
Abstract
Treatments based on applied behavior analysis (ABA)—an applied science of human behavior—have been increasingly recognized in public policy, both at the federal and state levels. Despite this recognition, however, the relative newness of the science often raises questions about the nature of the treatment approach and the qualifications and regulation of its practitioners. Thus, the present article is a primer on the features of ABA most relevant to public policy stakeholders, including professional certification, licensure, and workforce expansion.
Tweet
The high demand for ABA services has resulted in the rapid growth in the number of credentialed practitioners around the world in recent years.
Key Points
Applied behavior analysis has been demonstrated as a highly successful treatment approach in a variety of areas, including autism, substance abuse treatment, gerontology, brain injury rehabilitation, and occupational safety, among others.
In less than two decades, the BACB has credentialed more than 50,000 behavior analysts and behavior technicians in more than 70 countries, and there are no indications of a slowdown in growth trends.
In less than a decade, half of U.S. states have passed laws to regulate practicing behavior analysts.
Most U.S. licensure laws rely on the BACB’s credentials or standards, which reduces costs to states and facilitates practitioner mobility across state lines.
Introduction
Treatments based on applied behavior analysis (ABA) are becoming increasingly recognized by governments as effective approaches for solving problems of human behavior. At the U.S. federal level, for example, ABA treatments have been written into special education law (Individuals with Disabilities Education Act, 2004), are used for occupational safety by the U.S. Department of Energy (2003), are used to improve outcomes in probation systems (Taxman & Rudes, 2013), and are funded by federal health plans (TRICARE, 2016). At the state level, ABA treatments have long been implemented and funded for developmental disabilities treatment within state education and disabilities departments, are increasingly funded by private health plans (Autism Speaks, 2016), and have been used for various purposes within municipal systems (e.g., drug courts; Marlowe, Festinger, Dugosh, Arabia, & Kirby, 2008). In addition, licensure laws for ABA practitioners have been passed in 25 states within the past decade. ABA is a relatively new applied science and, thus, many policy stakeholders may have questions about the treatment approach and those who generally provide it. The present article is a primer on ABA and the credentialing of its practitioners, which should be relevant for legislators, government administrators, and funders as they encounter the treatment approach in their respective policy arenas.
ABA
Behavior analysis is the science of behavior and its roots extend back to the early 20th century (Skinner, 1938, 1945; Watson, 1913). Its underlying philosophy is behaviorism, which is based on the premise that attempts to improve the human condition through behavior change (e.g., education, behavioral health treatment) will be most effectively served if behavior itself is considered the proper subject matter rather than less tangible concepts such as the mind and the self (Skinner, 1953). To date, basic behavior-analytic scientists have conducted thousands of studies with humans and nonhumans to identify the laws of behavior; that is, the predictable ways in which behavior is learned and changes over time. The underlying theme of much of this work has been that behavior is a product of its circumstances, mainly the events that immediately follow it. Applied behavior analysts have taken this information and developed numerous techniques and treatment approaches for analyzing and changing behavior to improve lives. Because this approach is largely based on behavior and its consequences, the techniques generally involve teaching individuals more effective ways of behaving and making changes to the social consequences of existing behavior (Lerman, Iwata, & Hanley, 2013). ABA has been empirically shown to be effective in a wide variety of areas of concern, including parent training (Franks et al., 2013), substance abuse treatment (Silverman et al., 2007), dementia management (LeBlanc, Raetz, & Feliciano, 2011), brain injury rehabilitation (Heinicke & Carr, 2014), and occupational safety intervention (Geller, 2005), among others. However, because ABA was first applied to the treatment of individuals with intellectual disabilities and autism, it has the largest evidence base and has received the most recognition for work with these populations (Eldevik et al., 2009; Lovaas, 1987; National Autism Center, 2015). For almost 60 years, ABA has been refined and expanded and has now reached the point of growth where many required features of a mature profession have emerged: a robust literature of evidence-based practices, organized university training curricula, standards of professional and ethical practice, public policies, and professional credentials.
Professional Credentials
The regulation of members of a profession is primarily accomplished through two types of credentials (Green & Johnston, 2009). First, regulation can be offered through professional certification, which usually involves a private organization within a profession that establishes requirements for entry into the profession, often through education, training or experience, and passage of an examination, as well as ongoing credential maintenance requirements (e.g., continuing education). Certification programs may also issue a code of conduct for professional ethics and serve as the disciplinary entity for the profession. However, a defining feature of professional certification is that it is often considered voluntary (i.e., not required in order to practice the profession), although certification may be required for purposes such as service reimbursement. The second most common form of regulation is licensure, which in the United States originates in state law. Licensure often includes the same functions as certification (e.g., establishing eligibility and maintenance requirements), but also legislatively defines a profession’s scope of practice (i.e., the activities that are permitted or restricted for individuals practicing a profession) and protects the use of certain occupational titles. Certification and licensure sometimes interact when licensure statutes require professional certification as a requirement for obtaining a license.
The regulation of practitioners in any profession, regardless of the mechanism, is done primarily for two reasons. First, professional regulation helps protect the public by establishing a minimum level of demonstrated competence for those who are publicly identified with a credential (e.g., licensed physician, certified speech therapist) and also by enforcing ethical and professional conduct standards for the profession. Second, regulation of practitioners can protect a profession by ensuring that those who hold the credential meet explicit standards of that profession.
The story of regulation within a profession is typically one of growth. After a profession establishes services that are valued by the public and a certain number of practitioners are available to begin providing services, initial regulatory efforts are begun. For example, the first U.S. state medical boards emerged in the 1870s and by the early 1900s there were medical boards in all 50 states (Johnson & Chaudhry, 2012). As an example of a newer profession, the first speech–language pathology licensure board was authorized in 1969, and by 2012, all states had licensure for the profession (Boada & Crowe, 2012). Throughout these growth periods, one typically sees the expansion of university training programs, refinement of credentialing standards, and an increase in the number of practitioners. This same developmental trajectory has been occurring in ABA over the past decade.
The Development of ABA Practice
The roots of ABA can be traced back to the late 1950s, when initial reports of the success of behavioral treatments were first reported (e.g., Ayllon & Michael, 1959). In the 1960s, the first behavior analysis graduate training programs were beginning to emerge (Baer, 1993; Michael, 1993), and by 1968, there was a need to establish a dedicated scientific journal for ABA research (Journal of Applied Behavior Analysis), which published the first official definition of ABA (Baer, Wolf, & Risley, 1968). Most applied research conducted and ABA services delivered in the 1960s involved individuals with intellectual and developmental disabilities, although not exclusively. The 1970s and 1980s saw the further expansion of university training and increasing diversity of ABA practice across a variety of areas (Fisher, Piazza, & Roane, 2011). In the 1990s, the dissemination (Maurice, 1993) of the success of ABA treatment for children with autism spectrum disorder (ASD; for example, Lovaas, 1987) led to a substantial increase in demand for ABA practitioners. Subsequent widespread efforts to include health insurance coverage of evidence-based autism treatment further accelerated the growth in demand for and the training of ABA practitioners, especially in the autism area. Throughout this multidecade developmental period, the need to identify ABA practitioners using a professional credential became increasingly apparent.
The Behavior Analyst Certification Board® (BACB®)
In 1998, the BACB® was founded as a 501(c)(3) nonprofit corporation whose primary focus was to develop professional ABA credentials. The BACB offers three certification credentials for ABA practitioners at different educational levels: the Board Certified Behavior Analyst® (BCBA®) for individuals with a master’s degree or higher, the Board Certified Assistant Behavior Analyst® (BCaBA®) for individuals with a bachelor’s degree, and the Registered Behavior Technician™ (RBT®) for individuals with a high school diploma. In addition, behavior analysts who hold the BCBA credential and meet additional doctoral degree requirements may qualify for a doctoral designation: Board Certified Behavior Analyst–Doctoral™ (BCBA-D™). Although individuals who hold the BCBA credential may practice independently, both BCaBAs and RBTs must receive ongoing supervision by a BCBA.
Each BACB credential requires a degree, behavior-analytic instruction, and supervised experience as eligibility requirements (see Table 1). Applicants who meet their eligibility requirements are permitted to take the respective BACB examination. All BACB examinations have been professionally developed and are scored and maintained by a trained psychometrician. All of the examinations are based on content task lists, which are practice competencies derived from extensive job analysis studies that include input from experts and practitioners (Johnston, Mellichamp, Shook, & Carr, 2014; Shook, Johnston, & Mellichamp, 2004). The BACB’s examinations are administered by the Pearson VUE corporation, which operates a large worldwide network of secure, computer-based testing facilities. After passing their examination, all BACB certificants enter an ongoing cycle during which they must actively maintain their credential, which includes continuing education for the BCBA and BCaBA credentials and periodic direct-skill assessments for the RBT credential.
BACB Credentials and General Eligibility Requirements.
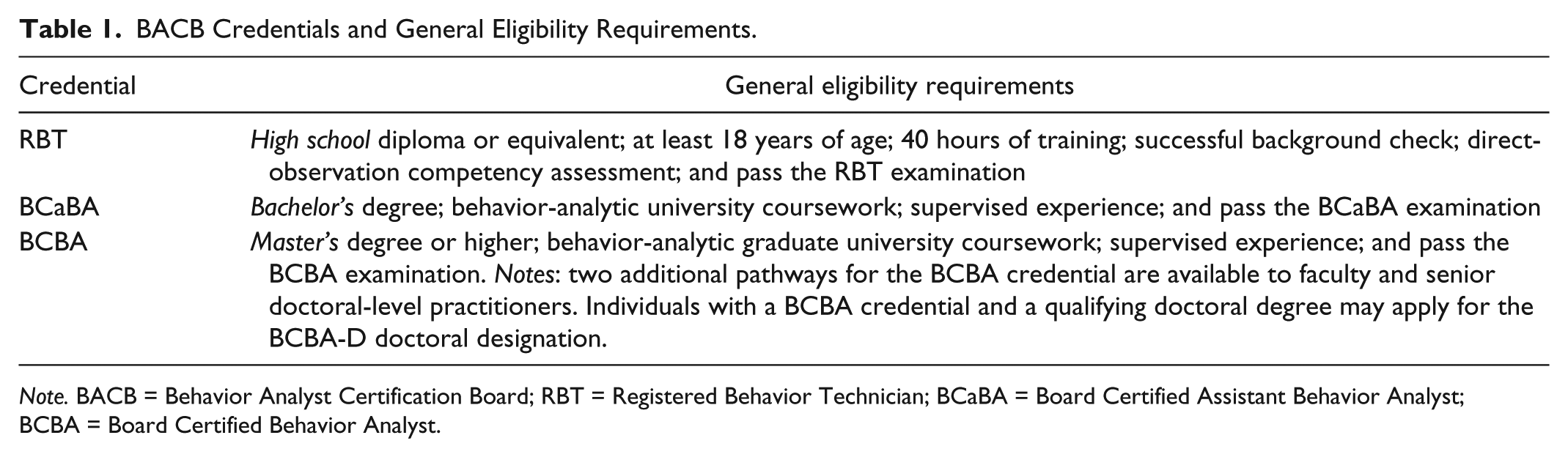
Note. BACB = Behavior Analyst Certification Board; RBT = Registered Behavior Technician; BCaBA = Board Certified Assistant Behavior Analyst; BCBA = Board Certified Behavior Analyst.
The BACB adheres to established testing and legal standards for boards that grant professional credentials (American National Standards Institute, 2016; Institute for Credentialing Excellence, 2016; U.S. Equal Employment Opportunity Commission, 1978). Indeed, the BCBA and BCaBA certification programs have met the rigorous standards of and achieved formal accreditation by the National Commission for Certifying Agencies in Washington, D.C. (Institute for Credentialing Excellence).
In addition to the credentialing standards described earlier, the BACB has developed several other standards and resources related to the training of behavior analysts and the practice of behavior analysis. The BACB has established standards for university coursework and experiential training systems and recognizes universities that meet these standards. There are now more than 300 universities worldwide that offer BACB-approved training programs. In addition, the BACB’s Professional and Ethical Compliance Code for Behavior Analysts (BACB, 2016) serves as the foundation of the professional disciplinary system for its certificants. The Compliance Code is enforced by the BACB through a process designed to provide consumer protection, appropriate due process for the certificant involved, mentorship where appropriate, and consequences to the certificant for violations. The results of significant disciplinary actions, including those that involve suspension or revocation of an individual’s certification, are posted on the BACB’s website (www.bacb.com). The BACB has also developed standards for training supervisors, standards for approving continuing education providers, and practice guidelines for ABA treatment of ASD (BACB, 2014). Finally, a public registry listing of all BACB certificants is available at the BACB’s website.
The Growth of ABA Practitioners
The behavior analysis discipline has grown substantially in recent years, as has the number of its ABA practitioners. Figure 1 depicts the number of individuals holding the BCBA, BCaBA, or RBT credential per year since the BACB’s credentials were first made available in 1999. The number of BCBAs grew steadily in the early years, but approached a near-exponential rate increase in the most recent half-decade. There are now 22,274 BCBAs worldwide. The growth of BCaBAs has been substantially more modest as there are fewer governments and funders who recognize this bachelors-level credential. There are now 2,439 BCaBAs worldwide. The RBT credential was first made available in August 2016, and approximately 2 years later, the number of RBTs (26,429) has exceeded the number of BCBAs and BCaBAs combined.
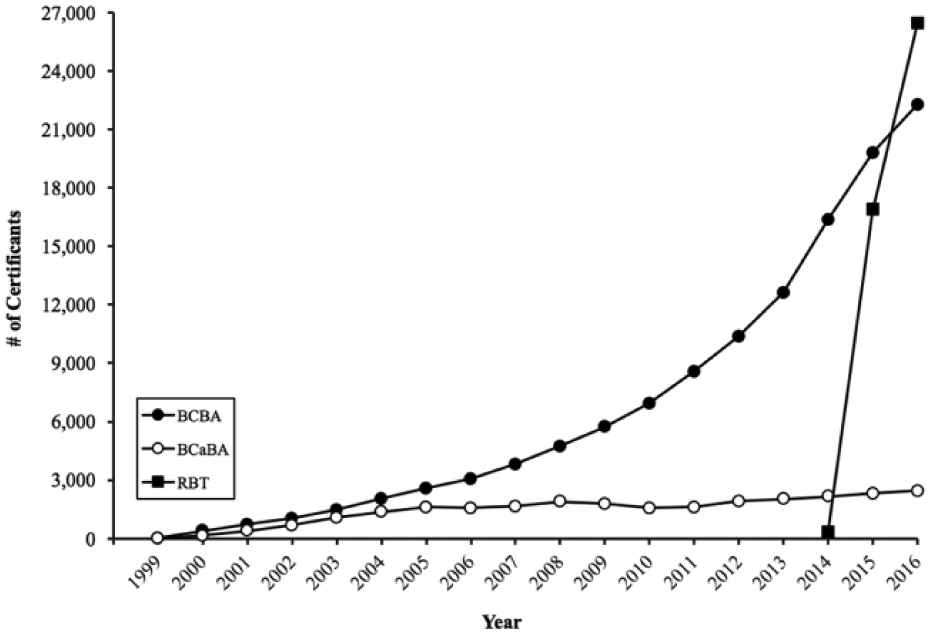
Number of BACB certificants worldwide per year by certification type.
Growth in the number of BACB certificants is likely a result of at least two factors. The most significant factor has been the increasing demand for ABA practitioners. As the ABA research database grew over the years, its effectiveness as a solution to numerous problems, including the treatment of autism, became more well known and the demand for services increased. The data in Figure 1 depicting the number of ABA practitioners per year represent “supply side” data. However, analyses of employment demand for ABA practitioners also show similar increasing trends (Burning Glass, 2015). Another important growth factor in the number of ABA practitioners has been the increasing number of states that have passed laws requiring health insurance coverage of autism treatment (including ABA). These legislative efforts have largely been a result of partnerships between the Autism Speaks national advocacy organization and state-based advocacy groups. To date, 44 U.S. states (plus the District of Columbia and the U.S. Virgin Islands) have passed laws requiring new treatment coverage (Autism Speaks, 2016). Thus, the growth of new funding streams for ABA services in the autism area is likely responsible, in part, for the growth in the number of ABA practitioners.
Unlike other professions that are currently beyond their “developmental” period and are fully matured (e.g., medicine, law), behavior analysis is in the process of growth and evolution during which substantial infrastructure (e.g., university programs, laws, professional associations, practice guidelines) is being created and will undoubtedly continue to shape the future of the discipline. It is likely that within the next two decades, most of the discipline’s core structural needs will be in place and the steep growth trends currently being experienced will level out. Until then, however, behavior analysis will continue to grow and develop. It is conservatively estimated that within one to two decades, there will be more than 100,000 credentialed behavior analysts (i.e., BCBAs and BCaBAs) and more than 200,000 credentialed behavior technicians (i.e., RBTs). Thus, as treatments based on ABA are increasingly recognized for their effectiveness, the primary workforce largely responsible for implementing them will be concurrently increasing in size.
U.S. State Licensure
Many professions in the United States regulate their practitioners through state licensure, which is likely the form of occupational regulation most familiar to the public. However, licensure of behavior analysts is a recent phenomenon; thus, the profession relied on certification programs as a mechanism for practitioner regulation for many years. As depicted in Figure 2, since 2009, 25 U.S. states have enacted laws to regulate the practice of ABA through licensure. The most common regulatory authority in these laws is an independent behavior analyst licensure board (Association of Professional Behavior Analysts, 2016). Twenty-five states currently provide a pathway to licensure for behavior analysts with a graduate degree (AL, AK, AZ, HI, KS, KY, LA, MD, MA, MO, MS, NV, NY, ND, OH, OK, OR, RI, SD, TN, UT, VA, VT, WA, WI) and 18 of those states provide a pathway to licensure for assistant behavior analysts with an undergraduate degree (AL, AK, KS, KY, LA, MA, MO, MS, ND, NV, NY, OK, OR, RI, TN, UT, VA, WA). The BACB’s standards constitute a pathway to licensure in 24 of these states. One benefit of linking licensure requirements to the BACB’s standards is a minimal fiscal impact on state governments, thus providing a cost-effective means of promoting consumer protection through regulation. In addition, reliance on BACB standards by licensure boards facilitates the mobility of practitioners across states (see Hall & Lunt, 2005). Finally, individuals who are both credentialed by the BACB and licensed within a state are subject to the often-coordinated actions of two professional disciplinary systems.
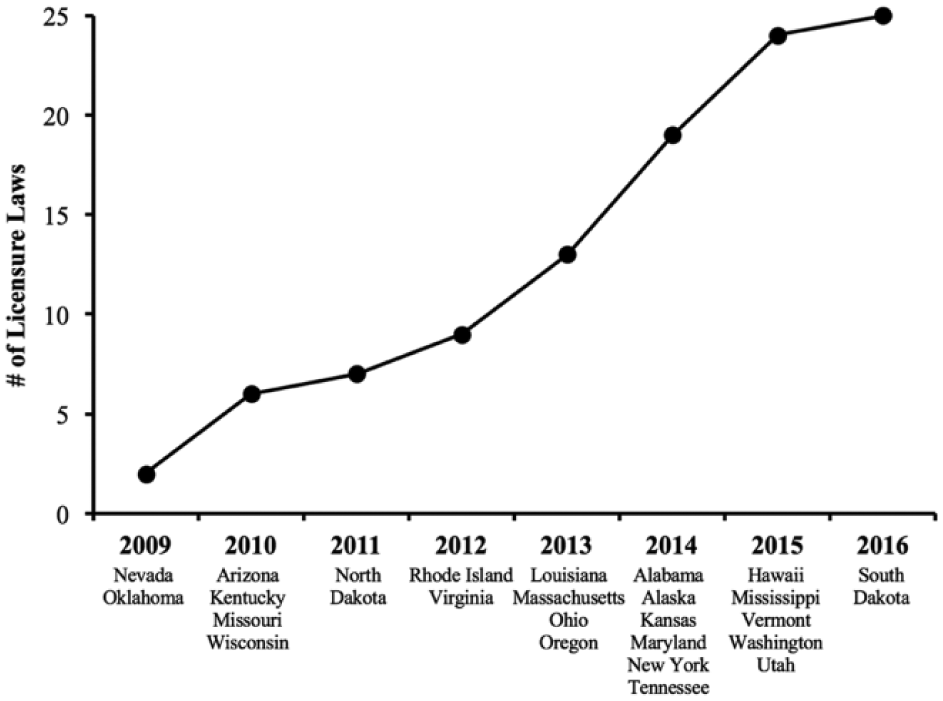
Cumulative number of U.S. licensure laws enacted through 2016 (N = 25).
The impetus for these licensure laws has been multifaceted. Some states pursued licensure as a form of additional regulation (in addition to BACB certification) of ABA practitioners who sometimes work with vulnerable populations. Other states pursued licensure along with bills to establish health insurance coverage of autism treatment because many insurance companies only reimburse licensed providers. The impact of licensure on the practice of behavior analysis has yet to be determined because most of these legislative activities have occurred in well under a decade and a number of other states are still pursuing licensure. However, the existence and growth of licensure is yet another indicator of the maturation of the profession of behavior analysis.
Conclusion
The past two decades have been a period of tremendous growth for ABA. This era has seen a significant increase in demand for services, the rapid expansion of university training programs, the development of a new global credentialing body (the BACB), behavior analyst licensure in half of U.S. states, and growth in the number of credentialed behavior analysts and behavior technicians, which now exceeds 50,000 in more than 70 countries. Of course, the maturation of a profession is not without its difficulties, and there is more work to be done. For example, behavior-analytic professional associations are in need of expansion and reconfiguration given the changing landscape of the discipline, and there is substantially more work to be done in the area of public policy. However, the recent developments in ABA, along with continued developments in basic behavior-analytic science and conceptual analysis, signify a healthy state of the parent discipline, behavior analysis.
The primary purpose of professional regulation is to protect the public by identifying members of a profession with defined training experiences and who have demonstrated competency (generally by examination). Because ABA-based treatments are increasingly being recognized and promoted in state and federal policy, it is important that appropriately credentialed workforces are linked to ABA treatment initiatives. As one example, ABA treatment of autism is covered by the health plan for U.S. military personnel (TRICARE, 2016), and BACB certificants are accepted as qualified service providers for the benefit. Due to the specialized nature of ABA treatments, it is important to consider appropriately credentialed ABA practitioners for related policy initiatives to maximize the likelihood that the positive outcomes reported in the scientific literature are achieved in typical practice environments (see Dixon et al., 2016).
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Both authors are employed by the Behavior Analyst Certification Board, one of the article’s primary topics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.