
Abstract
Objective
The American Heart Association (AHA) launched the 2022 guidelines for the diagnosis of hypertension (HT) by ambulatory blood pressure monitoring (ABPM). The present study aimed to evaluate the impacts of the 2022 AHA guidelines on the changes in the prevalence and phenotype of HT in children suspected of HT.
Methods
Consecutive 100 children aged 6 to 20 suspected of HT who underwent 24-hour ABPM were recruited. The patients were separated into 3 groups: escalated, de-escalated, and unchanged. Demographic data were compared between the 3 groups. Logistic regression analysis was performed to evaluate the factors associated with the escalation in the diagnosis of HT.
Results
The present study revealed that the prevalence of HT, including sustained and masked HT, increased from 48% by the 2014 AHA guidelines to 65% by the 2022 AHA guidelines. Patients in the escalated group tended to have a higher proportion of male gender, with an older age and a taller height compared to those in the de-escalated group. Multivariate analysis showed that height was the only factor associated with the escalation in the diagnosis of HT [OR 1.09 (1.01-1.19), P-value .04]. Five out of 6 (83.3%) patients in the escalated group with available echocardiographic results had left ventricular hypertrophy (LVH).
Conclusion
Using the 2022 AHA guidelines resulted in more detection of patients with HT, and almost 30% of the escalated group had LVH. This finding supports using the 2022 AHA guidelines to detect children at risk of developing cardiovascular diseases early.
Keywords
Introduction
The global prevalence of pediatric hypertension (HT) has been increasing. 1 In Thailand, the prevalence of HT was reported to be 2.6% in children and 9.4% in adolescents.2,3 Several studies have shown that pediatric HT increases the likelihood of acquiring cardiovascular diseases later in life. As a result, early detection and treatment of childhood HT would contribute to lowering the risk of adult cardiovascular diseases.4 -8
The American Academy of Pediatrics (AAP) clinical practice guidelines recommended that ambulatory blood pressure monitoring (ABPM) be used to confirm sustained HT in pediatric patients suspected of HT due to persistently high office blood pressure. 5 For the diagnosis of HT by ABPM, the 2014 American Heart Association (AHA) pediatric guidelines recommended using the 95th percentile criteria for gender and height. 9 In 2017, the American Academy of Pediatrics modified the HT cut-off for office blood pressure (BP) measurement to be 130/80 mmHg for all pediatric patients ages 13 years and older as same as the HT cut-off for office BP measurement in adults ages 18 years and older recommended by the 2017 AHA adult guidelines.5,10 Correspondingly, the 2022 pediatric AHA guidelines recommended the HT cut-off for ABPM in children ages 13 years and older as the HT cut-off for ABPM in adults ages 18 years and older. Still, the 95th percentile criteria remained for children ages 12 and younger. Additionally, BP loads from the previous 2014 AHA guidelines were eliminated, and the classifications of HT phenotypes were simplified. The new 2022 AHA guidelines were thought to be more predictive of target organ damage such as left ventricular hypertrophy (LVH), an independent risk factor for cardiovascular morbidity in adults, and more sensitive to HT diagnosis in most studies.11 -16 On the contrary, a study in children with chronic kidney disease showed the opposite result: the 2014 AHA guidelines slightly better discrimination of LVH. 15 To our knowledge, no study has compared the effect of changes in the classification of HT by the new 2022 AHA guidelines in pediatric Southeast Asian populations. The present study aimed to evaluate the impact of the 2022 AHA guidelines on the changes in the prevalence and phenotype of HT in children suspected of HT.
Materials and Methods
Participating Patients
This retrospective study enrolled consecutive pediatric and adolescent patients aged 6 to 20 years referred to the pediatric HT clinic at Ramathibodi Hospital due to high office BP on 3 occasions or clinical suspicion of HT. The study was approved by the Ethics Committee for Human Research of the Faculty of Medicine Ramathibodi Hospital (MURA 2020/1792). The study was granted exemption from informed consent due to its retrospective design. Some patients in the present study were included in the previous study examining the performance of waist circumference to height ratio to predict sustained HT. 17
All pediatric patients who underwent ABPM for 24 hours to confirm the diagnosis of HT were included. Patients were separated into 3 groups: escalated, de-escalated, and unchanged. The escalated group included patients with normotension, pre-HT, or unclassified diagnosis by the 2014 AHA guidelines but were escalated into masked HT or sustained HT by the 2022 AHA guidelines. The de-escalated group included patients with pre-HT or unclassified diagnoses by the 2014 AHA guidelines but were de-escalated into normotension or white-coat HT by the 2022 AHA guidelines. The unchanged group included patients who had the same diagnosis from both guidelines.
Baseline characteristics, anthropometric data, office BP, and ABPM results were collected. Body mass index (BMI) was calculated using the following formula: Weight (kg)/height (m). 2 BMI was adjusted to BMI z-score using the World Health Organization Anthroplus software, which is the growth reference data for children and adolescents ages 5 to 19 years. 18 Left ventricular hypertrophy (LVH) was evaluated using an echocardiographic study by an experienced pediatric cardiologist. LVH was defined as left ventricular mass index (LVMI) > 51 g/m27 or LVMI is >115 g/body surface area (BSA) in males and >95 g/BSA in females. 5
Blood Pressure Measurement
Office BP was measured twice in the right arm in a seated position with an oscillometric device, using standard BP measurement practice and appropriate cuff size. A BP value for each occasion was determined by taking the average of the 2 BP readings. According to current pediatric guidelines, high office BP is defined as a systolic blood pressure (SBP) or a diastolic blood pressure (DBP) ≥95th percentile for gender, age, and height in children aged < 13 years or 130/80 mmHg in children aged ≥ 13 years over the 3 occasions. 5 Mean office BP was an average of the BP values from 3 occasions, whereas maximum BP was the highest among the 3 values. Office BP parameters were converted to BP indices using the following formula: BP value/BP cut-off value for high BP for each patient. BP indices were used to compare BP parameters among patients of different ages, genders, and heights.
ABPM was performed using a TM-2430 (A&D, Japan) device, which has been validated for use in pediatric patients. 19 The qualified healthcare provider placed an appropriate cuff on each patient’s non-dominant arm. The device was programmed to measure BP every 20 minutes while awake and every 30 minutes while sleeping for 24 hours. Patients were advised to go through their daily routines, avoid strenuous activities, and record their activities, including their sleep and awake periods. ABPM data were considered valid in each patient if there were ≥40 valid BP readings over 24 hours. Definitions of ABPM HT phenotypes by 2014 AHA guidelines and 2022 AHA guidelines are presented in Table 1.
AHA 2014 and AHA 2022 Hypertension Phenotypes.

Abbreviations: BP, blood pressure; HT, hypertension; P90th, 90th percentile; P95th, 95th percentile.
ABPM P95th or the adult cut-off.
Adult cut-off: 24 hours, 125/75 mmHg; awake, 130/80 mmHg; sleep, 110/65 mmHg.
Statistical Analysis
Statistical analysis was performed using IBM SPSS® Software, Version 26. The distribution of each parameter was tested with the Kolmogorov-Smirnov test. Descriptive data were presented as number (percentage), mean ± standard deviation (SD), or median (interquartile range, IQR) as appropriate. Demographic data were compared among 3 groups. For comparative analysis, the chi-square test or Fisher’s exact test was used for categorical data, and the student t-test, ANOVA, or Mann–Whitney U-test was used for continuous data, as appropriate. According to different guidelines, the prevalence of ABPM phenotypes was compared using the McNemar test. Univariate logistic regression analysis was used to test the parameters associated with the escalated group compared to the non-escalated group. The parameters significantly associated with the escalated group from the univariate analysis were added to the multivariate logistic regression model. A P-value ≤.05 was defined as statistical significance.
Results
ABPM Phenotypes
Among 100 patients, abnormal ABPM results were detected in 48 and 65 children according to the 2014 and 2022 AHA guidelines, respectively. The prevalences of sustained HT, masked HT, and white-coat HT were increased when using the 2022 AHA guidelines compared to the 2014 AHA guidelines: 43% to 50% (p-value = .02), 5% to 15% (P < .01), and 12% to 27% (P < .01), respectively. Additionally, the prevalence of awake HT and nocturnal HT increased from 30% to 36% (P = .03) and 35% to 59% (P < .01), respectively (Table 2).
ABPM Phenotypes According to the 2014 and 2022 AHA Guidelines.

Abbreviation: HT, hypertension.
Bold texts indicate statistical significance.
Hypertension Classification
Patients were classified as escalated group, de-escalated group, and unchanged group according to changes in diagnosis by the 2014 and 2022 AHA guidelines (Table 3). Escalated group consisted of 17 individuals, which included patients who had previously been diagnosed with normotension (N = 1), pre-HT (N = 7), or unclassified (N = 9) according to the 2014 AHA guideline but who were escalated to have masked HT (N = 10) or sustained HT (N = 7) with the 2022 AHA guidelines.
Patient Classifications and ABPM Phenotypes.

Abbreviation: HT, hypertension.
Three patients with office BP and ABPM results in less than the 95th percentile and BP load less than 25% were previously diagnosed as having normotension or unclassified group. However, the ABPM results exceeded the cut-off of the 2022 AHA guidelines and were reclassified as having masked HT.
Fourteen patients with office BP greater than the 90th percentile, ABPM results were less than the 95th percentile, and BP loads greater than 25% were previously diagnosed with pre-HT or unclassified group. Still, they were reclassified as having masked or sustained HT by the ABPM results that exceeded the cut-off of the 2022 AHA guidelines.
The de-escalated group had 16 patients. In this group, the ABPM cut-off remained unchanged. All patients in this group had office BP over the 90th percentile, ABPM results were less than the 95th percentile, and BP loads were more than 25%. They were previously diagnosed as having pre-HT or unclassified group but were reclassified as having normotension or white coat HT because of the elimination of BP load from the 2022 guidelines.
When using the 2022 AHA guidelines, patients in the escalated group had higher proportions of awake systolic HT, nocturnal systolic and diastolic HT, and 24-hour systolic HT more than those in the de-escalated group. The awake DBP index, sleep SBP index, 24-h SBP, and DBP index using the 95th percentile reference from the 2014 AHA guidelines were different between groups (Table 4).
ABPM Values and Phenotypes According to Patient Classifications.

All data are presented as median (IQR).
Abbreviations: BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HT, hypertension; SHT, systolic hypertension; DHT, diastolic hypertension.
95th percentile reference from 2014 AHA guidelines.
Diagnosis by 2022 AHA guideline.
Bold texts indicate statistical significance.
Clinical Data
Patients in the escalated group had higher weight and height than the de-escalated and unchanged group, but the BMI z-score and the other anthropometries were not different (Table 5). In the subgroup analysis of patients ≥13 years old (N = 58), height was the only factor that differed between each group (escalated vs de-escalated vs unchanged group; 172, 160, and 166 cm, respectively; P = .04).
Patient Clinical Data.

All data presented as mean ± SD, otherwise indicated.
Abbreviations: WHtR, waist-to-height ratio; SBP, office systolic blood pressure; DBP, office diastolic blood pressure; LVH, left ventricular hypertrophy.
Median (IQR).
n = 72.
N = 36 includes 6, 3, and 27 patients in the escalated, de-escalated, and unchanged groups.
Bold texts indicate statistical significance.
Thirty-six patients underwent an echocardiography. Five out of 6 patients (83.3%) in the escalated group had left ventricular hypertrophy (LVH). One obese patient in the de-escalated group had LVH. Eleven out of 27 patients (40.7%) in the unchanged group had LVH, and all of them had either sustained or masked HT. When using the 2014 AHA guidelines, LVH was not statistically different between ABPM phenotypes (P = .15), with nine patients diagnosed with unclassified HT or pre-HT having LVH. On the contrary, using the AHA 2022 guidelines, different LVH diagnoses were found between each ABPM phenotype (P = .04). LVH was present in 11 out of 28 participants with sustained HT. All patients with masked HT (N = 5) also had LVH. Only 1 out of 3 patients with white coat HT had LVH.
Factor Associated With the Escalation in Diagnosis
Age, gender, height, and weight were the demographic data related to the escalation in diagnosis compared to the non-escalated group. After multivariate analysis, height was the only independent factor related to the escalation in the diagnosis of HT with an OR of 1.17 (1.02-1.34, P = .03) (Table 6).
Logistic Regression of the Escalated Group (N = 17) Compared to the Non-escalated Group (N = 67).
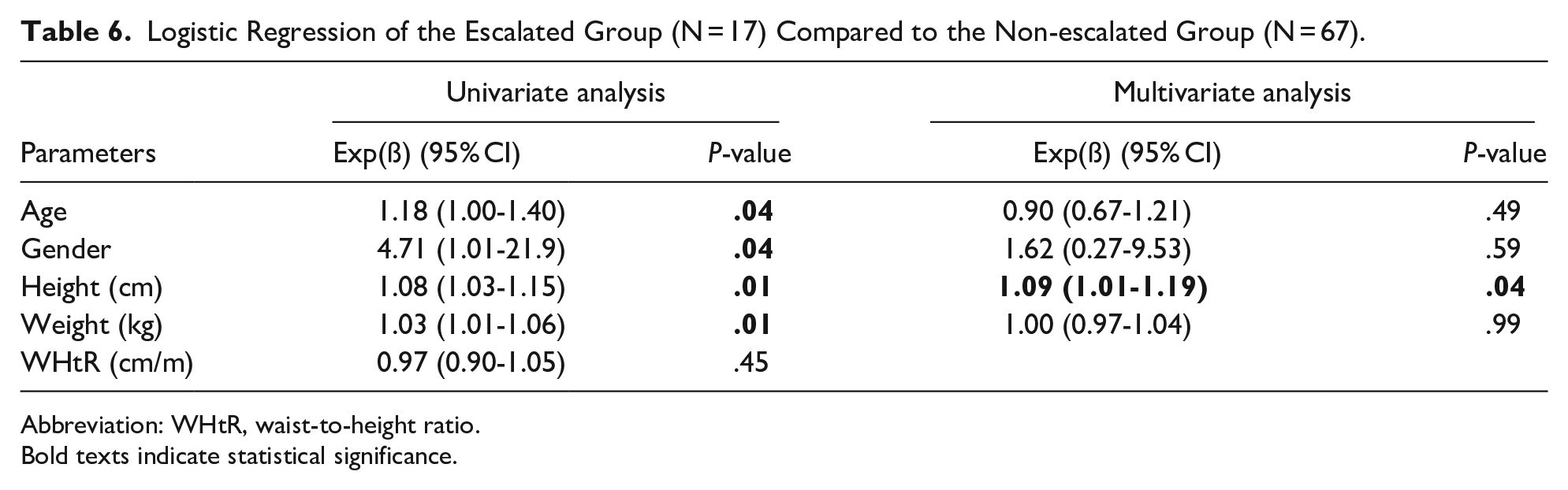
Abbreviation: WHtR, waist-to-height ratio.
Bold texts indicate statistical significance.
Discussion
The present study revealed that the prevalence of HT increased when using the 2022 AHA guidelines compared to the 2014 AHA guidelines. An abnormal ABPM was increased from 48% to 65%. These findings were concordant with the previous studies comparing the 2014 AHA pediatric and 2017 AHA/ACC adult guidelines in adolescent patients, which found an increase in 10% to 30% diagnosis of sustained HT and masked HT.12,13,15,16,20
Based on the changes in the ABPM cut-off in ages ≥13 years, the prevalences of sustained and masked HT were increased when using the 202 AHA guidelines from 43% to 50% and 5% to 15%, respectively. In the escalated group, children aged ≥13 years had all types of HT, including awake HT, nocturnal HT, and 24-hour HT, whereas children aged <13 years had only nocturnal HT. When compared to awake HT, nocturnal HT was more significantly increased from 35% to 59% (P < .01) vs 30% to 36% (P = .03). These findings were also detected in the previous studies.13,20 This could be due to the fact that the 2022 AHA nocturnal SBP cut-off (adult’s cut-off) was lower than the 95th percentile in males and females ages over 8 and 7 years compared to those ages over 12 and 15 years for the awake SBP cut-off.9,15
Both systolic and diastolic HT were increased by 40% to 50% in the present study. Previous studies in CKD patients also found an increase in both systolic and diastolic HT when using the adult ABPM cut-off.15,21 Due to removing BP load and changes in the ABPM cut-off in the 2022 AHA guidelines, pre-HT and unclassified phenotypes were eliminated (8% and 24% in the present study, respectively). Seven out of 8 patients (87.5%) previously diagnosed with pre-HT were reclassified into masked HT, which was approximate to the previous studies with an escalation in diagnosis of 70%.20,21 For the unclassified group, 9 out of 24 patients (37.5%) were reclassified into masked or sustained HT.
The prevalence of white coat HT using the 2022 AHA guidelines was increased from 12% to 27% in the present study. This result was different from the previous studies by Hamdani et al, 22 which showed a decrease of 16% prevalence of white coat HT. This could be due to the different patient populations between the 2 studies. In addition, the study by Campbell et al did not include the unclassified phenotype, while it was about 24% in the present study. On the contrary, the present study revealed that 15 of 24 patients (62.5%) were reclassified into white coat HT, which was also seen in the pilot study by Hill-Horowitz et al. 21
Age, gender, height, and weight were the demographic data related to an escalation in diagnosis compared to the non-escalated group. However, after multivariate analysis, height was the only independent factor related to the escalation in the diagnosis of HT, with an OR of 1.17 in our study. This was consistent with the previous study that showed reclassification in tall male patients.16,21 The reason was that the 95th percentile BP for tall adolescents was more than the adult cut-off, seen in male adolescents with heights more than 135 to 155 cm and female adolescents with heights more than 140 to 170 cm. 9
Based on the present study, it can be inferred that using the 2022 AHA guidelines was more associated with LVH than the 2014 AHA guidelines for the following reasons. First, 5 out of 6 patients who had pre-HT or unclassified phenotypes and LVH were escalated into masked or sustained HT. Only 1 patient, however, was de-escalated into white coat HT. Still, this patient was also obese, which could have contributed to a high left ventricular mass index, according to previous studies.23,24 This demonstrated that, by the 2022 AHA guidelines, these individuals at risk of developing LVH would be reclassified as having either masked or sustained HT. Second, when using the 2014 AHA guidelines, LVH was not significantly different between the different ABPM phenotypes, while it was significantly different when using the 2022 AHA guidelines. This is consistent with the previous pediatric cohort studies that demonstrated the adult ABPM cut-off to be a more accurate predictor of LVH but the BP loads to be poor indicators of target organ damage.12 -14,21,25,26
Although the present study was the first study comparing the 2014 and 2022 AHA guidelines in Asian pediatric populations with clearly defined phenotype reclassification, it has several limitations. Firstly, it was a single-center study, and a limited number of patients were included. Secondly, the sample size calculation was not done as the convenient samples were used. Thirdly, data regarding end-organ damages, such as left ventricular mass index, was limited to only 36%. Finally, the etiologies of HT in the participants were mixed between primary and secondary HT. A more extensive study with subgroup analysis between different causes of HT needs to be conducted to explore the performance of the 2022 AHA guideline in predicting end organ damage.
Conclusion
Using the 2022 AHA guidelines increased the prevalence of HT, including both sustained and masked HT. Nocturnal HT was more increased than awake HT because the nocturnal SBP cut-off of the 2022 AHA guidelines in ages ≥13 years was much lower than the 95th percentile of the 2014 AHA guidelines. Most of the pre-HT and some of the unclassified patients were reclassified into masked or sustained HT. The classification by the 2022 AHA guidelines was more related to the target organ damage than the 2014 AHA guidelines, as most patients with LVH were reclassified into masked or sustained HT when using the 2022 AHA guidelines. The escalation in the diagnosis of HT was seen among tall patients.
Footnotes
Acknowledgements
We are thankful for the participating patients and families. We also would like to thank Mr. Wirot Phairotsakun, Mrs. Kittirat Phairotsakun, Mr. Khobchai Phairotsakun, Mrs. Nuntawan Chayakul and Mr. Naratach Chayakul for donating the TM-2430 devices.
Author Contribution Statement
NN, KP, SC, PS, and KT contributed to the conception and performed the study. NN and KP contributed to the acquisition, analysis, and interpretation of data. NN and KP drafted the manuscript. NN, KP, SC, PS, and KT critically revised the manuscript for important intellectual content. NN, KP, SC, PS, and KT approved the final version of the manuscript.
Data Availability Statement
The datasets used and analyzed during the present study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved by the Ethics Committee for Human Research of the Faculty of Medicine Ramathibodi Hospital (MURA 2020/1792). The study was granted exemption from informed consent due to its retrospective design.