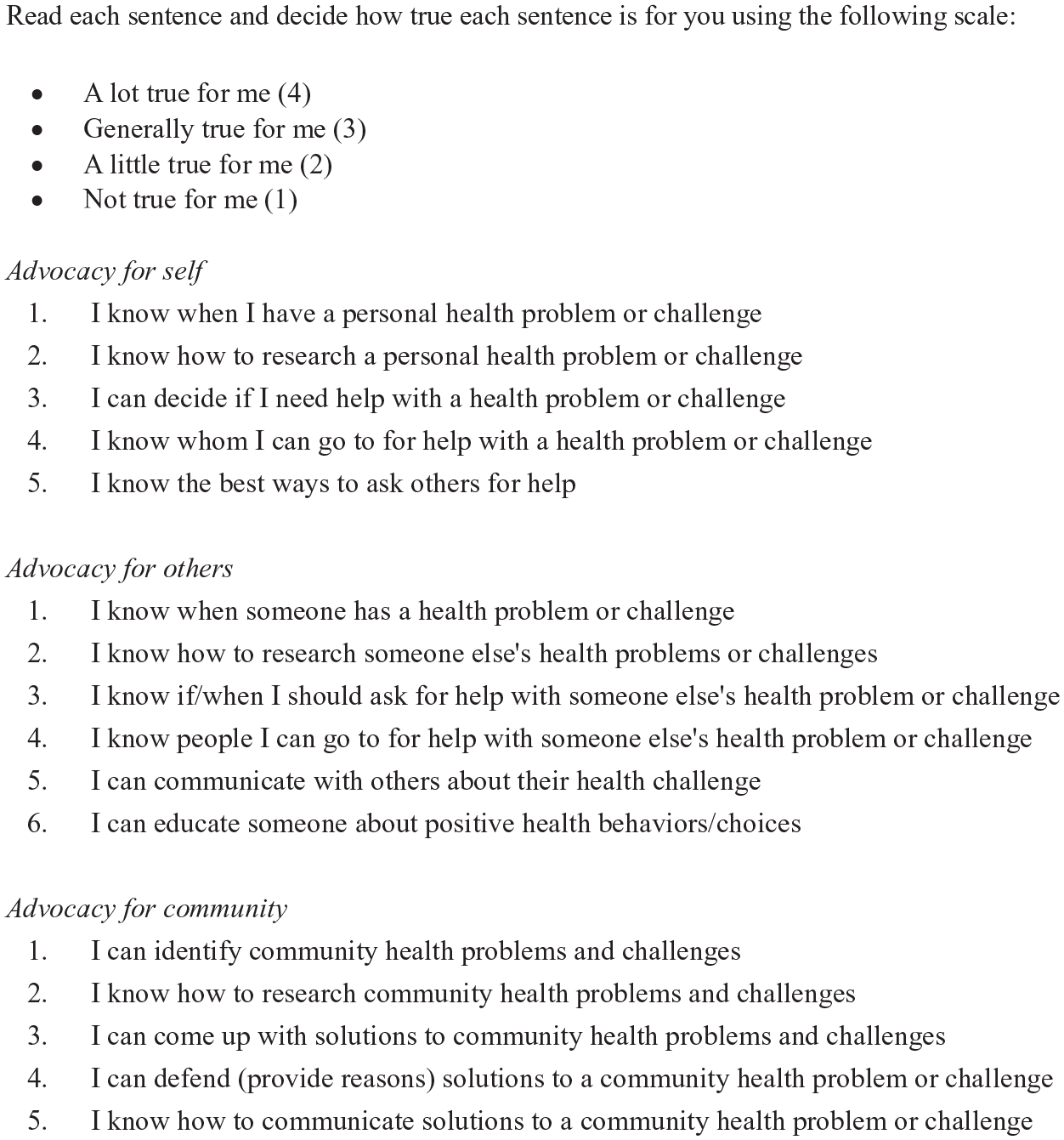
Pre-/post-assessment.
Step 3—Plan Learning Experiences and Instructional Strategies
Recognizing that students needed time to read their books, we spread the curriculum over 4 weeks. This also allowed for other required content to be taught. In our case, that was nutrition, and teachers taught it on Monday-Thursday. On Fridays, biblioguidance instruction, namely discussions, took place. Between Fridays, students read their books and reflected in their journals. We describe these activities next.
Based on our literature review, we knew discussions and reflective journaling were essential to the biblioguidance process. We decided these activities would be rooted in the same guided reading prompts. Students independently responded to the prompts in journals and later discussed them in small groups. To develop the prompts, we turned to four sources: (1) the NHES, (2) Literacy expert Jeffrey Wilhelm’s text called You Gotta BE the Book (2016), (3) the English language arts teacher, and (4) the school counselor.
Earlier, we indicated that NHES #8 requires students to apply several other NHES. These standards are: #2: Students analyze the influence of family, peers, culture, social media, technology, and other determinants on health behaviors. #4: Students demonstrate effective interpersonal communication skills to enhance health. #5: Students demonstrate effective decision-making skills to enhance health (National Consensus for School Health Education, 2022).
It was essential that the curriculum address these NHES to prime students into thinking about health advocacy. We decided to focus on one each week, culminating with NHES #8. The next step was to transform these into reading prompts and ensure students would benefit regardless of academic level.
According to Wilhelm (2016), only expert readers experience the transformation that comes from reading. In a multi-academic-level course, low-level readers could be at a disadvantage. However, Wilhelm contended that teachers could conjure the transformation via reading prompts that push readers through 10 dimensions he organized into three categories:
1. Entering the Story World. 2. Showing Interest in the Story. 3. Relating to Characters. 4. Seeing the Story World.
5. Elaborating on the Story World. 6. Connecting Literature to Life.
7. Considering Significance. 8. Recognizing Literary Conventions. 9. Recognizing Reading as a Transaction. 10. Evaluating an Author and the Self as Reader.
Collectively, these dimensions reflect the actions effective readers take when they create, experience, and respond to literary worlds.
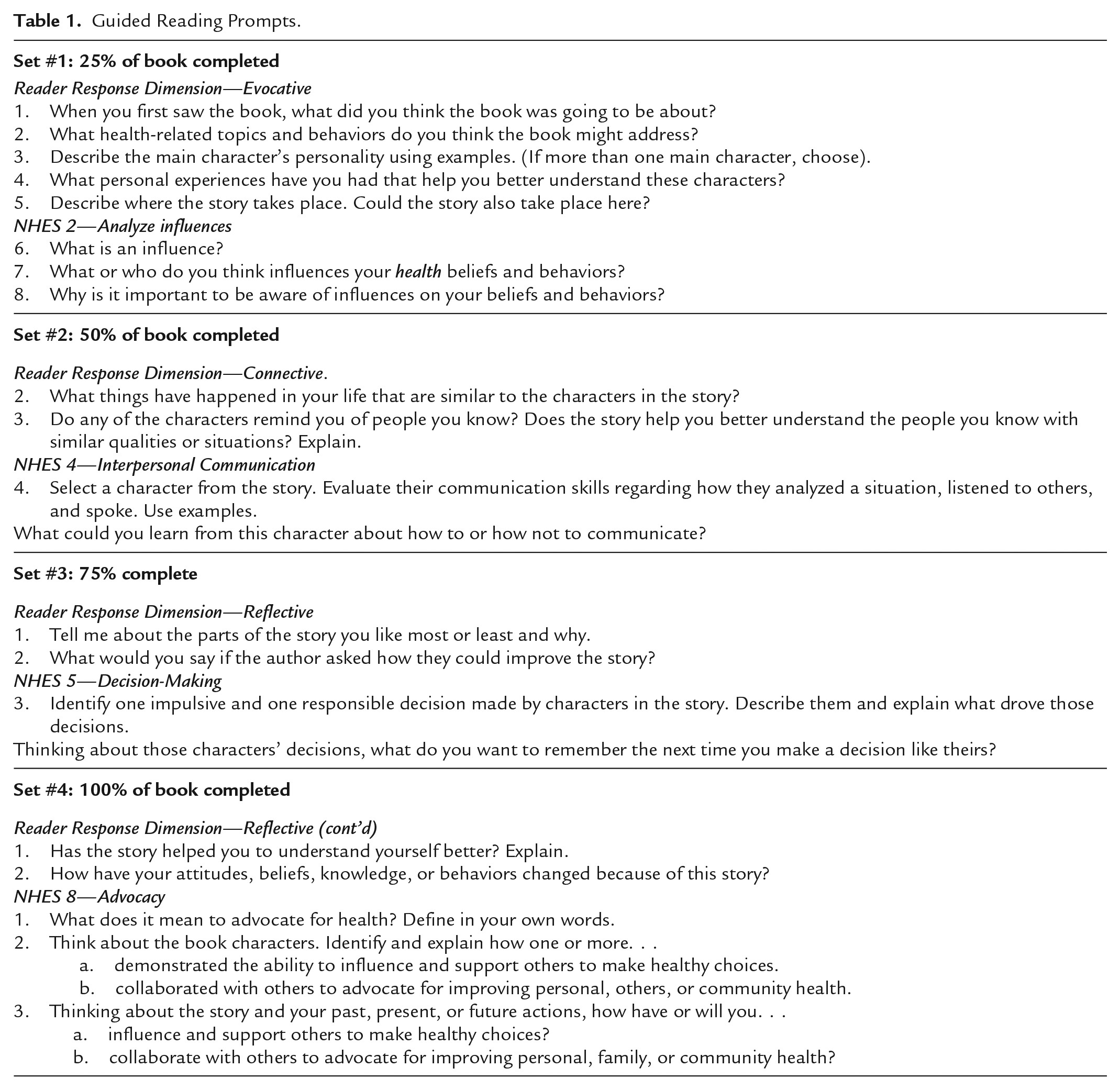
In You Gotta BE the Book, Wilhelm (2016) provided suggested reading prompts for each dimension. We selected a couple from each. Some we left as is; others we transformed to align with NHES #’s 2, 4, 5, and 8. For example, one prompt had readers evaluating a character’s behavior. We rephrased this to focus on NHES #4. Our prompt was: “Select a character from the story. Evaluate their communication skills regarding how they analyzed a situation, listened to others, and spoke.”
We shared our prompts with the English language arts teacher to ensure comprehension and with the school counselor to identify whether any would evoke an adverse emotional response. Our final prompts appear in Table 1. As noted, we assigned the prompts in four sets. For homework, students responded to these in electronic journals (Google Docs with the prompts embedded) after reading 25%, 50%, 75%, and 100% of their book. Then, they discussed their responses in small groups on Fridays each week.
Guided Reading Prompts.
Step 4—Select and Prepare Reading Materials
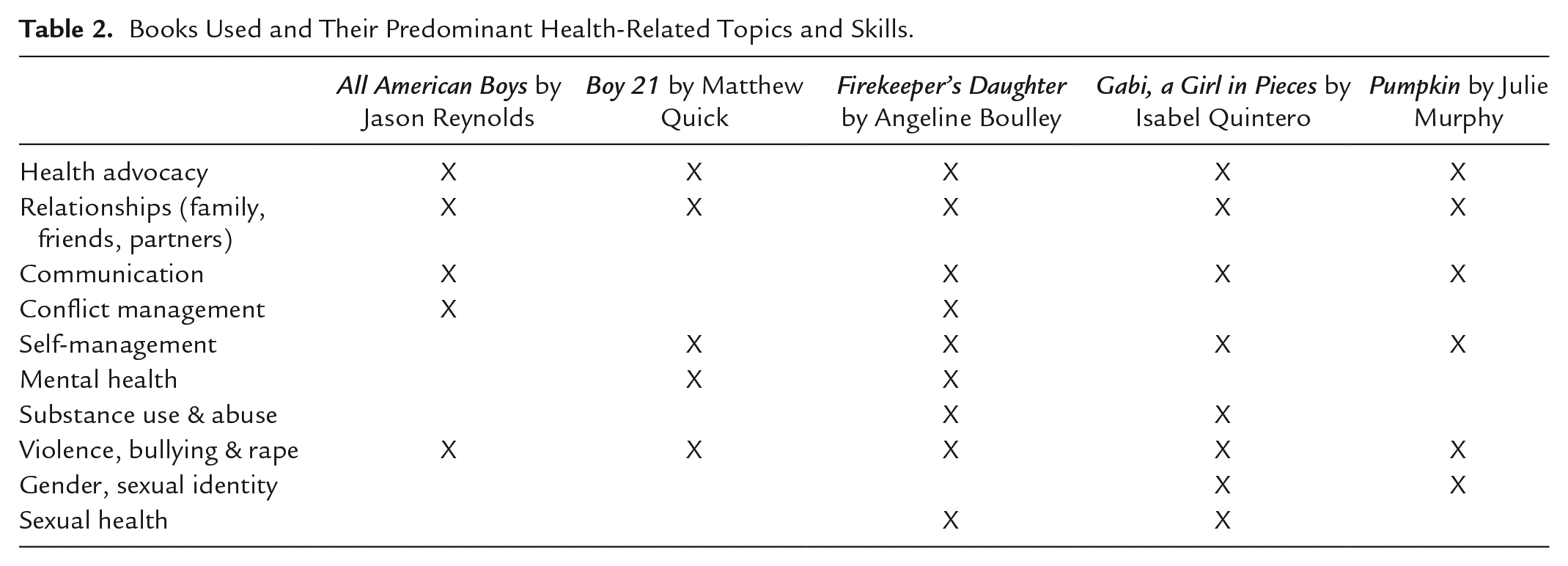
We wanted to provide students with book choices, so we selected multiple texts. We consulted with the school librarian and English language arts teacher, and we reviewed recommendation lists with health and advocacy themes compiled by the International Literacy Association, Teaching for Change, and local libraries. Next, we narrowed our list based on reading level and availability through the library. Then, we read them. Our final criteria were to identify books whose content addressed topics (e.g., communication, substance use, relationships, etc.) also covered that semester so they could double as a point of context. Table 2 shows the books we selected and their topics. Our list is not all-encompassing. We encourage others to consult with their librarians.
Books Used and Their Predominant Health-Related Topics and Skills.
Step 5—Present and Implement the Curriculum
We previewed the curriculum and conducted book talks to help students choose their books. Book talks are short presentations that foster interest in a book, hinting at the plot, characters, and themes. We did this 2 weeks before implementation to allow time to acquire the books. We assigned the first reading prompt set once we acquired and distributed the books. One week later, students discussed their responses with 3 to 5 others reading the same book. After discussions, we assigned the next prompt set to discuss the following Friday. We continued this pattern until students discussed the last prompts.
Step 6—Assess, Evaluate, and Refine
Step 6 includes assessment, evaluation, and refinement. We share this evaluative process in the Methods and Discussion sections.
Evaluation Methods
The evaluation focused on the following question: What impact does biblioguidance have on students’ self-efficacy to advocate for the health and well-being of themselves, others, and their community?
Data Collection and Analysis
The pre-/post-self-assessment we described in Step 2 was the primary data source. Per IRB guidelines, students obtained written parental consent and provided their assent to participate in the study. Of the 215 students, 168 met this requirement. Students did not know which classmates participated. All students completed the self-assessment and received points for completion; however, we only examined the de-identified responses of study participants. We used Qualtrics to administer the assessment and obtain student assent. Students took the assessment before reading their books and again after discussing the last prompts. We used Statistical Package for Social Science to perform paired samples t-tests (repeated-measures tests), which allowed us to calculate differences between pre and post-test scores. To reduce the possibility of a Type I error, the Bonferroni correction was applied to the original alpha, which was set to 0.05. The corrected alpha was determined to be .0167 (α/n = .05/3, with 3 being the number of subscales in the assessment).
Results
Our analysis showed a significant change (n = 168; p < .001), from pre- to post-assessment, in students’ collective self-efficacy, as well as on each sub-scale (also p < .001). See Table 3. The most significant changes were in self-efficacy to advocate for the community, increasing an average of 0.19 on a 4-point scale. The average change in advocacy for self and others was 0.16. While these movements might seem small, they were in a positive direction and suggest that the curriculum may have shifted students’ beliefs. Shifting self-efficacy beliefs about a given behavior is a step toward the increased likelihood that one will perform it (Bandura, 1997). As a reminder, the assessment measured students’ self-efficacy to research, consult, and communicate with others about a health problem or challenge. These activities align directly with the NHES #8 performance indicators. While we cannot assume causation, the biblioguidance curriculum may have shifted students’ beliefs about performing such activities, thus warranting further investigation.
Paired-Samples T-Tests: Impact on Self-Efficacy to Advocate for Health.
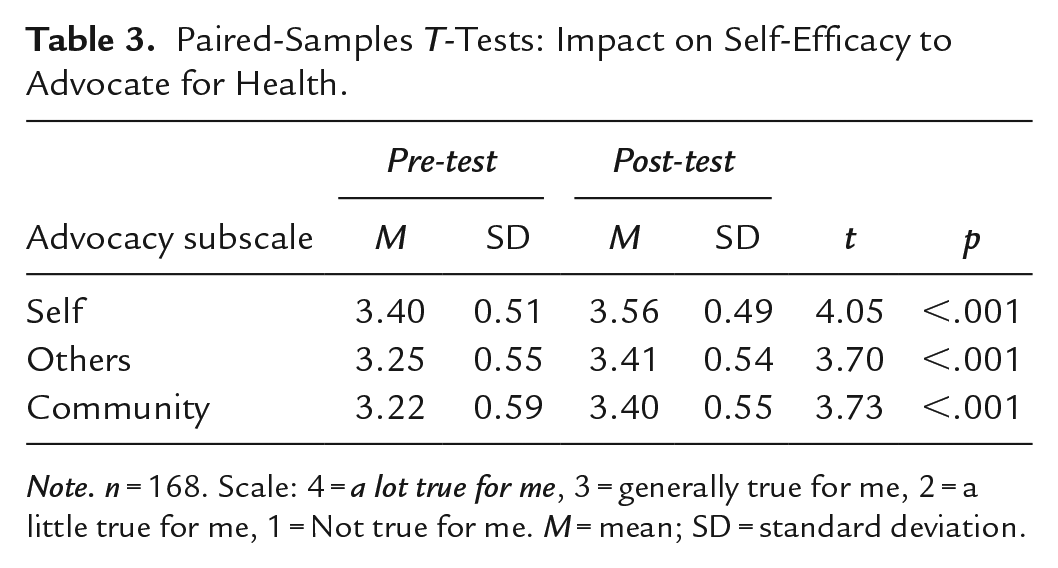
Note. n = 168. Scale: 4 = a lot true for me, 3 = generally true for me, 2 = a little true for me, 1 = Not true for me. M = mean; SD = standard deviation.
Though not formally assessed, teachers indicated that the six-step framework was relatively easy to implement. Also, they appreciated how they and the students could reference book characters and events in subsequent units. While learners may share demographic characteristics, personal experiences will always be different. The books provided a common ground to begin conversations and build new understandings.
Discussion
Each NHES reflects knowledge, beliefs, and skills necessary for young people to adopt and maintain healthy behaviors, achieve health literacy, and enhance their health and academic outcomes. Fostering these outcomes requires creative pedagogical practices, particularly for NHES #8. The root of this standard is being able and choosing to secure conditions that support the health and quality of life for oneself and others, including family, peers, school, and community (National Consensus for School Health Education, 2022). To be effective, one must also possess emotional conviction and the ability to persuade others to believe in a cause (Benes & Alperin, 2022). Self-efficacy is essential to achieving these outcomes (National Consensus for School Health Education, 2022). Our project and the existing literature demonstrate that biblioguidance might be a way to scaffold and foster it.
Biblioguidance has been shown to impact positively impact youth in many ways, including those associated with health advocacy, such as instilling a sense of agency and social empowerment (Byrd et al., 2021; Ford et al., 2019; Ryan & Hurst, 2021). For example, Banas and Gershon (2022) found a positive correlation between biblioguidance and improved self-efficacy to practice social justice. Similarly, Byrd et al. (2021) found that biblioguidance supported young adult African-American males in contending with systemic barriers and increased their self-awareness. Also, Ryan and Hurst (2021) used biblioguidance to help adolescents deconstruct, discuss, and find solutions to bullying. In another study, Ford et al. (2019) found that biblioguidance fostered gifted young African-American girls’ self-efficacy, motivation, and pride in facing social and personal obstacles. Flores (2021) found that biblioguidance supported adolescent Latina girls in expressing their visions for a just world and how they could be part of the solution. Our findings add to this knowledge base and suggest value in considering biblioguidance as an approach to teaching complex health behaviors.
Strengths, Limitations, and Implications
Our project demonstrated that biblioguidance might help students develop self-efficacy to advocate for the health of themselves, others, and their community. While we recognize that self-efficacy is not the only predictor of behavior, nor do we know the long-term impact of our work, the results are encouraging. Longitudinal studies with comparison groups, expanding the project to other schools, or including authentic assessments, such as an advocacy project, would add to the evidence base. Another factor to consider is the impact of external factors. We do not know the effect of other content-area instruction outside the curriculum, nor the impact of other school subject areas, personal experiences, or world events. Focus groups or interviews with students might help to reveal these. We are examining these ideas for future iterations.
Conclusion
Being able to advocate is essential for providing equitable health opportunities for all (National Consensus for School Health Education, 2022). The skills behind NHES #8 empower students to apply functional health knowledge and skills toward securing conditions that support the health and quality of life for themselves and others (2022). Our evaluation findings suggest that biblioguidance could offer a creative pedagogical approach to scaffolding this standard and supporting young people in becoming proactive about health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.