
Abstract
Idiopathic ventricular tachycardia (VT) is a rare form of arrhythmia in neonates that can be life-threatening prompting its timely diagnosis and importance of treatment to avoid serious complications, that is; heart failure. We describe a neonate with an incessant idiopathic ventricular tachycardia presented with heart failure and severe left ventricular dysfunction. This infant presented with poor feeding, irritability, increase work of breathing, and heartbeat of 260/min. The electrocardiogram (ECG) showed wide complex tachycardia and the echocardiogram showed a structurally normal heart with dilated cardiomyopathy. The clinical signs and chest X-ray changes were consistent with cardiac failure but preserved peripheral perfusion. This presentation, the sustained VT and the global cardiac failure makes the treatment challenging; therefore, early diagnosis of incessant VT in neonate is important for better prognosis.
Introduction
Arrhythmias in neonatal population is an uncommon clinical entity and may occur in neonates with a normal heart or in those with structural heart disease. The incidence of neonatal arrhythmia is reported to be 1% to 5% in all neonates. Ventricular arrhythmias in the neonate are classified as either benign or nonbenign. 1 Neonatal ventricular tachycardia can be idiopathic or can occur in the setting of congenital heart disease, cardiac tumors metabolic disturbance, myocarditis, cardiomyopathy, myocardial infarction, or channelopathies. 2 Idiopathic ventricular tachycardia refers to a clinical entity observed in children and adults, in whom conventional diagnostic evaluation fails to detect any cause.3 -5 Incessant ventricular tachycardia (VT) is defined as multiple episodes of VT within a 24 hour period, despite attempts to terminate the arrhythmia. 6 Idiopathic VT is extremely rare in neonates, features indicating a higher risk or underlying pathology may include polymorphic rather than monomorphic VT and the presence of symptoms or cardiomyopathy. The prognosis in the absence of underlying pathology or symptoms usually is good, but idiopathic VT can be refractory, and sudden death has been reported. A better prognosis for infants than for older children has been reported.7 -11 In past, several reports of ventricular tachycardia in children with structurally normal heart suggest that this disease follows a benign, self-limited course.12,13 Guidelines for treatment of such patients are far from being established; it was advocated that therapy could be withheld in most patients. However, there is paucity of data for management of young patients with incessant ventricular tachycardia presented late with heart failure.
Case Report
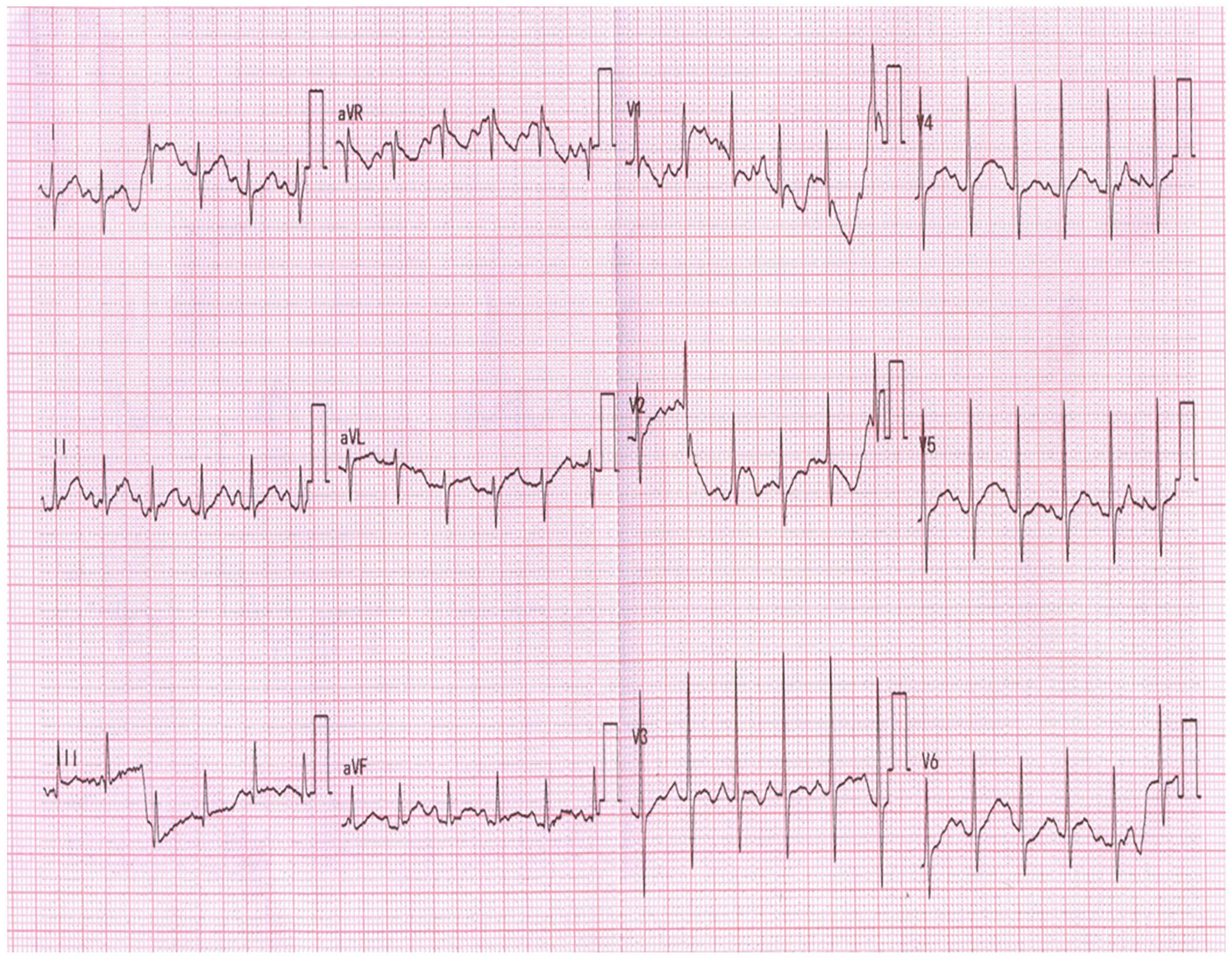
A 4 weeks-old infant presented to our hospital with a 2-week history of poor feeding, irritability and increase work of breathing. He was managed initially as bronchiolitis/pneumonia with nebulization’s and oral antibiotics at a remote primary care facility. Because of clinical deterioration and persistent tachycardia, he was referred to tertiary care hospital for further evaluation. Child presented with heart rate of 260/min, respiratory rate 63 /min and blood pressures 73/45 (60) mmHg and his weight was 3.3 kg. On examination, he had normal radial and femoral pulses with borderline delayed perfusion and mild sub costal recessions .Liver was palpable 2 cm below right costal margin. Upon admission, he was treated as supra ventricular tachycardia (SVT) with multiple boluses of adenosine, with no change in his tachycardia. Subsequently, DC cardioversion was attempted but failed to restore sinus rhythm. Pediatric electrophysiologist was consulted after getting ECG that showed monomorphic wide complex tachycardia (QRSd 88 m/s) of LBBB morphology and inferior axis with ventriculoatrial dissociation with capture and fusion beats (Figure 1). The clinical signs and chest X-ray changes were consistent with cardiac failure but preserved peripheral perfusion. Transthoracic echocardiogram showed structurally normal heart with severe left ventricular dysfunction (LVEF 21%) assessed on M Mode shown in Figure 2. Given the sustained VT and the global cardiac failure, the patient was slowly loaded with IV amiodarone (2.5 mg/kg over 1 hour) twice. After second bolus of amiodarone, rate control was achieved, with decrease in heart rate to 160 to 170/min. No electrolyte or metabolic disturbances were found. Viral panel for myocarditis was negative. He was started on amiodarone infusion at 10 µg/kg/min to achieve rhythm control along with anti-failure medications. Echocardiogram repeated after 48 hours showed some improvement in ventricular functions (LVEF 32%). The patient improved clinically after 48 hours with no signs of heart failure. His amiodarone was switched from IV to oral after 72 hours. The QTc interval remain with in normal limits. The patient was discharged on oral amiodarone (8 mg/kg/day) and anti-failure medications after 10 days of admission with a plan to adjust his medications on follow up. At discharge, he remained in accelerated ventricular rhythm at 140/min. On follow up, after 10 days of discharge, the ECG showed sinus rhythm at 140/min (Figure 3).

12 leads ECG showed monomorphic wide complex tachycardia with VA dissociation and capture beats.

Echocardiographic M Mode showing severe left ventricular dysfunction (LVEF 21%).
Electrocardiogram depicting sinus rhythm.
Echocardiogram repeated on follow up depict normal left ventricle systolic functions (LVEF 60%) shown in Figure 4. Holter monitoring done showed occasional isolated monomorphic PVCs and no runs of ventricular tachycardia.

Echocardiographic M Mode showing normal left ventricle systolic functions (LVEF 60%) on follow up.
Discussion
Idiopathic ventricular tachycardia in the presence of an apparently normal heart is observed rarely in children. Consensus guidelines on how to manage these children are still lacking. This case report depicts that ventricular tachycardia in infants can be misdiagnosed as supra ventricular tachycardia. This highlights the importance of using age-appropriate ECG parameters when evaluating pediatric patients. Moreover, unnoticed sustained ventricular tachycardia can be life threating if associated with tachycardia induce cardiomyopathy. Davis et al reported a 15% mortality in their cohort of 20 patients who presented late with heart failure. 12
In general, the pediatric reports to date suggest a favorable prognosis for idiopathic ventricular tachycardia infants. Pfammatter and Paul concluded that idiopathic ventricular tachycardia carries a favorable prognosis with no mortality reported. However, they reported 36% of patient presented with clinical symptoms or echocardiographic signs of left ventricular dysfunction, of which one-third (12% of the whole population) presented with severe symptoms (heart failure or syncope). Different single or 2 consecutive or concomitant medications were used for a subset of patients. However, there is no clarity on choice of antiarrhythmic medications for patients with severe left ventricular dysfunction.11,13 Levin et al reported 31 infants with ventricular tachycardia with complete resolution in all patients. They postulated that treatment is not necessary as there was no difference between children who received chronic outpatient anti-arrhythmic treatment and those who had no such therapy. 3 Similarly, Escudero et al reported that Idiopathic VT carries a good prognosis with or without treatment and has a high likelihood of spontaneous resolution by 1 to 2 years of age. 14 Davis et al concluded that Incessant VT greater than 80% of the day may be associated with tachycardia-induced cardiomyopathy. 12 Our patient also presented with tachycardia induced cardiomyopathy (TIC). We postulated that infants with ventricular tachycardia in resource limited countries are at high risk of developing TIC because of delayed diagnosis secondary to unavailability of monitoring and health resources. This report highlights the natural history of incessant idiopathic ventricular tachycardia in infants if goes unnoticed and the importance of early diagnosis and management to reduce the risk of tachycardia induce cardiomyopathy and heart failure.
In low-income countries, the approach to ventricular tachycardia (VT) in infancy requires careful prioritization of diagnostic and management strategies due to limited resources. 4 A detailed history remains crucial, particularly for identifying any family history of genetic disorders or sudden cardiac death, which may suggest inherited arrhythmias. In cases whereby long QT syndrome or Brugada syndrome are suspected, parental ECG’s can be great sources of evidence. Basic laboratory tests to rule out electrolyte imbalances, such as potassium, magnesium, or calcium disturbances, should be done as they are cost-effective and widely available. Echocardiography is an important diagnostic tool for detecting structural heart diseases, such as congenital defects or cardiomyopathies, and is often more accessible than advanced imaging modalities. Holter monitoring, if available, can help assess the burden of arrhythmia and treatment efficacy, however, intermittent ECG monitoring may be used as an alternative in resource-constrained settings. For suspected infective causes like myocarditis, cost-effective tests such as markers of inflammation (eg, C-reactive protein) and cardiac biomarkers (eg, troponins) are essential, while viral serology or PCR testing may be limited to specific cases. Cardiac MRI, although ideal for detecting myocarditis, tumors, or arrhythmogenic cardiomyopathies, is often unavailable or prohibitively expensive and may be reserved for persistent or refractory cases when other methods fail to provide answers.13,15,16 In our setting, we used above mentioned approaches to rule out structural and infective causes of VT in infancy except for the MRI due to the un availability of this modality. This resource-sensitive approach ensures that available diagnostics are used efficiently to provide the best possible care for infants with VT in low-income settings.
Amiodarone is a potent antiarrhythmic agent primarily used to treat and manage life threatening arrhythmias. However, because of risk of cardiovascular collapse in children extreme caution and careful hemodynamic monitoring is recommended while using intravenous amiodarone. 17 Once the arrhythmia is controlled, patient may be transitioned to oral therapy for long term management. This transition requires careful dosing and monitoring due to pharmacokinetics of amiodarone including its long half life, high tissue binding and potential for accumulation. Due to rarity of neonatal ventricular tachycardia, no consensus available for duration of treatment and is depends on underlying cause, severity of arrhythmia, and response to treatment. We decided to use amiodarone as our patient was in incessant ventricular tachycardia and had severe ventricular dysfunction. There are concerns of using amiodarone in infants because of risk of cardiovascular collapse.17,18 Amiodarone is the only IV antiarrhythmic medication available for use in acute situation in most developing countries. However, large boluses of amiodarone should be avoided to achieve rhythm control rather slow amiodarone infusion is a better option for rate control in acute setting to avoid hemodynamic compromise in young patients.
Conclusion
Ventricular tachycardia in young population is rare with overall good prognosis. However, it can be life threating if it remains unnoticed and undiagnosed for longer period. The risk is substantially high in resource limited countries because of paucity of health facilities and personnel who can diagnose it. Moreover, the choice of medications is limited for management in acute situations.
Footnotes
Acknowledgements
The authors wish to acknowledge the support of the staff members of the Clinical Research Department of the National Institute of Cardiovascular Diseases (NICVD) Karachi, Pakistan.
Authors’ Contributions
RS, ASS, MM contributed to the concept and design of study, RS, ASS, MM, contributed to the analysis and interpretation of data, RS, and MM collected data and drafted the manuscript, and ASS, and MM critically analyzed for content. All author approved the final draft to the manuscript.
Data Availability Statement
Data will be provided on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the ethical review committee of the National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan with IRB-No. 39/2024. Written informed consent was taken from the parents.
Informed Consent/Patient Consent
Written informed consent was taken from the parents of the patient who are legally authorized representative of the minor subject for the publication of this study.