
Abstract
Demographic estimates suggest that as the population continues to grow and age in the coming decades, the United States of America will continue to become a more diverse society. The increased diversification of the population makes it urgent for public health professionals, including health education specialists, to master the concepts of cultural and linguistic competence during their academic preparation to be more applied in their professional work. The purpose of this study was to investigate the incorporation of concepts of cultural and linguistic competence in the curriculum among accredited public health schools and programs and other health education and promotion programs to prepare public health education specialists. Point of contact at selected 2021 Council on Education for Public Health list of accredited Schools and Programs of Public Health and an online directory of Health Education and Promotion programs were surveyed. Descriptive statistics were calculated to examine the responses of the participants. While most of the programs reported including cultural competence content and skills in their curriculum, fewer reported inclusion of linguistic competence. Academic programs should prioritize incorporating cultural and linguistic competence in their curriculum not only because of accreditation requirements but because of the moral and professional imperatives presented by the changing demographic changes in the United States.
Keywords
Introduction
Demographic estimates suggest that as the population continues to grow and age in the coming decades, the United States of America will continue to become a more diverse society (U.S. Census, 2020). The growth in the diversification of the population makes it urgent for public health professionals, including health education specialists, to master the concepts of cultural and linguistic competence during their academic preparation to be more applied in their professional work.
The concept and definition of cultural competence have evolved over the last few decades, and while there is disagreement among professionals about the definition, there is a consensus that taking culture and language into account in the delivery of services improves health outcomes across the board. The Office of Minority Health provided one of the earlier definitions as part of the National Standards for Culturally and Linguistically Appropriate Services in Health Care, but even that definition has evolved. Currently, in the health education field, cultural competence is defined as “a developmental process defined as a set of values, principles, behaviours, attitudes, and policies that enable health professionals to work effectively across racial, ethnic, and linguistically diverse groups” (Joint Committee on Health Education and Promotion Terminology, 2012, p. 11). Moreover, the National Center for Cultural Competence (NCCC, n.d.) identifies five “essential” components of cultural competence which include valuing diversity, having the capacity for cultural self-assessment, being conscious of the dynamics inherent when cultures interact, having institutionalized culture knowledge, and having developed adaptations to service delivery reflecting an understanding of cultural diversity. Of similar importance is the concept of linguistic competence, which has been defined as: The capacity of an organization and its personnel to communicate effectively and convey information in a manner that is easily understood by diverse groups including persons of limited English proficiency, those who have low literacy skills or are not literate, individuals with disabilities, and those who are deaf or hard of hearing (NCCC, n.d.: para. 4).
Cultural and linguistic competence (CLC) has been identified as a tool to eliminate health disparities in the USA (Sanchez et al., 2014). Cultural and linguistic competence are top priorities embedded in Healthy People 2030 (U.S. Department of Health and Human Services, n.d.a) the national initiative for improving the health status of US residents. Healthy People 2030 highlights the need to deliver programs that addresses culture and linguistic competency in many of its individual goals and objectives. In addition to Healthy People 2030, several leading public health organizations, including the Office of Minority Health (n.d.) and the Institute of Medicine (2002) have promoted a public health professional workforce that can deliver culturally and linguistically appropriate health programs and services. Increasing cultural and linguistic competence in public health programs and health care organizations has been demonstrated as a sound approach to decreasing health disparities.
National efforts by government entities to promote CLC have translated into initiatives by professional groups and academic institutions. Data from the recent Health Education Specialist Practice Analysis, led by the National Commission for Health Education Credentialing (NCHEC, 2019), identified the need for health education specialists to apply the concepts of cultural competence and cultural humility in several of the sub-competencies of the revised responsibilities for the health education profession. Similarly, an Expert Panel on Cultural Competence Education for Students in Medicine and Public Health (2012) produced a report which identified a set of competencies to prepare culturally competent practitioners and provided recommendations for embedding cultural competency education within and across the curricula of both medicine and public health. Furthermore, the Council on Education for Public Health (CEPH, 2016) requires documented proof that academic programs train future public health professionals to apply their understanding of cultural values and practices to the development and implementation of public health policies and/or programs. CEPH included Diversity and Cultural Competence as part of its 2016 accreditation criteria (Criterion G1) “The school or program defines systematic, coherent and long-term efforts to incorporate elements of diversity.” Specifically, CEPH (2016) states “The school or program also provides a learning environment that prepares students with broad competencies regarding diversity and cultural competence, recognizing that graduates may be employed anywhere in the world and will work with diverse populations” (p. 44). In its guidance to schools and programs of public health, CEPH lists the expectations of the said program: Requisite competencies include self-awareness, open-minded inquiry and assessment, and the ability to recognize and adapt to cultural differences, especially as these differences may vary from the school or program’s dominant culture. Reflecting on the public health context, recognizing that cultural differences affect all aspects of health and health systems, cultural competence refers to the competencies for recognizing and adapting to cultural differences and being conscious of these differences in the school or program’s scholarship and/or community engagement. (CEPH, 2016, p. 44)
The scientific literature along with accreditation criteria highlights the importance of incorporating cultural and linguistic competence into curricular activities. While accredited public health programs must demonstrate the incorporation of these concepts into their curriculum, only a few studies have been conducted to assess the preparation of public health education and promotion professionals. Luquis et al. (2006) found that while most of the programs offering an undergraduate and graduate degree in health education seemed to adequately address cultural competency within their curriculum, most of those programs were not offering courses entirely devoted to these concepts. Few other studies have followed up on the incorporation of CLC into academic preparation programs. Hall and Guidry (2013) conducted a literature review on the cultural competence curriculum and found a small number of articles that addressed this area of the curriculum including the Luquis et al. study, with most of the studies being in the areas of medicine, nursing, and pharmacy education. Powell Sears (2012) provided a framework for medical education to prepare physicians to work with racially and ethnically diverse patients. Similarly, Avila et al. (2016) found a small improvement in participants’ knowledge, attitudes, and comfort in cultural and linguistic competency because of training in this area. Within the field of public health education and promotion, several researchers have assessed cultural competence with service-learning programs (Tremethick & Smit, 2009), as part of pedagogical models (Banerjee & Firtell, 2017), as part of global health curriculum (Chapman & Veras-Estévez, 2020) and a tool to address microaggression in preservice health education (Melendez & Thompson, 2020).
The purpose of this study was to investigate the incorporation of concepts of cultural and linguistic competence in the curriculum among accredited public health schools and programs and other health education and promotion programs to prepare public health education specialists. The study aimed to answer the following questions: (a) how cultural and linguistic concepts and skills are incorporated into programs to prepare the public health workforce? (b) what topics are covered in the courses to prepare the public health workforce for cultural and linguistic competence? and (c) how knowledgeable and comfortable are the faculty members in addressing cultural and linguistic competence issues?
Methodology
Sample Selection
The study participants were selected from the CEPH list of accredited Schools and Programs of Public Health and an online directory of Health Education and Promotion programs (CEPH, 2021; NCHEC, 2018). Only those programs that offer a focus on public health education, health education and health promotion, and/or community health were selected to participate in the study. Based on the description of each of the programs, the authors identified 34 schools of public health, 95 public health programs that offer a master’s degree in public health, and 16 standalone baccalaureate programs for a total of 145 CEPH accredited programs. In addition, the authors identified 13 master’s degree and 11 baccalaureate degree programs that focus on health education and promotion. Both the CEPH list and directory included the names and contact information of the dean, chair, and/or program coordinator. Point of contact at those identified programs were invited to participate in an online survey. While 65 (38%) participants opened the survey, only 55 (32%) of them responded to the first question, leaving 41 completed surveys, for a completion rate of 24%.
Instrument
An updated version of the cultural competence development in health education survey (Luquis et al., 2006) was used for this study. The survey included the definition of cultural competence, linguistic competence, and diversity (CEPH, 2016; Joint Committee on Health Education and Promotion Terminology, 2012; NCCC, n.d.) as these were critical for the aim of the study. The survey included 20 closed and one open-ended questions requesting information regarding the type of degree program the school offers, the type of course(s) in each program with a focus on cultural and linguistic competency, whether the course(s) was required or elective, whether the program provided cultural/diversity training to their faculty. In addition, the survey allowed respondents to select from a list of possible changes needed in the program and to add any other comments. Since most of these questions were descriptive and did not fit a particular scale, the reliability of these items was not calculated. The survey also asked participants to report on each content and skill covered in the courses dealing with cultural competence.
Survey participants were asked to identify which racial, cultural, and/or underrepresented groups were addressed in the course. In addition, participants were asked to choose from a list of 15 cultural and linguistic competence-related content areas, and a list of 15 cultural and linguistic competence-related skills covered in the courses. The authors gather these lists of cultural and linguistic competence-related content and skills based on previous literature and the NCHEC and CEPH expected competencies for public health education professionals. The responses were then coded as yes or no response for each item. Reliability analysis with the current data resulted in a Kuder-Richardson = .77 for the question regarding racial/ethnic/cultural/underrepresented groups, Kuder-Richardson = .85 for content areas, and Kuder Richardson = .87 for the question of regarding skills.
Participants were asked to report the level of commitment, knowledge, the comfort of faculty members in cultural competency, and the level of involvement of faculty members with ethnically/racially/diverse groups outside academia. The responses for these questions include a five-point Likert scale reflecting the response categories of very committed to not committed; very knowledgeable to not knowledgeable; very comfortable to not comfortable; and very involved to not involved. For these four items, a reliability coefficient calculated with the current data resulted in a Cronbach’s alpha = .80. Responses to these questions and reliability results were like those reported during our previous study (Luquis et al., 2006). Participants were provided with the option of requesting a copy of the study results. Those who selected to receive them were instructed to click on a link to a different form where they could provide their contact information. This last step was employed to maintain the anonymity of survey responses since there was no way to link individual survey responses to those who requested copies of the results.
Data Collection and Analysis
The present study followed a descriptive research design over 3 months. Each of the study participants received an email, including a link to the survey explaining the purpose of the investigation, issues regarding anonymity, and contact information for the principal investigator. Implied informed consent was obtained from all study participants as required by the Institutional Review Boards from each institution represented by the authors. Since the responses were anonymous, the research team sent email reminders to all participants every 2 weeks to remind them about the importance of their participation in the study and completion of the survey before the deadline. Each participant received at least five reminders.
The principal investigator received approximately 10 to 15 returned email messages due to the participants no longer working in the institution, and/or changing dean, chair, and/or program coordinator. When possible, a team member attempted to identify the correct contact information of the dean/chair/ program coordinator through the institution’s website and resent the emails to those individuals. In addition, a colleague of the authors posted a message on the Association of Schools and Programs of Public Health online community portal with the hope to yield additional responses. The responses from Qualtrics were downloaded to SPSS (v27) for analysis. The downloaded data file had no identification for the participants. Given the sample size, only descriptive statistics were calculated to examine the participants’ responses.
Results
Characteristics of the Programs
Table 1 shows data about the programs represented in the sample. Most of the respondents (68%) were from Master of Public Health programs and the rest from Schools of Public Health and Standalone Baccalaureate programs (15% and 17% respectively). When asked what type of degree program they offered, over half of the participants reported both undergraduate and graduate degrees (54%), followed by graduate degrees only (36%). A further analysis, not shown in the table, indicated that 67% of the schools of public health offer only a graduate degree in public health, while 61% of public health programs offer both undergraduate and graduate degrees, and 57% of baccalaureate programs offer only an undergraduate degree, respectively. Almost half of the participants (47%) reported that their programs offer both graduate and undergraduate courses that address cultural competency, while 37% offer only graduate courses. However, most programs (54%) do not offer a course addressing linguistic competency, and 35% offer a graduate course or both. Finally, many of the programs (76%) encourage students to take courses outside the program that address cultural and linguistic competency.
Characteristics of the Programs (N = 41).
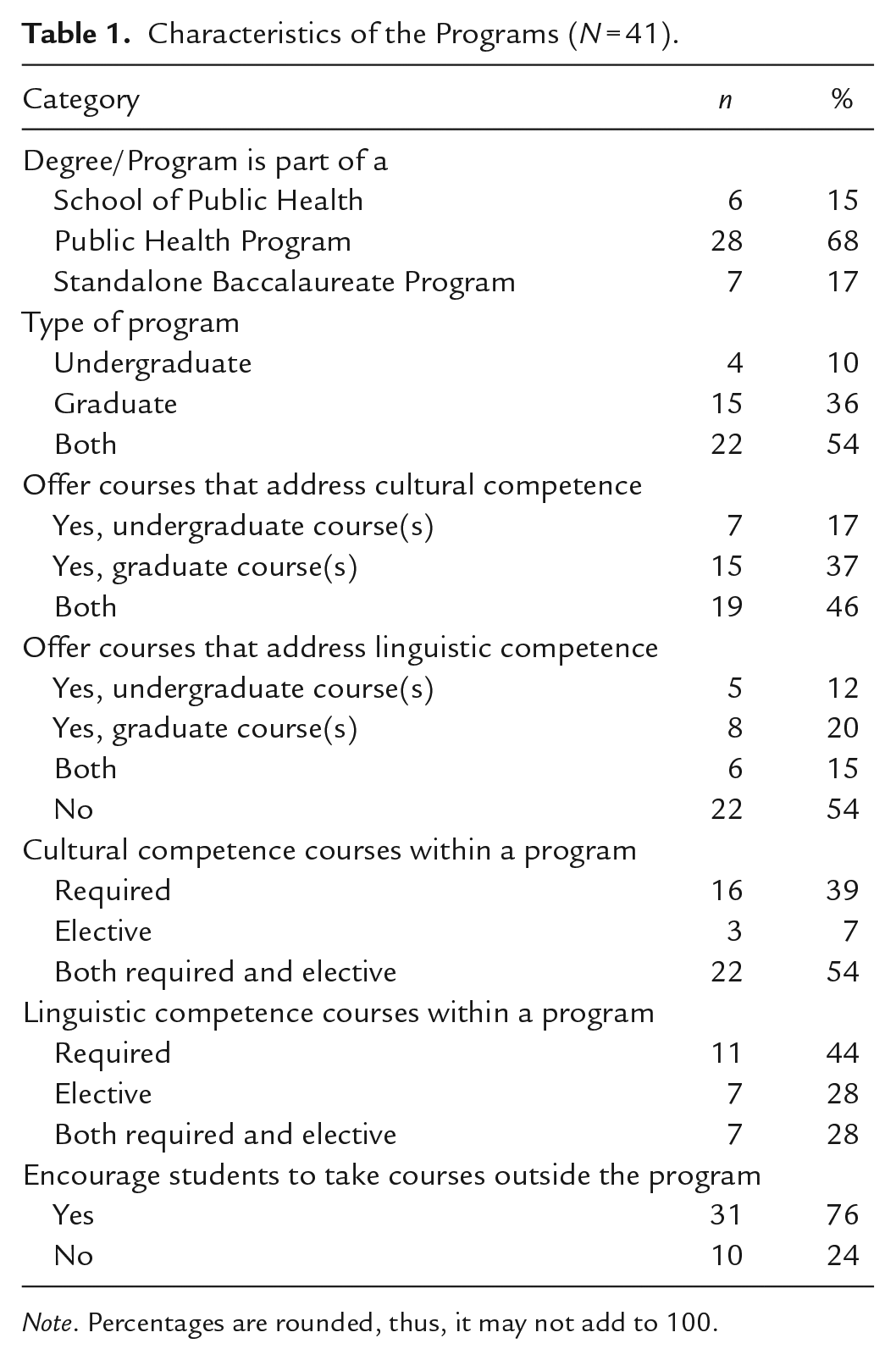
Note. Percentages are rounded, thus, it may not add to 100.
Cultural and Linguistic Competence Content and Skills
When asked which ethnic, racial, cultural, and/or underrepresented groups were addressed in the courses, over 90% selected Hispanic/Latinos, African American/Blacks, and LGBTQI groups, followed by at least 80% who selected Immigrants/Refugees and American Indian/Alaskan Native. Almost three-quarters reported Asians, people with disabilities, and Native Hawaiian/Pacific Islanders as groups that the course covered. Finally, a small percentage reported that the course addresses other groups including the rural population, incarcerated individuals, women and children, elderly, international groups, and/or all the previously mentioned groups equally (see Table 2).
Cultural and Linguistic Competence Content Addressed Within the Courses (N = 41).
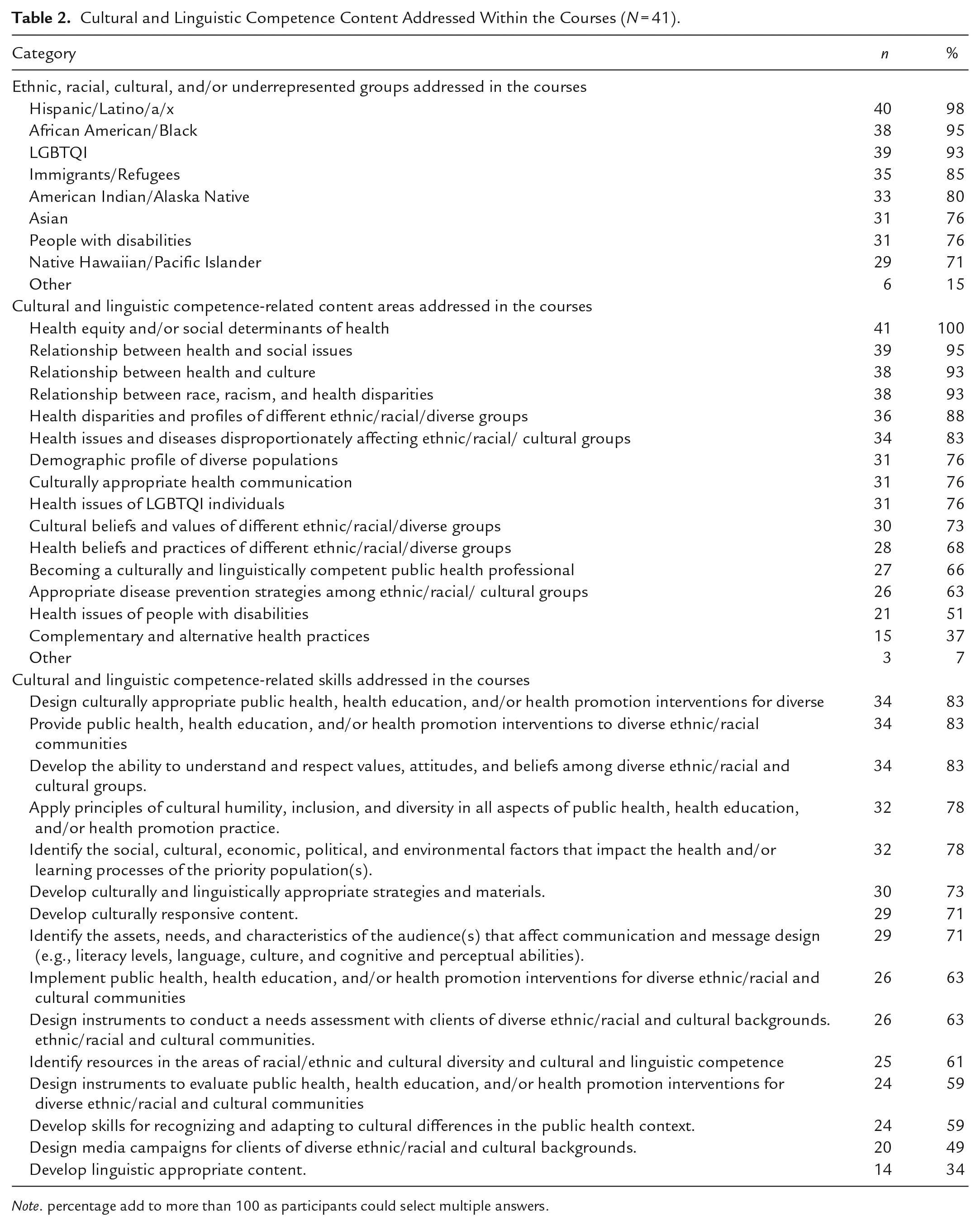
Note. percentage add to more than 100 as participants could select multiple answers.
In response to the question dealing with cultural and linguistic competence skills, over 80% of the participants indicated that their courses addressed how to “design culturally appropriate interventions,” “provide intervention to diverse communities,” and “develop the ability to understand and respect values, attitudes, and beliefs.” Over 70% of the respondents reported that their courses also focused on how to “apply principles of cultural humility,” “identify social, cultural, economic, political, and environmental factors,” “develop appropriate strategies and materials,” “develop culturally responsive content,” and “identify the assets, needs, and characteristics of the audience.” Approximately 60% of the participants reported that their courses also covered how to “implement interventions,” “design instruments to conduct a needs assessment,” “identify resources,” “design instruments to evaluate interventions,” and “develop skills for recognizing and adapting to cultural differences.” Finally, less than 50% indicated that their courses addressed how to “design media campaigns” and “develop linguistic appropriate content” (see Table 2).
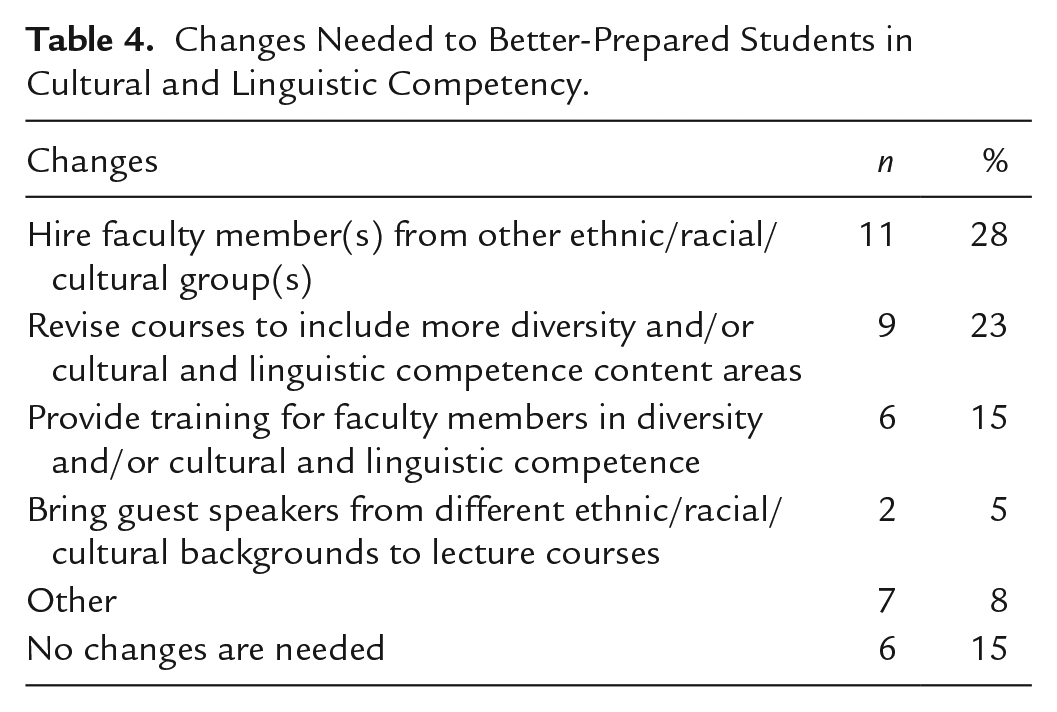
Most of the study participants indicated that their faculty are extremely/very committed (87%) and extremely/somewhat comfortable (93%) addressing issues of diversity and cultural competence. However, participants responded that only 61% of their faculty were extremely/very knowledgeable on issues of cultural and linguistic competence and 54% were extremely/very involved with ethnically/racially/culturally diverse groups outside academia (see Table 3). Almost three-quarters of the participants (71%) reported that their department/ program had provided training in cultural/diversity areas in the past 3 years. Many of them (86%) indicated that they have offered 1 to 6 training programs during that time. Nonetheless, only 41% of those who offered training reported that attendance at the training was required (see Table 3). Finally, participants selected several answers when asked what changes were needed to better prepare students for cultural and linguistic competency. Approximately 25% of survey participants reported that they need to hire diverse faculty or revise courses to include more content areas. Fifteen percent reported that they need to provide training for faculty, and a similar percentage indicated that no changes were needed (see Table 4). Five percent of the participants reported that they would bring guest speakers. In comparison, 8% of study participants reported other changes, including a combination of the one presented above, developing graduate courses, and adding the topic of disabilities.
Faculty Commitment, Knowledge, and Training (N = 41).
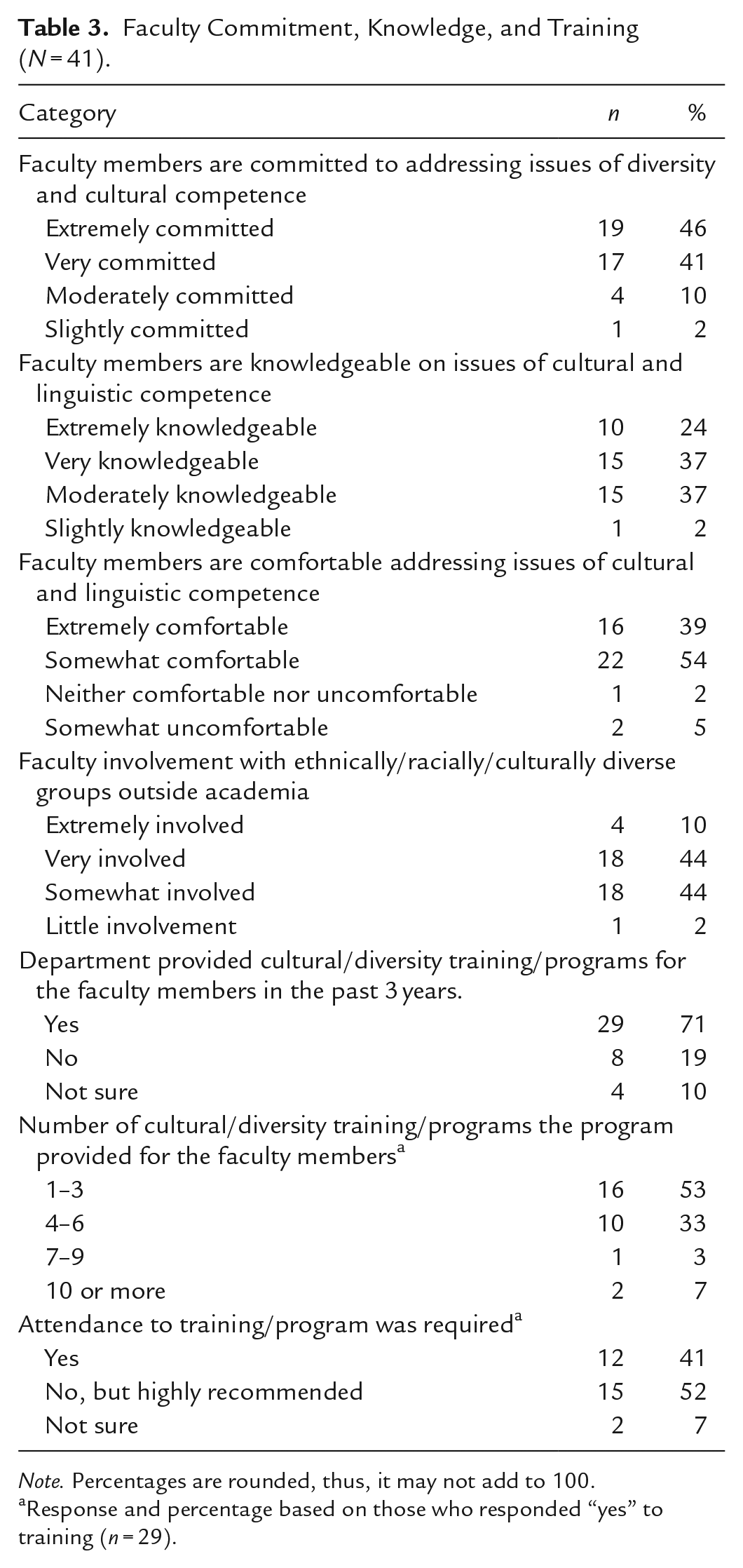
Note. Percentages are rounded, thus, it may not add to 100.
Response and percentage based on those who responded “yes” to training (n = 29).
Changes Needed to Better-Prepared Students in Cultural and Linguistic Competency.
Four participants responded to the open-ended questions. One of the participants noted that for students in the baccalaureate degrees academic service-learning programs may create opportunities to engage with diverse communities, while another participant mentioned that changes to the curriculum would be easier to implement if CEPH required them. One participant stated that health equity and cultural needs are addressed throughout their courses since their program focused on health disparities, and another participant stated that they are doing a lot in this area but can always do more.
Discussion
A few limitations should be considered in interpreting the findings from this study. First, the low response rate limits the generalizations of the results. Like other survey research studies during the COVID-19 pandemic (de Koning et al., 2021; Patel et al., 2020; U.S. Census, 2021), the pandemic may have impacted the response to the survey (i.e., survey fatigue), as it has caused a significant number of demands and stress among faculty members in higher education. As such, the low response rate leads to the question of differences between programs that responded to this survey and those that did not. A second limitation is the inability to compare accredited programs with non-accredited programs based on the limited sample size for the latter. Similarly, no data were collected on the location or age of the programs, which limits the ability to compare programs by geographical locations or how long the program has been in existence. This also limits the ability to speak about the meaning of these findings from a historical perspective of the health education field.
The above limitations notwithstanding results from this study suggest the need to continuously monitor academic offerings related to CLC. Findings from this study showed that public health education programs are responding to changes in professional standards for more culturally competent public health practitioners by providing undergraduate and/or graduate-level courses that address cultural competence. While the findings on cultural competence courses represent an increase from the 27% of programs that reported courses related to cultural competence in the previous study (Luquis et al., 2006), only less than half of all programs are offering dedicated coursework around linguistic competence. Being able to communicate in a language that is understood by program participants and at a level that is appropriate to address health literacy concerns as outlined in Healthy People 2030. Thus, public health education programs preparing the next generation of public health practitioners need to do better to address linguistic competence within the courses they offer. The reduction of programs that refer their students to obtain CLC training outside their program from 87% in 2006 to 76% in 2021 is encouraging. Similarly encouraging is the increase in the number of programs that cover LGBTQI issues in their curriculum from 10% in 2006 to 93% in 2021 (Luquis et al., 2006). Public health professionals need to continue to learn and address issues affecting this community as they have suffered health inequities and have unique health care needs (Cowdery et al., 2021).
Findings from this study suggest that public health programs are making progress toward the inclusion of cultural and linguistic competence in their curricula. The vast majority seem to address diversity in its many facets including race and ethnicity, sexual orientation, disabilities, and immigrant/refugee health. Academic programs also seem to address social determinants of health, culture and social issues, racism, health equity and disparities issues, and culturally appropriate health communication. Similarly, most of the programs are addressing cultural competency, cultural humility, and diversity-related skills. These content areas and related skills are essential in the preparation of culturally and linguistically competent health education specialists (CEPH, 2016; Luquis & Perez, 2021; NCHEC, 2019). Finally, the findings showed that a vast majority of the faculty were committed and comfortable addressing cultural competence areas, which is not surprising as most of the programs had provided training to their faculty. However, only 41% of the programs that provided cultural and diversity training reported that they required attendance for faculty members. Public health education programs should continue to offer cultural and diversity training to their faculty to increase their knowledge and/or maintain their commitment and comfort level in these areas. Finally, future studies could assess the knowledge, commitment, and comfort level of CLC among students attending public health programs, their opinions of whether they are receiving appropriate CLC training and how would they rank CLC knowledge and comfort level among the faculty within their respective educational programs.
Conclusions
Academic programs should prioritize incorporating CLC in their curriculum not only because of accreditation requirements but because of the moral imperative presented by the changing demographic occurring in the United States. As shown during the recent COVID-19 pandemic, health disparities continue to impact underrepresented and diverse populations; hence, health education specialists are compelled to serve these communities. Arguably, having CLC-trained public health professionals is more important now than ever, as they would be better equipped to address the needs of these populations.
Findings from this study also suggest the need for more schools to hire faculty members from diversified cultural backgrounds, as diverse faculty brings different perspectives when teaching CLC-related content that is beneficial for the students. In addition, faculty should participate in training on how to incorporate CLC across the curriculum to ensure that these concepts are incorporated into more than one course. The inclusion of guest speakers from different ethnic and cultural backgrounds, who are working with diverse communities, provides another learning opportunity for students to understand how to address the needs of these communities. Currently, a lot of the recommendations for CLC have been adopted and adapted from health care. Given the significance of this topic, it might be time to call for a series of consensus statements and recommendations which are specific to public health education like those reported from other fields (Charity & Mallinson, 2017; Kaihlanen et al., 2019). For example, in 2000 the Office of Minority Health introduced the National Culturally and Linguistically Appropriate Services (CLAS) standards, which established a blueprint for health care and health care organizations to advance health equity and address health disparities (U.S. Department of Health and Human Services, n.d.b). It is time for professional organizations and accrediting bodies to develop guidelines along with measurable objectives to help public health programs in their quest to fully integrate CLC into both graduate and undergraduate curricula. Until the time that CLC is incorporated into 100% of academic programs, organizations like CEPH and NCHEC should continue to assess the incorporation of CLC into the professional preparation of future public health practitioners, and, more specifically, health education specialists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.