
Abstract
Objectives. This study aims to report clinical features and treatment outcomes of 16 cases diagnosed with post-influenza encephalopathy/encephalitis. Methods. We recorded clinical characteristics of 16 pediatric patients diagnosed with post-influenza encephalopathy/encephalitis at the Vietnam National Children’s Hospital from January 2019 to January 2021. Results. There were 87.5% infected with influenza A, with influenza A/H1pdm09 and influenza A/H3 accounting for 88.9% and 11.1% respectively, and 12.5% of participants infected with influenza B. The time from onset to the appearance of neurological symptoms was 3 days, of which perceptual changes (93.8%), hypertonia (75%), and seizures (43.8%) were prevalent neurological symptoms. The majority of cases had normal cerebrospinal fluid. Cranial CT/MRI imaging revealed abnormalities in 87.5% of patients. 56.3% of patients had sequelae, including epilepsy and cerebral palsy; 25% recovered, and 18.8% died after treatment. Conclusions. Influenza-associated encephalitis/encephalopathy is a complication occurring early in children, with high mortality and sequelae rates.
Introduction
Influenza is among the most prevalent causes of acute lower respiratory infection (ALRI), especially in young children. In 2018, there were an estimated 10.1 million influenza-virus-associated ALRI cases, 870 000 influenza-virus-associated ALRI hospital admissions, and nearly 34 800 influenza-virus-associated ALRI deaths among children under 5 years of age worldwide. 1 Over 80% of in-hospital deaths took place in low-income and lower-middle-income countries. 1 Although influenza usually resolves on its own, it has led to complications in many pediatric patients, ranging from such minor complications as acute otitis media (AOM) to more severe conditions such as respiratory failure or death. 2
Previous research also reports non-respiratory complications secondary to influenza. 3 Rare but essential neurological complications are reported at the rate of 7.6% of children hospitalized for influenza.3,4 Young children, both healthy and chronically ill, are vulnerable to neurologic complications after influenza, including encephalopathy and encephalitis, and the fatality rate of influenza-associated neurologic complications among this group is as high as 30%. 5 Influenza-associated encephalopathy/encephalitis is uncommon, occurring in 1.4% of hospital admissions due to influenza across studies, but severe complications with increased mortality of up to 30% in children and neurological sequelae at about 30%.4,6-8
Currently, indicators for early diagnosis of influenza-associated nervous system injury in general and encephalopathy/encephalitis are scarce, resulting in delays in the early diagnosis of critical cases, poor prognosis, and mortality. In this study, we described 16 instances of post-influenza encephalitis that received inpatient treatment at the Vietnam National Children’s Hospital, Hanoi, to understand the clinical and subclinical characteristics, brain lesions, and treatment outcomes.
Methods
Study Design
We conducted this case series study from January 2019 to January 2021 at the Center for Tropical Diseases, Vietnam National Children’s Hospital.
Selection of Subjects
Cases of influenza were defined when pediatric patients present with influenza-like clinical manifestations and real-time reverse transcription polymerase chain reaction (qRT-PCR) tests detect influenza viruses in nasopharyngeal fluid, and specimens were tested negative for other viruses such as adenovirus, rhinovirus, respiratory syncytial virus, and Parainfluenza virus.
Encephalitis was diagnosed when the child has a perceptual disorder that lasts at least 24 hours without other causes and at least 3 of the following sub-criteria: (1) Fever within 72 hours before or after the onset of symptoms; (2) Seizures (generalized or focal) not attributable to other causes; (3) Other new focal neurological manifestations; (4) The number of leukocytes in the cerebrospinal fluid of more than 5 cells/ml; (5) Abnormalities on CT/MRI of the central nervous system toward encephalitis; and (6) Abnormality on electroencephalography that is consistent with encephalitis and not attributable to another cause. 9
Influenza-associated encephalopathy/encephalitis was determined when patients had a positive pharyngeal/endotracheal influenza PCR test and were diagnosed with encephalopathy/encephalitis of causes other than common factors, such as Herpes simplex Virus (HSV), Enterovirus (EV), Japanese encephalitis virus (JEV), Mycoplasma. 7
Classification of Patients Upon Discharge From the Hospital
Patients were clinically examined before being discharged from the hospital and divided into 4 groups as follows: (i) no sequelae; (ii) mild or moderate sequelae without effects on daily living; (iii) severe sequelae, requiring assistance with activities of daily living; and (iv) mortality.
Data Collection
Data about the eligible cases were reviewed and collected retrospectively. Caregivers provided indicators of medical history and clinical course before admission to the hospital. Clinical course variables were collected when at least 2 pediatric infectious disease doctors confirmed. The criteria used in this study were according to the pediatric definition. Tests for influenza were done as soon as the child was admitted to the hospital. Testing for influenza viruses in cerebrospinal fluid and other viruses that cause respiratory infections and encephalitis was carried out immediately in the presence of neurological manifestations. Test indicators were collected when results were available from the laboratory. The PCR test in cerebrospinal fluid was conducted using the AB17500 fast system, with the Invitrogen SuperScript TMIII Platinum® One-Step Quantitative kit as the reagent. The test was carried out at the Laboratory of Molecular Biology for Infectious Diseases (ISO 15189 – 2014), Vietnam National Children’s Hospital, Hanoi.
Ethics
The study was approved by Vietnam National Children’s Hospital, Hanoi, Vietnam (Code: IRB – VN01037/IRB00011976/FWA00028418). All data were only used for research purposes. Written informed consents from parents or caregivers of the subjects were collected. The study did not affect the rights or benefits of any patient in this report.
Results
The study described 16 patients diagnosed with influenza and presenting encephalopathy or encephalitis.
Table 1 summarizes the demographic characteristics and clinical symptoms of participants. The participants ranged from 1 month to 18 years old, with 12 (75%) patients in the study under 5 years of age. The male/female ratio is 10/6. In this report, no child received a flu vaccine in the previous 6 months. There were 7 patients with underlying medical conditions, accounting for 43.8%, including 2 (12.5%) patients with psychomotor retardation, 1 (6.2%) patient with epilepsy, 1 patient (6.2%) with a history of previous febrile seizures, 2 sibling patients (12.5%) diagnosed with amino acid metabolism disorder during hospitalization, and 1 (6.2%) patient with renal tubular acidosis.
Demographic Characteristics and Clinical Symptoms of Patients.
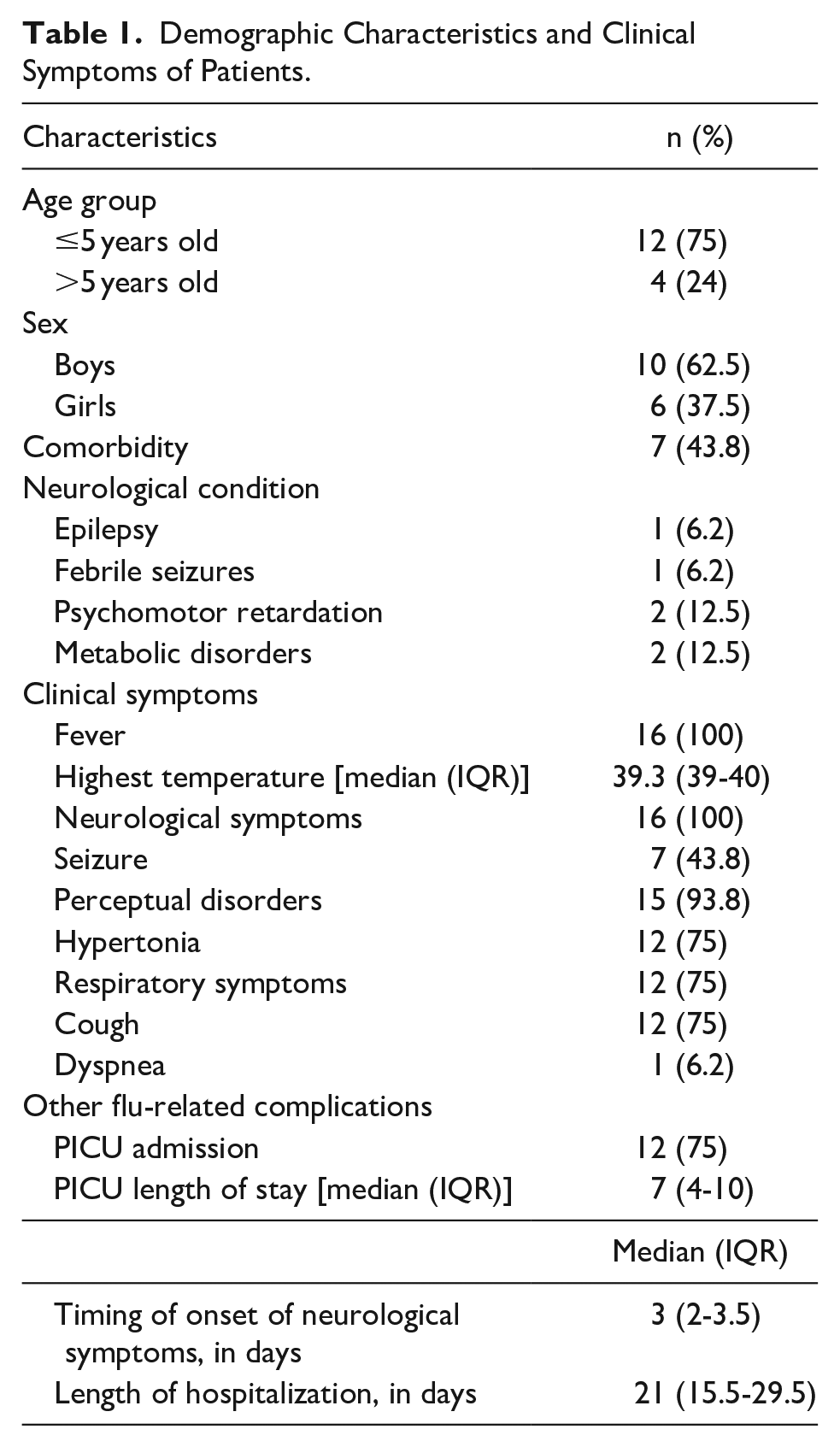
The time from the first symptoms to the onset of neurological symptoms was 3 days (1-6 days). Sixteen (100%) of patients had a fever, 12 (75%) had a cough, and 1 (6.2%) had dyspnea. In addition, 15 (93.8%) patients had perceptual changes, 7 (43.8%) had seizures, hypertonia accounted for 12/16 (75%), and no patients experienced focal paralysis. These 12 patients (75%) were admitted to the PICU for treatment; the average duration of treatment in the PICU unit was 7 days (ranging from 4 to 10).
The results of the patient’s tests are presented in Table 2. Cerebrospinal fluid testing was performed in all patients, including 3 (25%) patients with increased white blood cell counts accompanied by a protein increase of over 0.5 g/l; 1 (6.2%) patient had an increase in white blood cell count, and 2 (12.4%) patients had a protein increase over 0.5 g/l. Other patients had normal results. PCR tests for influenza virus RNA in cerebrospinal fluid were negative. This indicated that the influenza virus might not directly cause encephalitis or post-influenza encephalopathy. Type-specific identification of influenza viruses was performed in all patients, of which influenza A accounted for 87.5% and influenza B accounted for 12.5%. Sub-type identification of influenza A virus was performed on 9 patients with influenza A and identified influenza A/H1pdm09 in 8 (88.9%) patients and H3 in 1 (11.1%) patient. Four patients (25%) had a white blood cell count within normal limits, 7 (43.7%) had an increased white blood cell count, and 5 (31.3%) had a reduced white blood cell count. In addition, 10 (62.5%) patients had an elevated CRP above 6 mg/dl.
Changes in Laboratory Characteristics.

Table 3 reveals the influenza type, CSF analysis, cranial MRI, clinical diagnosis, treatment, and outcomes of the 16 cases. Abnormalities were found in 14/15 (93.3%) brain CT/MRI scan results (representative MRI results as in Figure 1). Most patients (86.7%) had varying severity lesions in the cerebral cortex and gray nuclei. These lesions increased signaling on T2 pulses and bilateral symmetry at cortical sites, thalamus, caudal nucleus, putamen, periventricular white matter, brain stem, and cerebellum. Regarding treatment and outcomes, 15 patients (93.4%) used Oseltamivir, 12 (75%) received corticosteroids, and 1 (6.2%) was prescribed immunoglobulin. After the treatment, 4 (25%) patients recovered without sequelae, and 9 (56.3%) patients had sequelae. A total of 3 patients (18.8%) died, including 1 case after 48 hours of hospitalization, 1 case after 10 days of deep coma, and 1 case after being hospitalized for 63 days, not due to brain damage.
Influenza Type, CSF Analysis, Cranial MRI/CT, Clinical Diagnosis, Treatment, and Outcome.

Abbreviations: CSF, cerebrospinal fluid; WBC, white blood cell; WM, white matter; GN, gray nuclei; IVIG, intravenous immune globulin.

Representative MRI results. (a and b) 55-month-old boy; lesions at thalamus, caudal nucleus, lenticular nucleus, 2-sided white matter. (c and d) 27-month-old boy; lesions at thalamus, hippocampus, bilateral pons.
Discussion
In our study, 12/16 patients were under 5 years of age. The study results are consistent with those of authors Wada et al, showing that neurological complications are more common in children under 5 than in older age groups.10,11
Influenza often occurs in young children; the central nervous system is immature and vulnerable. In addition, the study found that more boys had the disease than girls, and the results were similar to many analyses by other authors.10,11
In our study, 43.8% of patients had comorbidities, including 4 patients with comorbid neurological disorders, 2 with congenital amino acid metabolism disorders, and 1 with renal tubular acidosis. In addition, a study by Newland et al, 12 and Khandaker et al 13 showed a 5.6-fold and 6.5-fold increase in neurological complications in children with neuromuscular disorders compared to typical children.
The average onset time of neurological symptoms (seizures, perceptual changes) was 3 days, ranging from 1 to 6 days. This result differs from previous studies, in which neurological symptoms appeared 24 to 48 hours after the first symptom. However, the observed difference can be attributable to the nature of the present neurological complications and can vary with the number of patients. 7 The most common neurological symptoms were perceptual changes, hypertonia, and seizures, the first to occur. This result is consistent with the findings of Wada et al, 10 which indicated that seizures were usually the first manifestation in children under 5 years of age. According to Mastrolia et al, 7 the first neurological symptom in all children under 2 years of age admitted to the hospital with respiratory symptoms (cough or shortness of breath) was perceptual changes.
Only 6 (37.5%) patients in our study had cerebrospinal fluid abnormalities. In addition, we did not find influenza virus RNA in cerebrospinal fluid. The current findings were similar to those of Mastrolia and Muhammet Sukru Paksu, with only 14% and 18% of cases with an increase in the number of leukocytes and proteins, respectively, in the cerebrospinal fluid.3,7 Low levels of white blood cells and proteins in the cerebrospinal fluid were observed in most patients with brain lesions shown on CT/MRI films, suggesting that the mechanism of lesions may be due to the inflammatory or immune-mediated response6,7 Levels of proinflammatory cytokines, such as interleukin (IL)-6, IL-1b, tumor necrosis factor (TNF)-α, and soluble TNF receptors are reported to be elevated in cerebrospinal fluid and plasma in patients with influenza-associated encephalopathy/encephalitis. Levels of other cytokines/chemokines also increase in cerebrospinal fluid and plasma. Serum IL-6 levels are correlated with a poor prognosis, and the chronological evolution of serum IL-6 levels also reflects clinical status. The severity of the disease is associated with the concentration of proinflammatory cytokines. 3
Nevertheless, the pathogenesis of influenza-related encephalopathy/encephalitis remains ambiguous and requires further research with a larger sample size.
The determination of influenza virus type showed that influenza A/H1pdm09 was the most prevalent, while there was only 1 patient infected with influenza A/H3 and 2 patients with influenza B. The high prevalence of influenza A/H1pdm09 was also observed in studies by Paksu et al 6 and Mastriolia et al. 7 However, due to the small study data, we could not compare the differences between the above etiological groups.
Regarding the characteristics of lesions on cranial CT/MRI results, 81.3% of study subjects had increased signaling lesions on T2 pulses, with bilateral symmetry at central gray nuclei, periventricular deep white matter, brain stem, and cerebellum. Our observations were similar to a previous study by Wada et al 10 and case reports of Fuchigami et al 14 and Goenka et al. 15 Although brain lesions are nonspecific and the mechanism of lesions has yet to be well-established, lesions observed from cranial CT/MRI results can assist in the diagnosis, prognosis, and initial treatment guidance. 16
Regarding leukocyte counts and serum CRP, only 25% and 37.5% of patients had leukocyte counts and serum CRP in the normal range, respectively. The study results differ from Mastrolia et al’s 7 data. However, the change is insignificant.
Most patients in our study were given Oseltamivir. Unfortunately, the efficacy of Oseltamivir in these cases is not observable. However, due to the severity of the disease, the timing of the onset of neurological symptoms, and the role of infection in triggering the inflammatory process of the central nervous system, Oseltamivir is recommended for use as soon as possible. The use of immunomodulatory drugs (Corticosteroids and Immunoglobulins) remains controversial. However, evidence of immune-mediated pathogenesis supports the clinical use of these drugs. 7
The current study recorded 3 deaths, different from Mastrolia et al’s, 7 with 14 out of 15 patients recovered and 1 with mild sequelae. In another study by Philip N. Britton from 2013, Britton from 2015 on 54 patients with influenza-related neurological manifestations, the mortality rate among ten patients with encephalopathy/encephalitis was 20%, and the sequelae rate was 37.5%. 4 Factors such as patient age, comorbidities, vaccination status, and duration from onset of neurological symptoms in our case series were not significantly different from the 2 studies above. However, we could not compare the above groups due to the small number of patients and lack of reports in Vietnam.
The results of this study should be viewed considering some limitations. We included all eligible cases during the study period instead of following power analysis for sample size calculation, limiting the study results’ extrapolation ability. Since this is a rare complication and data were collected in 1 hospital only, the number of cases is limited. In addition, the PCR testing in CSF used in our study has yet to be standardized for the Influenza virus and may lead to some deviations in the interpretation of the test results.
Conclusions
The complication of encephalitis/encephalopathy associated with influenza is an early complication. In the current study, encephalitis/encephalopathy was mainly seen in children under 5 years old with accompanying comorbidities. Clinical features include altered consciousness, seizures, and increased muscle tone. In addition, normal cerebrospinal fluid does not rule out damage. CT/MRI brain scans showed lesions in multiple locations of white matter and central gray nuclei. Mortality and sequelae rates were high. Given the characteristics and onset symptoms of cases examined in this study, encephalopathy/encephalitis complications should be examined in all hospitalized influenza-infected children with neurological symptoms.
Footnotes
Acknowledgements
None.
Author Contributions
LVN: Contributed to the conception of the study and supervised the work process; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. DSN: Contributed to analysis and interpretation; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. QTP: Contributed to the acquisition of data; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. HTD: Contributed to the acquisition of data; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. DMT: Contributed to the conception of the study and supervised the work process; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. TVC: Contributed to the conception of the study and supervised the work process; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. HTP: Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. TQP: Contributed to the conception of the study and supervised the work process; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Availability of Data and Materials
Data is available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by Vietnam National Children’s Hospital, Hanoi, Vietnam (Code: IRB – VN01037/IRB00011976/FWA00028418). All data were only used for research purposes. The study did not affect the rights or benefits of any patient included in this report.