
Abstract
In public health, ethics is a core competency. Accordingly, ethical decision-making should be part of the curriculum for all students seeking to enter the profession. Evidence suggests simulation may positively impact student learning of ethics. Yet, engaging in a traditional simulative or immersive experience is inaccessible to many students. Instead, could participation in virtual immersive experiences serve as a proxy for promoting student outcomes for ethical decision-making in public health? This quasi-experimental mixed methods study examined whether the integration of 360° videos in an undergraduate online health ethics course enhanced intended ethical decision-making. Undergraduate students (n = 26) provided access to two assignments or artifacts. These artifacts were analyzed in accordance with a tailored rubric to explore differences in five constructs of ethical reasoning when writing assignments were completed with (n = 13), or without (n = 13), an integrated 360° video component. The results show the 360° videos enhanced the students’ ability to engage in ethical reasoning, with significant differences in rater scores being noted across multiple constructs. The data were also analyzed qualitatively. Students in the intervention group engaged in a process of “compassionate calculus,” integrating various elements of empathy, compassion, and self-awareness toward a clinical outcome. Together these findings demonstrate the capacity of virtual immersive experience to support students in the enhancement of intended ethical decision-making through the development of greater compassion or empathic concern. This study provides evidence to guide the continued integration of virtual immersive experiences into undergraduate public health education.
Keywords
Introduction
Ethical decision-making is a critical skill for students entering professional health careers, including public health. Almost 20 years ago, writing on behalf of the Institute of Medicine in the U.S. (currently known as the National Academy of Medicine), Thomas (2003) advocated ethics should be taught explicitly, as opposed to accidentally, in all schools of public health. Historically this has not been the case. Since then, this call has been echoed, for example, by the International Union for Health Promotion and Education (IUHPE). In its Core Competencies and Professional Standards for Health Promotion (International Union for Health Promotion and Education [IUHPE], 2016), the IUPHE asserts ethical values and principles for health promotion underpin the competencies and standards listed in all nine articulated domains of practice and considers it the responsibility of education providers to ensure their graduates are equipped with ethics knowledge and skill.
The equivalent core competencies document in the U.S., the Core Competencies for Public Health Professionals, revised most recently in 2020 to 2021, adopts a similar position. The current recommendation is all public health professionals in the U.S. should be equipped to apply ethical principles in their work around policy and programing, education and training, and research, as well as in the context of professional interactions (The Council on Linkages Between Academia and Public Health Practice, 2021). To facilitate such ethics learning, U.S. schools of public health and public health programs outside schools of public health are required to include ethics content in their undergraduate and graduate curricula in order to receive accreditation (Council on Education for Public Health, 2021). Further, the mastery of public health professionals around, inter alia, ethics is examined via the National Board of Public Health Examiners’ voluntary, yet highly recommended certification process (National Board of Public Health Examiners, 2022). Still, teaching public health ethics remains “patchy and somewhat theoretically incoherent” (Potter, 2015, p. 1), within and beyond the U.S.
In the health sciences, teaching ethics has typically involved a combination of developing theoretical understanding, chiefly through traditional didactic instruction (e.g., lectures, readings), alongside supplementary learning activities that foster critical reflexivity, such as small group tutorials. In other words, a straight lecture format is recognized as being insufficient for supporting students to develop emancipatory and practical knowledge, which are critical to ethics education (Potter, 2015). Today, various practical techniques are drawn upon in the learning and teaching of ethics, including moral case deliberation (Haan et al., 2018), and case review and discussion (Thiel et al., 2013). Simulation takes the case study approach one step further, by providing a safe environment for students to engage with, and be immersed in, course content that realistically mimics real life (Buxton et al., 2015). Evidence (e.g., Gallagher et al., 2017; Patterson et al., 2017) suggests simulation, or immersion, may be particularly effective in terms of promoting learning outcomes related to ethical decision-making.
At most universities in the U.S., students have multiple options for engaging in a traditional, physical immersion experience. Short-term internships or fieldwork courses are offered through many majors and minors, Study Abroad programs are in the hundreds, and student organizations host a diverse range of winter- and spring-break experiences. Yet, participating in a traditional immersion experience is out of reach for many students. These experiences often have high tuition or other costs, and students with work or family commitments outside of school, such as adult learners enrolled in online degree programs, may not be able to commit the time. Further, academic departments may be unable to facilitate or support a traditional immersive learning experience for all their students if enrollments are high.
The question arises: Could participation in a virtual immersive experience serve as a proxy for promoting ethical learning among undergraduate students, in particular those on public health career trajectories? This article explores this question by presenting the findings of a recent study that examined whether the integration of a virtual immersive experience, namely 360° videos, into an online undergraduate health ethics course enhances student learning around intended ethical decision-making in public health.
Virtual Ethics: A Literature Review
Technological advancements in the field of virtual reality over the past 5 to 10 years have seen virtual immersive experiences become increasingly accessible to everyday users as costs of necessary equipment (e.g., headsets) dramatically lower (Kesselman, 2016). Virtual immersive experience broadly refers to the act of placing people in virtual and alternative states of the world in time and location. Virtual immersive experiences ask the user to immerse themselves and be present in a computer-based environment that cannot be easily accessed physically for temporal reasons (e.g., traveling back in time to a different historical period), due to physical inaccessibility or danger (e.g., fieldwork in remote locations or areas of civil unrest), and/or because engaging in a certain situation would be unethical (e.g., students performing surgeries as part of their medical training; Freina & Ott, 2015). The uptake and adaptation of virtual immersive experiences has increased significantly following the onset of COVID-19, in (e.g., Dunnagan & Gallardo-Williams, 2020; Tabatabi, 2020) and beyond classrooms (e.g., Mottelson et al., 2021), as people seek to compensate for or ameliorate the diverse impacts of the pandemic, including physical lockdowns and travel restrictions.
In the health sciences, virtual immersive experiences have been shown to effectively facilitate clinical outcomes, whether in the form of preventative health (Ahn, 2015), pain management (Gromala et al., 2015), and/or motivation to engage in behavior change, for example, around nutrition (McGuirt et al., 2020). The primary application of virtual immersive experiences in the health sciences has been in training. This has been with frontline health workers facing potentially high-risk situations, such as health care workers in Liberia exposed to Ebola (Mellor et al., 2016), but the focus has especially been for clinical health care education (Freina & Ott, 2015). According to a systematic review and meta-analysis on the effectiveness of virtual reality for educating health professionals (Kyaw et al., 2019), current evidence demonstrates a small improvement in knowledge, alongside a moderate-to-large improvement in clinical skills, for learners who engaged in virtual reality interventions compared with traditional or other forms of digital learning such as online. Further, research indicates the degree of interactivity seems to matter, as more interactive virtual reality interventions appear to foster higher gains than those that are more one-way virtual reality interventions (Kyaw et al., 2019).
There is no current consensus as to the precise capacities needed for ethical decision-making or for demonstrating one of its core variables, ethical competence. A review of the literature shows ethical competence, defined as “the sensitivity of [managers and professionals] to moral issues. . . followed by moral judgment and actions” (Pohling et al., 2016, p. 450), is not a single construct or personality trait. Rather, as Pohling et al. (2016) demonstrate in their revised version of Hannah et al.’s (2011) framework, at least five factors of personality influence of moral maturation and moral conation processes, which together comprise ethical competence. In particular, self-transcendence values (e.g., universalism), high agreeableness (e.g., straightforwardness, tender-mindedness), and high conscientiousness (e.g., dutifulness, self-discipline), and a general respectful and humble orientation to life seeking equality and welfare of others appear to be critical capacities explaining individual differences in moral processes. Research suggests the ability to engage in ethical decision-making is strengthened when an individual is able to demonstrate empathic concern and personal distress toward another who has been harmed or suffered failure (Chudzicka-Czupala, 2012). In summary, it appears when a problem is highly technical or well-defined, decision-making is task-oriented and logical. However, when values-based decision-making needs to occur, certain aspects of empathy are critical to weighing information, making judgments, and resolving the ethical dilemma.
That empathy is foundational to ethical decision-making begs the question: Can empathy be taught, or are humans born—perhaps to varying degrees—with the propensity to feel what others are feeling? Recent psychological studies attest empathy is not in our genes and individuals do have the capacity to learn to empathize more (or less) intensively. Developing enhanced empathy simply requires us to work on our appraisal processes (Heyes, 2018). However, it is not empathy we need to strive to teach. In the neuroscience literature, empathy is defined as “. . .sharing and understanding the ‘feelings’ of others” (Chierchia & Singer, 2017, p. 248). However, when we see others suffer we do not always empathize with them. Empathizing with another requires one to feel with the other, which can lead to empathic distress and, in turn, protective behaviors such as withdrawal and self-protection. Instead, empathic concern or compassion—that is, concern for the suffering of others combined with the motivation to increase their welfare—can lead to feeling for others and prosocial behaviors such as helping (Chierchia & Singer, 2017).
Recent neuroscience literature (e.g., Brydon et al., 2021; Jütten et al., 2018) asserts compassion can be not only regulated, but trained. Even minor interventions, such as short-term “compassion training,” have been shown to shift empathic responses either toward negative affect (i.e., empathic distress) or compassion (i.e., empathic concern). Traditional strategies for “teaching empathy” include role-playing and imitative play; psychodrama that is, guided dramatic action; mindfulness practices; and, the use of the arts (e.g., music, dance, a piece of still art; Foster & Yaseen, 2019). Beyond this, there is emerging empirical evidence to demonstrate the potential role for virtual immersive experiences in the learning and teaching of compassion or empathic concern. As educational technologies, virtual immersive experiences differ from traditional pedagogies as they position the student as active learner in the educational process, asking them to engage with, interact and manipulate the virtual (or, in the case of Mixed Reality, a blend of physical and virtual) world on their own terms, anytime and anywhere, so as to foster transformative learning (Sharma & Sharma, 2021). Recent studies (Formosa et al., 2018; Herrera et al., 2018) have suggested virtual immersive experiences may be a more effective method of fostering empathy than traditional perspective-taking approaches. To date, however, there have been few, if any, studies of the interplay between empathy, ethics, and virtual immersive experiences as a classroom practice. The present study seeks to address this gap.
The Study
This study employed a quasi-experimental mixed methods design to examine whether the integration of 360° videos in an online, upper-division (i.e., advanced-level, intended for students who have declared their major area of study) health ethics course enhances student engagement and learning in intended ethical decision-making.
Setting
The study took place at State University, 1 a large, public, research intensive university located in the Mid-Atlantic region of the U.S. Admission to the institution is considered competitive and the university is consistently highly ranked in most indices of research and overall quality. While the majority of State University’s 75,000 undergraduates earn their degrees in face to face courses at 1 of 19 residential campuses, the course through which participants were recruited was offered via the university’s online campus in collaboration with the Department of Biobehavioral Health (BBH). BBH has selected ethics as one of the five learning objectives of its undergraduate program. Internally defined as “the ability to understand and apply ethical principles in the conduct of research and professional practice and in the analyses in implementations of health-related policies and programs” (Department of Biobehavioral Health, n.d, p. 4), BBH majors are required to complete at least three credits (e.g., one semester-long course) in either ethics, bioethics, or philosophy prior to graduation.
Participants
Participating students were enrolled in Values and Ethics in Biobehavioral Health Research and Practice, a fully online course, for either the summer or fall semester of 2019. Participants were all BBH majors, the majority of whom were in either their third or fourth year of study, enrolled in the online Bachelor of Science (BSc) in the BBH program, which grants approximately 500 undergraduate degrees per year. Further demographics of the study population cannot be reported here for several reasons. First, student demographic data is not typically released to instructors by online campus administrators for reasons of confidentiality. Second, we did not ask for consent for such data because, with a small sample size, such data would be potentially identifying. Further, breaking the small dataset out into demographic sub-populations would be statistically unsound. Finally, we did not anticipate significant demographic differences within the study sample because students enrolled in the online BSc in BBH program typically move linearly through the curriculum, taking consecutive courses during the fall, spring and summer semesters. Even if demographic differences did exist, and while findings are emerging (e.g., Felnhofer et al., 2012), the literature is unclear regarding the mediating role of identity markers such as gender and race in engagement with virtual immersive experiences. Given this, alongside our previous experience teaching health ethics, we had no definitive reason to believe that the interventions used in our study would be categorically experienced significantly differently across student sub-populations.
Recruitment
Participants were recruited by email by a member of the research team who was not the instructor. Consent was obtained in writing. During the first week of the semester, students were asked to email the recruiter from their university email account, indicating whether or not they consented to being in the study. Further information about the study was provided in the form of a recorded video, made by the recruiter, and accessible via the course learning management system (LMS), Canvas. During the informed consent process it was stressed participation is voluntary and can be stopped at any point during, but not after, the semester, when data analysis would commence; their instructor will not be told of their consent status; and, students will receive the same instruction and no grade penalties if they choose not to participate in the study. All students, regardless of consent status, received a low-stakes course credit (two points toward their final course grade, out of a total of over 200 points) for engaging in the consent process.
The precise impact of extra credit on study participation is not known, but overall rates of participation were somewhat higher than most educational research studies of online courses at the university, which often average approximately 25%. For this study, of the 23 students enrolled in the summer course and the 22 enrolled in the fall course, 13 students per semester participated for a total of 26 participants. Thus, the participation rate was approximately 56%. The summer semester students (n = 13) served as the control group, while the fall semester students (n = 13) served as the intervention group.
Curriculum and Data Collection
Two 360° videos were integrated into the course material prior to data collection. These 360° videos differ from traditional videos as they comprise visuals in which the view in every direction is captured and presented simultaneously (i.e., in three-dimension). This presentation allows the viewer to immerse themselves in the experience and engage with, or manipulate, aspects of their surroundings as if they were part of the scene or story. The sensation or feeling that one is really there in the mediated space, albeit through the connection of technology, is captured by the concept of presence (Cameron et al., 2020).
A 9:53 min 360° video on migrants being rescued from the Mediterranean Sea was identified and accessed via a media library maintained by State University’s digital media technologies unit. This video was aligned with the Lesson 2 discussion board activity, Lifeboat Dilemma Discussion (Assignment 1). For this assignment, students were asked to draw on ethical theory and concepts that had been covered in the course lesson to discuss and justify their decisions around who, out of a group of nine persons, they would pull to safety into a lifeboat with three empty seats. A 6:40 min 360° virtual tour of a hospice facility in London, identified and accessed via YouTube, was integrated into the Lesson 8 writing activity, Death with Dignity (Assignment 2). In this paper, students were asked to respond, in two to three pages, to one of three essay prompts that guided them to consider the ethical issues surrounding end-of-life care, including assisted suicide. The control (summer semester students) and intervention (fall semester students) groups received the same instructions for each assignment, asides from a brief instruction to view the video (intervention group only). Prior to their inclusion in the course, all videos underwent a rigorous review process to ensure accessibility. This review was provided by a team of experts associated with the online campus through which the course was offered. Further details of the requirements for each of these assignments is presented in Table 1.
Summary of Assignments into Which 360° Videos Were Integrated.
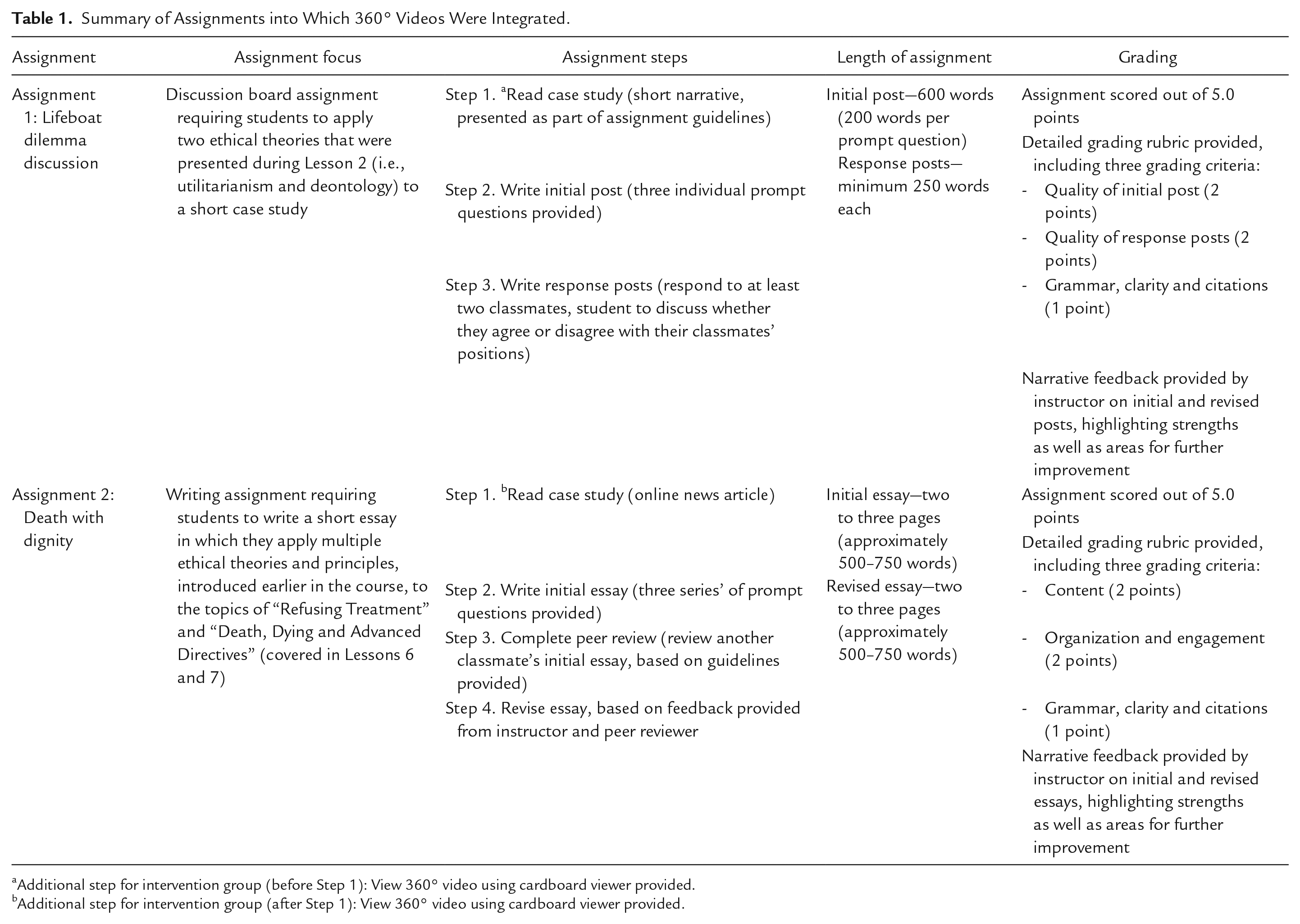
Additional step for intervention group (before Step 1): View 360° video using cardboard viewer provided.
Additional step for intervention group (after Step 1): View 360° video using cardboard viewer provided.
All students in the intervention group course section received a Google Cardboard viewer, a low-cost headset for viewing 360° videos using almost any smartphone, via mail during the first week of class. Full instructions on how to use this viewer to access the 360° videos were provided alongside the Assignment 1 and Assignment 2 instructions. Study participation then took place over the course of the academic semester. Students completed their assignments, with (intervention group) or without (control group) the 360° videos, as part of their regular online classroom activities. Notably, in the control group, no 360° videos or other resources were provided in advance of these two assessment tasks that is, they were merely written tasks. Other than this substitution of modalities (with or without the videos), the content, instructions, and assessment used in both courses, for both assignments, was the same. At the end of each semester, a member of the research team who was not the course instructor copied the two course assignments from consenting students in both course sections and removed all identifying information.
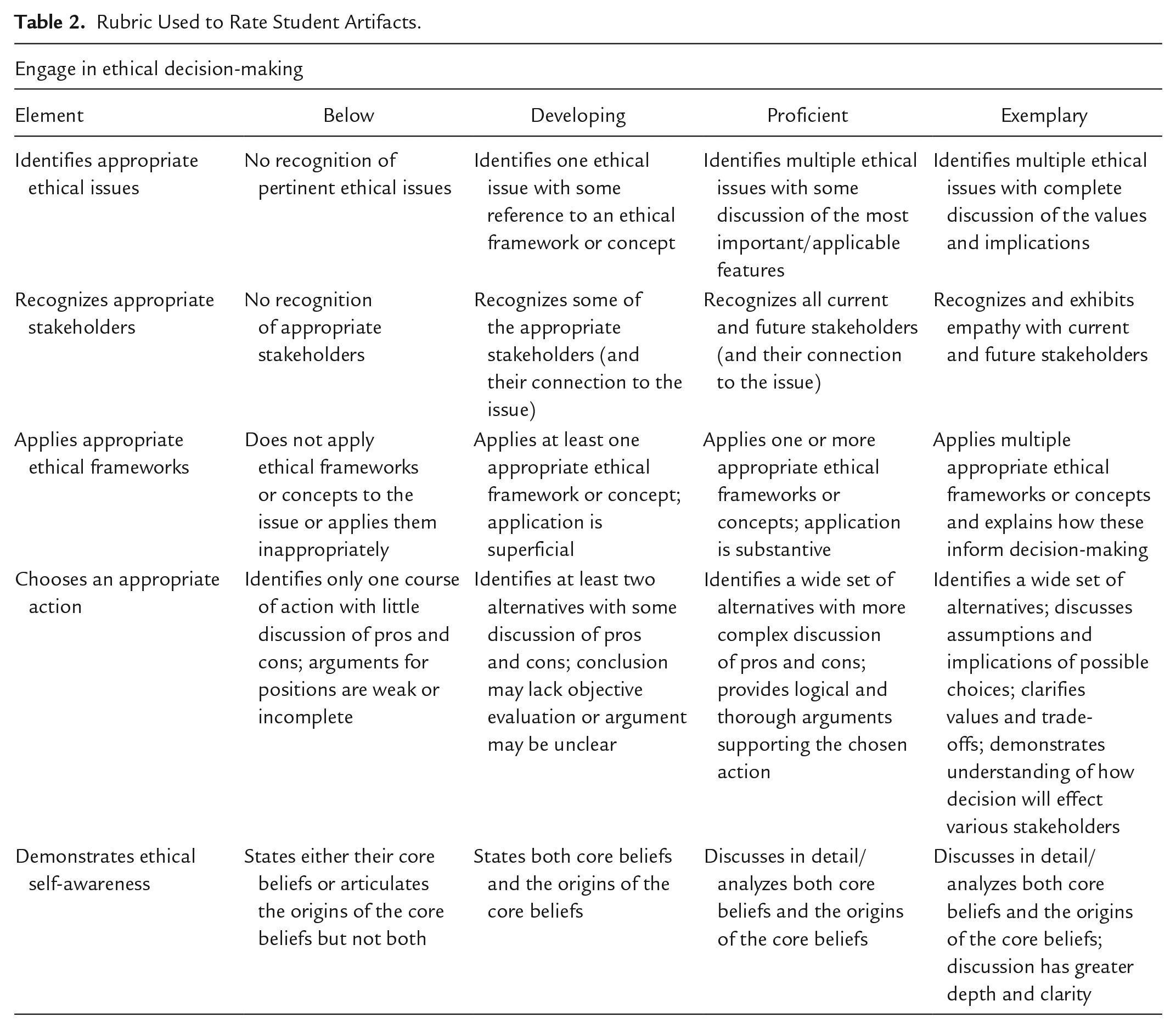
This study sought to identify the impact of the 360° videos on the students’ ability to engage in intended ethical decision-making via ethical reasoning that is, “identifies appropriate ethical issues,” “recognizes appropriate stakeholders,” “applies appropriate ethical frameworks,” “chooses an appropriate action,” and “demonstrates ethical self-awareness.” Prior to the start of data collection, the research team developed a tailored rubric to measure these constructs on a four-point scale based on existing tools, especially the Ethical Reasoning VALUE rubric, developed by the American Association of Colleges & Universities [AAC&U], 2022). A copy of the rubric used to rate the student assignments, or artifacts, is presented in Table 2.
Rubric Used to Rate Student Artifacts.
Data Analysis
In keeping with best practices in direct assessment of learning (Grant et al., 2021), the research team used the prepared rubric to assess the impact of 360° video engagement on student learning outcomes. As there was a potential for loss of confidentiality related to this study (e.g., it was possible that the instructor would potentially recognize the distinctive work of individual students), the course instructor did not serve as one of the raters for the study. Rather, each artifact was assessed by two independent raters who were not affiliated with the course or the instructor. Raters were advanced graduate students who were trained and funded through the university’s Center for Teaching and Learning.
The raters examined the artifacts from all consenting students without knowledge of which group (control or intervention) in which they were included. The raters gave numerical scores (1–4) for each student artifact along the constructs in the rubric, with 1 corresponding to “below” and 4 corresponding to “exemplary.” Four, as opposed to five, scores were considered sufficient as the process did not utilize a neutral option. Inter-rater reliability (IRR) was calculated to determine the level of agreement between the raters for each element in the ethical decision-making rubric. Rater scores were collected via a Qualtrics survey, the results from which were exported as an Excel spreadsheet for the purposes of statistical analysis. Rater scores were averaged for the calculation of significant difference using two-tailed paired t-tests with the control and intervention groups. Because of the relatively small sample size, a p-value of .05 was determined to be appropriate, based on prior Scholarship of Teaching and Learning (SoTL) studies with similar population numbers (Boring et al., 2016).
The evidence from both assignments were also analyzed qualitatively by two researchers not affiliated with the course or the instructor. Similar to the quantitative analysis, the qualitative analysis also utilized a between-groups design, comparing the control and intervention groups, which consisted of separate classes with different students. The qualitative analysis took place in two stages. In the first stage, the members of the research team used an inductive thematic approach, in which each team member read and re-read the student artifacts to identify patterns and repetitions independently. Following these independent readings, the team met with an educational researcher who facilitated peer debriefing and member checks. This stage resulted in the identification of three themes: compassion, self-awareness, and compassionate calculus. In the second stage, these three themes were applied and coded by a single member of the research team, whose work was reviewed by two other members of the research team. All qualitative data were managed via Microsoft Word.
Ethics Approval
Prior to data collection, Institutional Review Board (IRB) approval was sought through State University’s Office of Research Protections. The study was determined as being Exempt (low to minimal risk) following pre-review of the submitted application by an IRB analyst, meaning full review by the IRB committee was not required.
Limitations
This study has limitations. First, the sample size is relatively small, thereby limiting the generalizability of these findings. The ethical decision-making and compassionate calculus of only a limited number of undergraduate students may not be representative for a generalized experience with 360° videos or other virtual immersive experiences, as other students may engage differently. Second, the participation rate for the study was 56%, which means the artifacts gathered are not representative of the entire range of students who took the class. It is possible students who found the intervention (360° videos) appealing and/or effective may have been more likely to participate in the study, and vice versa. Third, students were required to view the videos as a course assignment. However, the LMS does not have the capability to provide analytics at the level of individual students, so it was not possible to confirm all students had watched the videos in their entirety. Adherence was informally confirmed by the instructor through identification of references to the videos in the student assignments and via communication (e.g., email) with the students. Finally, the study did not use a within-groups or randomized design. Therefore, we are unable to conclude a causal association between the intervention (360° videos) and enhanced ability to engage in intended ethical decision-making.
Results
Using a between-groups design comparing the control and intervention groups, each student artifact used in this study was analyzed using the prepared rubric, resulting in a score, or rating, assessing the degree to which the students demonstrated ethical decision-making. The same artifacts were reviewed qualitatively and coded for three themes, compassion, self-awareness, and compassionate calculus, which provided further insight into how students engaged in ethical decision-making processes and why they made the decisions they did for each scenario.
Quantitative Results
The quantitative results of this study reflect a statistical analysis of the scores determined by the independent raters using the tailored AAC&U Ethical Reasoning VALUE rubric.
Ethical Decision Making
The scores determined by the raters suggest the 360° videos provided to the intervention group enhanced the students’ ability to engage in ethical reasoning, as defined by the AAC&U Ethical Reasoning VALUE rubric. The mean, aggregate scores for each of the five elements of ethical reasoning are presented in Table 3, by rater. The IRR (Kappa) for all ratings is 0.70, which indicates a substantial level of agreement (Munoz & Bangdiwala, 1997). In SoTL studies, a IRR of >0.70 is considered sufficient, if not good (Peeters et al., 2013).
Elements of Ethical Decision-Making, Control Versus Intervention Group, With p-Value.
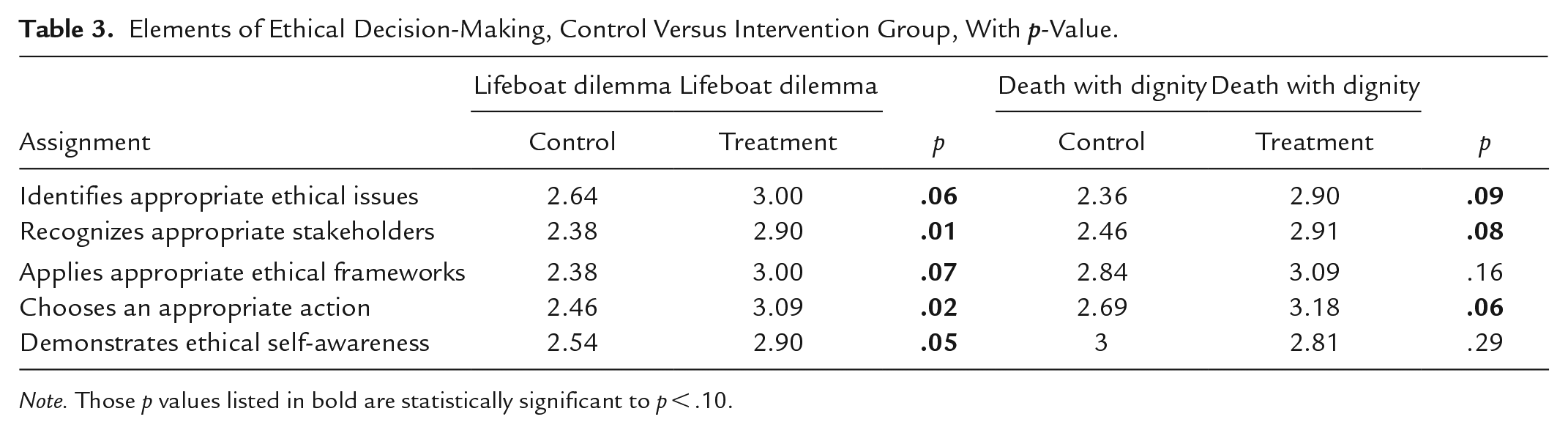
Note. Those p values listed in bold are statistically significant to p < .10.
In all but one case, the rater scores reflected gains between the control and intervention groups, with significant differences noted across three constructs (i.e., “identifies appropriate ethical issues,” “recognizes appropriate stakeholders,” and “chooses an appropriate action”) for both assignments. Significant differences occurred across all five constructs for the lifeboat assignment, and for three of the five constructs for the death with dignity assignment. When compared to the lifeboat assignment, ratings were generally higher overall for the death with dignity assignment, which is perhaps a reflection of its position within the course that is, near the end. These higher baseline scores may also partially explain the slightly higher p-values. Based on this analysis, it was clear the students had strengthened their ethical decision making skills, but questions remained about how they might integrate these skills into their academic and professional practice.
Qualitative Findings
The qualitative coding process identified three additional inter-related themes which emerged from the combined analysis of the two sets of student artifacts papers: compassion, self-awareness, and compassionate calculus. These themes serve to extend the components of the general AAC&U Ethical Reasoning VALUE rubric (assessed through rater scores, as above) toward areas that may be especially salient for public health education.
Compassion
As the quantitative findings above suggest, students in both the control and intervention groups engaged in empathy in the form of taking the viewpoint of another person, but the students who engaged with the 360° videos (intervention group) articulated the extension of empathy toward compassion that is, empathy directed toward helping behaviors (Rowland & Kuper, 2018). Students in the intervention group identified opportunities where additional resources may be needed for example, “. . .the vast majority of families do not have the flexibility, resources and/or time to make all these changes, and [even] if they do, these things are the last steps they want to take in their final days of life,” as well as situations in which participants may require emotional support for example, “I would imagine it would challenge the hearts and minds of most family and friends. They will be faced with a dilemma. Do they convince the person to hold on and suffer in physical and emotional pain, or do they stand behind the person and their decision, which will result in emotional distress for the family member?” These students also identified situations in which appropriate compassion may be lacking from the health care team for example, “. . .the biggest problem with taking away someone’s ability to choose for themselves is that we make them not only physically ill, but emotionally ill as well, causing stress and headache. We make the patient feel incapable of being a human.”
Self-Awareness
The use of first person (“we”) in the previous sentence reflects the second theme, self-awareness, which indicates the student has shifted from viewing the ethical dilemma as a disembodied classroom exercise. Rather, the students in the intervention group indicated increased awareness of how their own moral and ethical perspectives, whether as a person or as a potential health care provider, play a role in how they navigate complex ethical dilemmas with which they may have limited direct experience. This took the form of clarifying their own ethical stance for example, “. . .my father always taught me that the easiest way is seldom the right way, so I face difficult situations with that in mind as well”; recognizing the effect of their beliefs on others for example, “. . .[if a patient asks], I will tell them like it is, but in a nice way, I will not lie about it. Some of them will appreciate my honesty and some will not”; and even identifying their own emotional burden for example, “. . .even though these people are fictional, I felt so badly leaving people behind” or “. . .the thought of leaving a child behind that I had to ability to save [weighs] heavily on my conscience.”
Compassionate Calculus
The weight of conscience was one possible factor the students in the intervention group took into account when making intended ethical decisions, and when engaging in what we call a compassionate calculus, in which they integrated various elements of empathy, compassion, and self-awareness toward a clinical outcome. These calculations seemed to take place regardless of preferred ethical framework for example “. . .using [a deontological approach], I would likely have the most comfort, because I wouldn’t have to make that decision and I wouldn’t have to think about it. As cruel and inhumane as that sounds, it would be the only way that I would be able to live with myself knowing that I left people in the water to die,” or “. . .if I have the means and resources to maximize the good for the greatest number of people [i.e., employ a utilitarian approach], then why not do it? I’m the type of person who will dwell on a situation and ask myself, could I have done more? Could I have done something different to get a better outcome?” Making this calculus is not always easy, as one student remarked, “. . .my heart battled my brain. . .as an African American woman, I do not feel as though people with power follow their codes, laws and morals when it comes down to certain groups of people. Being a victim of this pushes me away from laws, despite being cognizant of the laws and their benefits.”
Discussion and Implications
This study examined whether or not virtual immersive experiences, in particular 360° videos, can foster student engagement and learning around intended ethical decision-making when compared to more conventional, written assignments. The results demonstrate that engagement with 360° videos in an undergraduate online health ethics course does promote ethical decision-making via ethical reasoning, with particular gains noted for recognizing appropriate stakeholders, choosing an appropriate action, and demonstrating ethical self-awareness. No components of ethical decision making ranked lower for the intervention (360° videos) when compared to the control group. This suggests virtual immersive experiences may well be a suitable alternative, or at least a complement, to traditional ethics teaching tools and strategies.
Further, this study suggests introducing virtual immersive experience interventions in other online courses, including those with larger enrollment, or in residential courses, may be relatively straightforward for educators given the current ready availability of cheap cardboard viewers (e.g., Google Cardboard, which cost approximately $10USD each) and Apps. Students would simply need to be supplied with a headset or purchase one on their own as a required course material. Barriers to intervention may include the accessibility of high-quality 360° videos themselves, as well as learning design support to ensure accessibility. However, as shown here, these barriers are surmountable.
These results confirm that engaging in a virtual immersive experience can support students in the development of greater compassion or empathic concern. This finding is consistent with earlier work, including the studies by Herrera et al. (2018) and Formosa et al. (2018), as well as the study by Kalyanaraman et al. (2010), which found empathy toward persons with schizophrenia increased when individuals were exposed to symptoms of the disease via virtual immersive experiences and written materials, but not the latter. These data extend previous work, however, by adding in a third, intermediary piece to the puzzle. This additional piece is compassion or empathic concern. To this end, this study presents new findings around the relationship between virtual immersive experiences, compassion or empathic concern, and ethical decision-making skills (see Figure 1).

Findings around ethical decision-making.
Future research is needed to further these findings, for instance, to empirically demonstrate exactly how and why virtual immersive experiences serve as an effective teaching tool for compassion or empathic concern. Formosa et al. (2018) believe the answer to this question lies in part in the fact virtual immersive experiences do not rely on a teacher to communicate particular knowledge. Rather, they demand the user to personally experience and feel new events in order to make sense of them. In other words, virtual immersive experiences represent a constructionist approach to education. Shin (2018) shares this perspective, asserting immersive experience in virtual reality, in which users feel as if they are part of the action, is not automatically bestowed by the technology per se, but rather is reconstructed by the user themselves. Shin (2018) believes the user follows a two-tiered process of immersion and empathy. In this process, an initial presence (the “I feel like I’m there”-type response) triggers the user to go deeper and selectively experience empathy and embodiment on the basis of their individual characteristics, such as their empathy traits, and the nature of the medium. From a pedagogical standpoint, this raises the question of how virtual immersive experiences may be used to support students in viewing and constructing virtual reality stories to foster the matching mechanism that connects the automatic and more learned processes that comprise and influence an individual’s capacity to empathize (Heyes, 2018). Work is needed to examine how the constructionist capacity of virtual immersive experiences might best contribute to the associative learning that underlies the development or shaping of empathic concern or compassion.
These findings contribute to the exploration of the above questions by demonstrating, for the first time, a potential and important relationship between the variables of virtual immersive experiences, compassion or empathic concern, and intended ethical decision-making. Given the potential impact of these findings for ethics education in undergraduate public health, and broader higher education curricula, further investigation is warranted.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of Drs. Deena Levy and Chas Brua to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Schreyer Institute for Teaching Excellence Scholarship of Teaching and Learning Grant.