
Abstract
Objective. To determine clinical presentations and laboratory findings of meningitis outbreak among children in 2023 in Iraq. Method. the demographic data (gender, age, symptoms, and disease transmission among family members) were collected from child patients, who were admitted to Halabja and Sulaimania pediatric teaching hospital in the period of 15 March 2023 to 1st of August, 2023. The blood and cerebrospinal fluid (CSF) specimens were collected for hematological, biochemical, microscopic, and microbiological examinations, including culturing and FilmArray meningitis/encephalitis panel. Results. The population studied were 170 children between 1 and 18 years old, Males were 110 (64.7%), and females were 60 (35.3%). Children between 5 and 10 years old had the highest frequency, whereas only 2 children were <1 year. Clinical symptoms were fever in 100%, followed by headache, vomiting, convulsion, photophobia, and lethargy (79%, 12%, 3%, 3%, 2%) respectively. CSF parameters were: 38.8% of them had >1000 leucocytes/µ, followed by 31.2% for those who had <300 cells/µ, differential CSF leucocytes, 82.4% were monocytes, and sugar was normal at 84.1%. while protein was <40 mg/d in 55.9% of them. Conclusion. Meningitis outbreak due to enterovirus was recorded, and age predilection and clinical presentation refer to different serotypes. Further work is needed to define the species and serotypes of the virus and define the environmental source of the virus.
Introduction
Meningitis is an inflammation of the meninges of the brain and spinal cord, it causes CSF pleocytosis. 1 The etiology of the disease is bacteria, viruses, fungi, parasites, and sometimes immunological disorders. 2 These etiologic agents differ in their clinical presentation and severity, with different age predilections. The disorder has a huge clinical burden, with high morbidity and mortality in children. 3 The mortality and morbidity differ according to the agent, and age of the child, sometimes the victim’s morbidity may reach >50%, and 100% of affected children lose their lives. 4 The incidence of bacterial meningitis in Iraq is estimated to be around 1.47 cases/100 000 population, 5 Owing to this, it is a serious public health problem that necessitates a high index of suspicion as well as rapid comprehension and management of the condition. 4
Importantly, worldwide implementation of intrapartum antibiotic prophylaxis, 6 universal vaccination programs against Hemophilus influenza, 7 streptococcus pneumonia, 8 and Neisseria meningitis 9 led to a dramatic fall in bacterial meningitis, most meningitis cases are aseptic meningitis, and viruses are the most common cause of aseptic meningitis. 6
Aseptic meningitis is differentiated from bacterial meningitis by negative cerebrospinal fluid (CSF) bacterial cultures. This condition is typically diagnosed based on CSF pleocytosis, indicated by an elevated white blood cell (WBC) count of more than 5 cells/mm³.10,11 Viral meningitis is widely spread, and sometimes occurs in epidemics 2 it has diverse clinical presentations. It can be brought on by a variety of viruses, such as the parechovirus, herpes virus, respiratory virus (adenovirus, influenza virus, coronavirus, measles), enterovirus (EV), mumps, rotavirus, lymphocytic choriomeningitis virus, human immunodeficiency virus, and parvovirus B19. Again, the introduction of the measles, mumps, and rubella (MMR) vaccine, 12 makes the enterovirus the most common viral pathogen, 13 followed by herpes simplex virus, and varicella zoster viruses subsequently. 14 These agents cause diverse clinical symptoms, ranging from non-specific symptoms to neurological symptoms, in addition to testing cerebrospinal fluid (CSF) culture, polymerase chain reaction (PCR), and serological methods these cases are diagnosed as meningitis. 15 Affected Child may improve and only may need supportive treatment, on the other hand, it may leave adverse neurologic consequences and complications, 14 additionally, the cost of treating aseptic meningitis remains high despite advancements in diagnostic capabilities, so viral meningitis has a huge burden on health settings. 16
Recently, there was an outbreak of meningitis in Iraq. The World Health Organization declared that there was a surge in cases of meningitis in the Halabja and Sulaimania governorates. 17 To guide clinical treatment and determine the top areas for future study, it is crucial to define the patterns of the diseases. The objective of this study was to clarify the epidemiological, clinical, and agent identification of the outbreak among children with meningitis who were being treated in hospitals.
Patients and Method
The present prospective descriptive study was carried out in the Sulaimania and Halabja Governorates in the Kurdistan region of Iraq in a 4.5-month duration, From 15th March to 1st August/2023, during the outbreaks of meningitis among children. The population study included all children diagnosed with meningitis between 1 month and 18 years in Dr. Jamal Ahmed Rashed Pediatric Teaching Hospital and Halabja maternity and pediatric teaching hospitals (excluding the neonatal age group and adults). All patients confirmed with CSF test (CSF culture and PCR), after obtaining consent from parents, and an ethically approved predesigned questionnaire was used to retrieve information on patients’ records which included; demographic data (Age, sex, residency, previous admission, history of contact, and previous use of antibiotic, etc.), clinical presentation including (fever, headache, vomiting, convulsion, photophobia, lethargy, and diarrhea), meningeal sign.
CSF samples from all the participants were collected through lumbar puncture prior to receiving medications, then analyzed by laboratory personnel of the 2 aforementioned specialized hospitals. The analysis included appearance evaluation, total and differential cell counts, glucose and protein level determination, culturing, and direct microscopy of CSF to detect bacterial or fungal pathogens. In addition to, BioFire® FilmArray® Meningitis/Encephalitis Panel.
The cases were confirmed with CSF examinations (CSF culture and PCR), 18 The microbiological methods used to confirm the cases were: Manual CSF culture for all cases in accordance with WHO guidelines. 19 The types of culture media employed encompassed blood, chocolate and MacConkey, agars.
BioFire® FilmArray® Meningitis/Encephalitis Panel was used for the simultaneous detection and identification of various viral, bacterial, and fungal nucleic acids directly from cerebrospinal fluid samples obtained from 90 individuals exhibiting signs or symptoms of meningitis. The Panel menu comprises the following microorganisms: Bacteria: Escherichia coli K1, Listeria monocytogenes, Haemophilus influenza, Streptococcus agalactiae, Neisseria meningitidis, Streptococcus pneumoniae; Viruses: Enterovirus Cytomegalovirus (CMV), Herpes simplex virus 2 (HSV-2), Herpes simplex virus 1 (HSV-1), Human par echovirus, Human herpesvirus 6 (HHV-6), Varicella zoster virus (VZV); Fungus: Cryptococcus neoformans/gattii.
Additionally, blood tests like complete blood count, taken for all participants
Statistical Analysis
The data was coded and added to a Microsoft Excel spreadsheet, and IBM-SPSS software version 22 was used for data analysis. Categorical variables were expressed via frequencies and percentages.
Ethical Approval and Informed Consent
The study has approval from ethical committee at Dr. Jamal Ahmed Rashed Pediatric Teaching Hospital, with proof number 50-2023/7, in addition, all parents or legally authorized representatives provided written informed consent prior to enrolment in the study.
Results
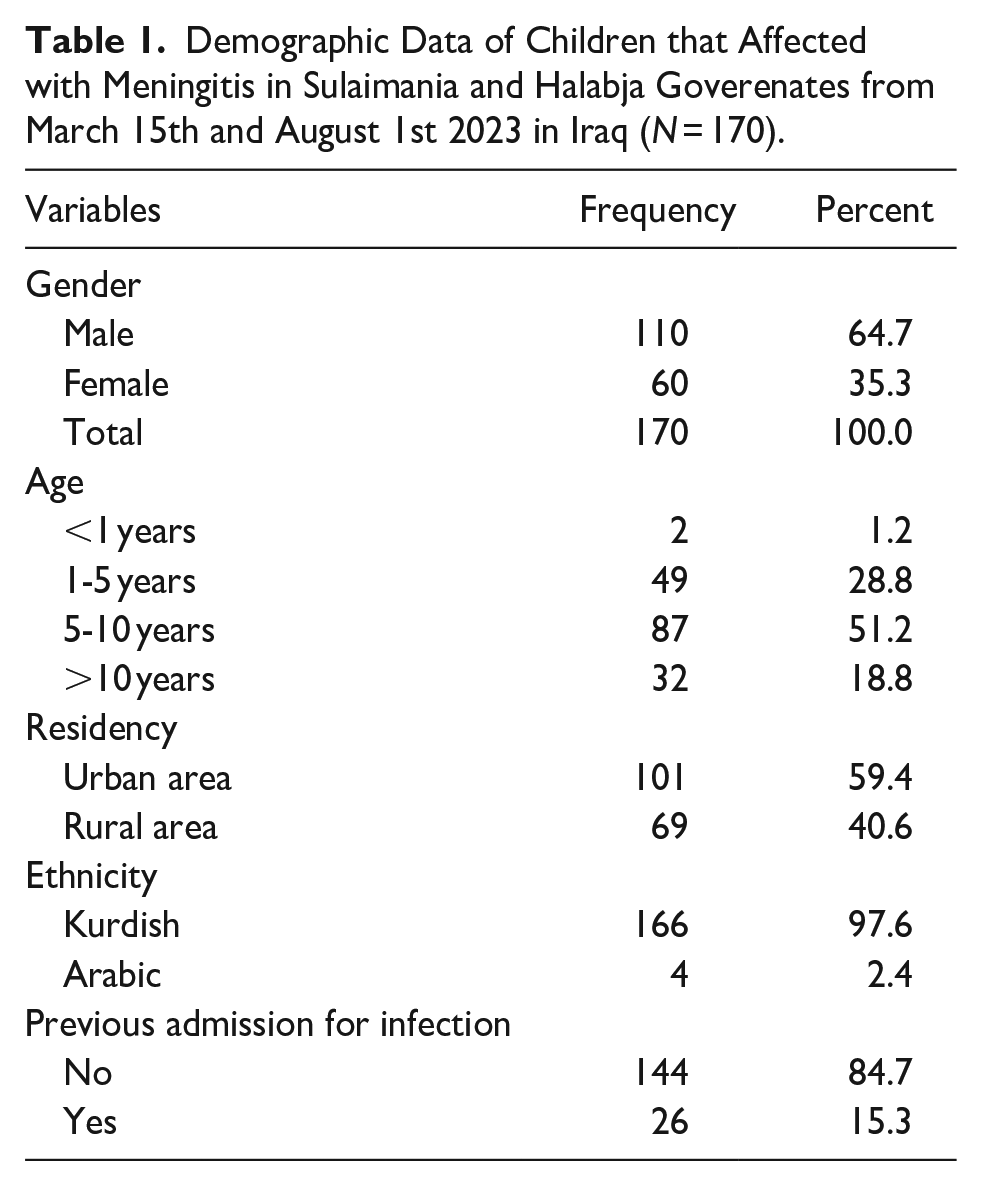
During 4.5 months, there were 170 children diagnosed with meningitis and admitted to the hospitals. Males were 110 (64.7%), and females were 60 (35.3%). Children between 5 and 10 years had the highest frequency, whereas only 2 children were below 1 year (Figure 1). The residency of the affected children, mostly from urban areas 59.4%, followed by those who came from rural areas 40.6%. Regarding ethnicity, 97.6% were Kurdish, while 2.4% were Arabic (Table 1).

The chart shows affected pediatric age groups during the meningitis outbreak in Sulaimania and Halabja governments from March 15th and August 1st, 2023, in Iraq (N = 170).
Demographic Data of Children that Affected with Meningitis in Sulaimania and Halabja Goverenates from March 15th and August 1st 2023 in Iraq (N = 170).
the most common Clinical symptoms were fever in 100%, followed by headache, vomiting, convulsion, photophobia, and lethargy (79%, 12%, 3%, 3%, 2%) respectively (Figure 2). Moreover, 61.8% of children had signs of meningeal irritation. The majority of the patients (67.1%) received antibiotics before a diagnosis of meningitis (Table 2).

The chart shows clinical signs and symptoms of children affected with meningitis in Sulaimania and Halabja governments from March 15th and August 1st, 2023 in Iraq (N = 170).
Distribution of Symptoms Among Children with Meningitis in Sulaimanya and Halabja Governorates, Iraq, Between March 15th and August 1st 2023 (N = 170).

Abbreviation: AB, antibiotics.
The laboratory findings of the children: white blood cell count (WBC) in >half of patients were between 10 000 and 20 000. For CSF leucocytes, 38.8% of the patients had >1000 cells/µL, followed by 31.2% for those who had <300 cells/µL, and 30% had 300 to 1000 cells/µL. After the Differentiation of leucocytes, 82.4% were monocytes, and 17.6% were polymorph nuclear cells. The CSF sugar, was mostly between 40 and 100 mg/d (84.1%), while those <40 mg/d were 14.1%. The greatest percentage of children (55.9%), had CSF protein <40 mg/d, while 44.1% of them was >40 mg/d. The CSF culture in 157 patients (92.4%) were negative, and only 3.5% and 4.1% had streptococcus pneumonia and S. paucimobilus subsequently (Table 3). In addition, Enteroviruses were detected in 85 cases, means (94.4%) of tested populations, while no pathogen was detected in 5 patients (5.6%). Importantly, all cases improved and discharged well without any sequelae.
Laboratory Findings of Children that Affected with Meningitis in Sulaimania and Halabja Goverenates from March 15th and August 1st 2023 in Iraq (N = 170).

Abbreviations: CSF, cerebrospinal fluid; MNC, mononuclear cell; PMN, polymorphous nuclear cells; ↔, normal; ↑, elevated.
Discussion
This study was conducted on 170 children with meningitis in Sulaimani and Halabja governorates in the Kurdistan region of Iraq. The main finding in this study is that, the outbreak was due to enteroviruses, this is contrasts with the study of Al-Sanouri in Iraq in 2021, which found meningococcal meningitides was the responsible pathogen. 20 The current study found that males were predominant, with a ratio of male to female 2:1, this corresponds with other studies with a ratio of 2:1 1 the exact causes of high male/female ratio are poorly understood, but the effect of sex hormones on the T-helper 1/T-helper 2 cytokine balance has been proposed to explain it. 17 The current study found the highest rate was among the primary school age (5_10-year-old) which accounted for 51%. This outcome is contrasts with studies done in Iran, and Egypt, who found child <6 years and, <4 years old were the most affected age groups subsequently.21,22 This difference may be explained by the difference in causative agent, individual susceptibility, and, coverage of vaccination. The residency of the affected children, was mostly from urban areas 59.4%, followed by those who came from rural areas 40.6% similar to the study of Giannakopoulos Ioannis, et al in Greece. 23 Regarding ethnicity, 97.6% were Kurdish, while 2.4% were Arabic as the original population of Kurdish ethnicity with some others living in this region.
The most common Clinical symptoms were fever in 100%, followed by headache, vomiting, convulsion, photophobia, and lethargy respectively similar to studies done in Jordan and Tehran, 24 Although, there is a difference in the incidence of seizure, it is low in our study compared to other like Chamkhaleh et al. that was 2nd most common symptom after fever. 25 Simillarly, Anahita et al. reported convulsion in 20% of the cases. 21
In our study, most of the children had signs of meningeal irritation at the time of presentation (neck stiffness, Kerning sign), this is much higher if compared to other studies, 25 this difference may have been related to the onset, time of presentation and involvement of posterior meninges, so in the absence of typical features in children we should not miss the diagnosis of meningitis, so early performing lumbar puncture lead to a diagnosis of meningitis as soon as possible. Importantly, The majority of the patients received antibiotics before a diagnosis of meningitis, although the results differ from some published studies Alizadeh 2021, 25 but consistent with that from Rogers 2019, 26 this is related to health state and strict antibiotic stewardship program.
In the current study, white blood cell count (WBC) in most patients was between 10 000 and 20 000, which differs from the study of Nguyen-Huu et al., 27 In which about 2 of 3 cases with meningitis had decreased WBC, so peripheral blood leukocyte count is not a reliable marker to predict meningitis in pediatric age group.
During an epidemic of meningitis as we have a shortage of PCR and blood culture we depend on CSF parameters to differentiate bacteria from viruses. In bacterial meningitis, there is CSF pleocytosis, usually with a leucocyte count greater than 1000 cells/mm3 and a predominance of polymorphonuclear leukocytes. In some cases, especially when performed early in the disease, the CSF leucocyte count could be normal. 28 In this study, the CSF leucocyte in most of the patients <1000 cells/µL, and after Differentiation of CSF leucocytes, the majority were lymphocytes, and only 17.6% were polymorph nuclear cells, like in viral meningitis.
The current study found that CSF sugar was mostly between 40 and 100 mg/dL, which contrasts with that of Vietnam in 2022. 27 Furthermore, the percentage of children who had CSF protein >40 mg/dL. Only 44.1%, while 97% of the patients had high protein in the study of Chau Duc Nguyen-Huu (2022). in Vietnam. 27 In bacterial meningitis, the biochemical examination demonstrates a decreased glucose concentration (<40 mg/dL), unlike proteins, which is high (usually >100 mg/dL), in contrast to viral meningitis no significant change in the levels of glucose and protein may be normal to slightly increased. 29
Importantly, the CSF culture of the majority of the patients was negative, only in 3.5% there was a growth of streptococcus pneumonia. This result is lower in comparison with other study, where CSF culture was positive in 24.2% of patients. 27
The current study shows that the outbreak of meningitis is viral, although, some cases are bacterial meningitis and it’s difficult to differentiate on the base of clinical presentation and CSF pleocytosis.
This study set out to gain a better understanding of the recent outbreak of meningitis in Sulaimania and Halabja governorates in the Kurdistan region of Iraq. The most obvious finding to emerge from this study is that the clinical presentation and investigations, as well as the favorable outcome of the cases point to that the outbreak is mostly aseptic meningitis and enterovirus was the responsible pathogen even among those which we couldn’t perform the PCR test. Although, sporadic cases of bacterial meningitis were recorded. In addition, this study found that the highest risk group was children 5 to 10 years old. Importantly, there was no history of such an outbreak in these 2 governorates, and even there was no enterovirus outbreak in Iraq and neighboring countries at that time, so the occurrence of this outbreak was unusual and the source unidentified. These findings enhance our understanding of the new outbreak of meningitis cases in these 2 goverenates of Iraq, and this can help to build up strategic plans to prevent further outbreaks in future in Iraq.
The limitations of this study are: the calculation and justification of sample size were not selected, and the questionnaire used has no validity and is not pilot-tested. Furthermore, the way to find the responsible pathogens like the culture method, which was manual instead of using VITEK 2 and, doing PCR or film array for all cases to find the responsible pathogen. Additinally, the serotypes and species of the virus are still not detected, and this demands future work. The key strength of the present study was that the culturing process was done according to WHO guidelines. Importantly, this is the first study that documents the current meningitis outbreak among children in Iraq.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241293948 – Supplemental material for Outbreak of Meningitis in Iraq in 2023
Supplemental material, sj-docx-1-gph-10.1177_2333794X241293948 for Outbreak of Meningitis in Iraq in 2023 by Khalid Hama Salih, Zana Baqi Najmadden, Bahadin Qader Ahmed, Pishdar Abdullah Ismael, Kaiwan H. Kareem, Lana Diyar Abdulqadir, Roza M. Sabir, Basta J. Abdalla, Binay A. Qadir, Razhan M. Mohammed and Ali Salih karim in Global Pediatric Health
Footnotes
Acknowledgements
The authors thank the general directorate of Halabja Health Governorate, the manager of Jamal Ahmad Rashid Hospital, as well as all medical and laboratory staff of Halabja Pediatric and Maternity Teaching Hospital and Jamal Ahmad Rashid Hospital for their kind efforts and cooperation during the outbreak.
Author Contributions
Khalid Hama Salih: Supervision, writing, analysis, revising, final approval
Zana Baqi Najmadden: supervision, data collection, writing, revising, interpretation, final approval
Bahadin Qader Ahmed: data collection, interpretation, final approval
Pishdar Abdullah Ismael: data collection, revising
Kaiwan H. Kareem: data collection
Lana Diyar Abdulqadir: data collection
Roza M. Sabir: data collection
Basta J. Abdalla: data collection
Binay A. Qadir: data collection
Razhan M. Mohammed: data collection
Ali Salih Karim: data collection
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Committee
The study has approval from the ethical committee at Dr. Jamal Ahmed Rashed Pediatric Teaching Hospital, with proof number 50-2023/7
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.