
Abstract
Objectives. This study aimed to analyze the inter-molar width and skeletal base class to predict maxillary canine impaction in permanent dentition. Methods. This cross-sectional study was carried out between September 2021 to March 2022. Patients aged between 13 and 20 years were recruited. These patients’ cone-beam computer tomography(CBCT), lateral cephalogram, and dental casts were collected and analyzed. For statistical analysis, T-test and Chi-square tests were applied. Results. A total of 92 patients were enrolled in this study. Inter-molar width was significantly decreased in patients with impacted canine(P < .001). The skeletal base classification was statistically significant when compare with intermolar width(P < .05). The location of impaction (P = .060), type of impaction(P = .435), and side of impaction(P = .239) were determined to be statistically insignificant. Conclusion. The Inter-molar width was decreased in patients with impacted canine; therefore, it may be a potential risk factor. The skeletal classification was found to affect inter-molar width in impacted canine patients.
Introduction
After the maxillary and mandibular third molars, the maxillary canines are the third most impacted teeth, 1 and there are more palatally impacted maxillary canines than labially impacted maxillary canines. Moreover, maxillary canines are more commonly impacted than mandibular canines. 2 The etiological factors for both types of impactions are different with labial canine impaction is mainly caused by dental crowding, 3 and the etiology of palatally impacted maxillary canines is related chiefly to growth direction 4 and genetic theory.5,6 However, if maxillary canines remain impacted, complications such as resorption of adjacent teeth, cyst formation, infection, and dislodgement of neighboring teeth may arise. 7
Several diagnostic tools are currently employed to identify and manage canine impaction, including orthopantomograms (OPGs), periapical films, occlusal films, and lateral cephalograms. However, the most effective tool for diagnosing and treating complex impacted canine cases is cone-beam computed tomography (CBCT) (7). CBCT provides superior diagnostic accuracy and reliability when evaluating the position of impacted maxillary canines. By utilizing 3D rendering techniques, CBCT generates high-resolution images that prove invaluable for both diagnosis and treatment planning in cases involving impacted maxillary canines. 8 The mesiodistal angulation of the impacted canine crown and its overall angulation can serve as predictive factors for treatment success. Ericson and Kurol found that an impacted canine with a more mesially positioned crown is less likely to erupt after primary canine extraction. 9
Early detection of impacted maxillary canines involves a clinical assessment of the permanent lateral incisors. The angulated or unusual positioning of these incisors can serve as indicators of potential canine impactions. It is worth noting that a distally tipped lateral maxillary incisor is a normal occurrence during the mixed dentition stage and does not necessarily signify a displaced canine. 6 In typical cases, the canine’s root naturally “slides” along the lateral incisor’s root, and alignment occurs as the canine continues to erupt. 3 However, a labially tipped lateral incisor crown may suggest a labially placed canine in comparison to the lateral incisor’s root. Additionally, severe mobility of the lateral incisor may indicate root resorption caused by a displaced canine, which demands prompt attention and appropriate treatment to preserve the affected tooth. 10 These signs should not be disregarded, and timely intervention can play a crucial role in saving the tooth.
The transverse maxillary discrepancy is often linked to maxillary canine impaction. A study suggested using maxillary orthopedic expansion as an interceptive treatment for palatally displaced canines. 11 Surgical exposure and long-term orthodontic treatment may damage the impacted canines’ periodontal structures and impose a financial burden on patients. 12 Early orthopedic expansion is a viable option to address transverse maxillary discrepancies and lower the risk of canine impaction, potentially avoiding more complex and costly treatments later on. 13
Patients with a transverse discrepancy are reportedly more prone to unilateral canine impaction than those without such a discrepancy. 14 Transverse maxillary deficiency is frequently observed in young individuals, typically between the ages of 8 and 10 years, coinciding with the eruption of maxillary canines around 10.5 years in females and 11.5 years in males. To mitigate the risk of canine impaction, maxillary expansion can be utilized when necessary to address the transverse deficiency. 14 Surprisingly, the mean maxillary intermolar width in individuals with impacted canines has not been investigated in the local population.
This study aimed to investigate the mean maxillary intermolar width in patients presenting with impacted canines, as there is limited research on this topic in terms of Pakistani context. The findings of this study can have significant implications for future clinical practice by providing valuable insights into intermolar width expansion. By identifying cases with deficient maxillary intermolar width, clinicians can effectively intercept canine impaction, potentially avoiding the need for lengthy and costly comprehensive orthodontic and surgical procedures. The potential benefits of this research lie in its contribution to early intervention and preventive measures. With early identification of patients at risk for canine impaction due to narrow maxillary intermolar width, clinicians can implement timely orthodontic or orthopedic expansion techniques. This proactive approach may alleviate the need for more invasive treatments later in life, reducing both the treatment duration and financial burden on patients and their families.
Materials and Methods
Study Design and Sample Size
This cross-sectional study was carried out at the Department of Orthodontics. The duration of this study was from the 2nd of September 2021 to the 2nd of March 2022. Data collection was started after being approved by the research ethics and review committee at University (ethical number: AIDM/ERC/07/2021/03). This study was carried out in compliance with the Declaration of Helsinki and was approved by the University ethical review committee. This study’s participants were selected using a non-probability convenience sampling method due to the eligibility criteria of the study. 15 The sample size of this study was calculated using the WHO sample size calculator. 16 By keeping the mean and standard deviation of intermolar width among the patients with canine impaction (44.858 ± 1.9), 17 5.5% as the margin of error, and the confidence interval at 95%. The sample size was determined to be 92. Prior to participation, written and verbal consent were obtained from the patients above 18-year old and written informed consent was obtained from the legally authorized representative of the subjects who are less than18 years of age to ensure voluntary participation.
Data Collection Procedure
Ninety-two patients between the ages of 13 and 20 years were chosen to participate in this study. Written and verbal consent were obtained from the patients above 18-year old and written informed consent was obtained from the legally authorized representative of the subjects who are less than 18 years of age to ensure voluntary participation. CBCT and dental casts, along with the age and gender of the patients, were studied. CBCTs’ were used to evaluate the position of the impacted maxillary canine, as presented in Figure 1.

CBCT of the impacted maxillary canine. (a) CBCT of impacted canine and (b) CBCT axial view of impacted canine.
The intermolar width at first molars was evaluated on the dental cast with the help of a pointed vernier caliper, read to the nearest 0.1 mm, as presented in Figure 2. The intermolar distance was measured using the transverse distance between the left and right first molars’ central fossa and the transverse distance between the palatal grooves of the left and right first molars.
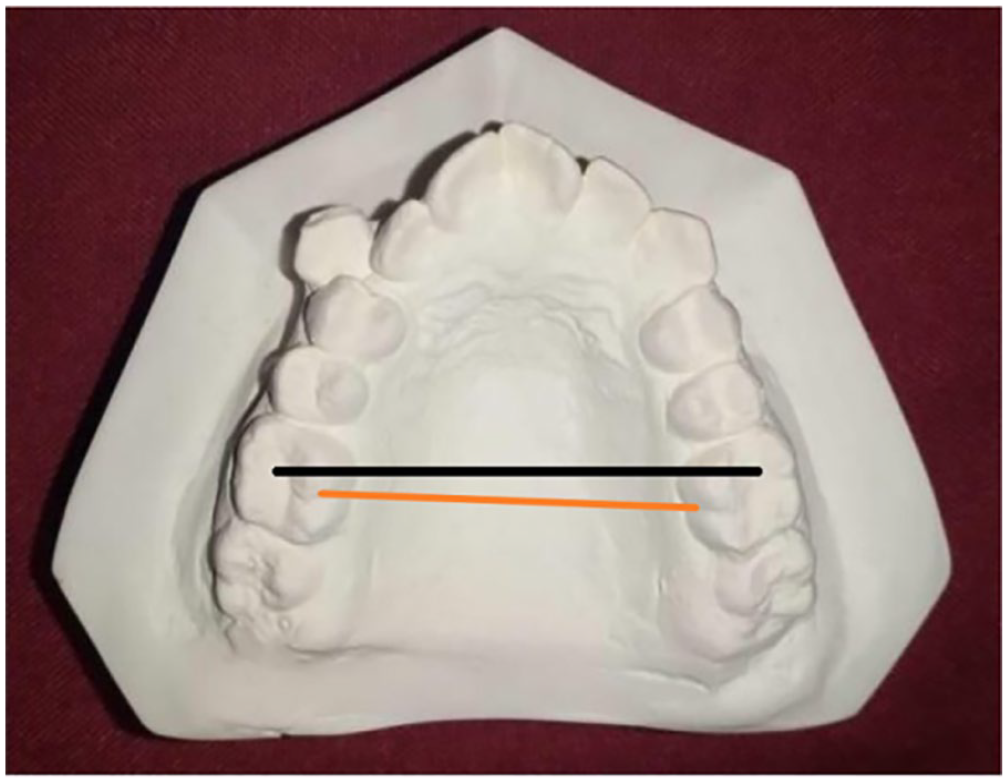
Measurement of intermolar width on a dental cast.
The Skeletal Base Class was analyzed on a lateral cephalogram; the 3 classes were recorded as follows:
• Skeletal Class I: If the mandible was in proper Sagittal relationship with the ANB angle between 0° and 4°.
• Skeletal Class II: Maxilla was Prognathic or mandible in a retrognathic position or both.
ANB Angle was above 4°.
• Skeletal Class III: Maxilla was retrognathic, the mandible prognathic, or both.
ANB angle was below 0°.
Inclusion and Exclusion Criteria
The purpose of participation in this study was to evaluate the maxillary intermolar width of the patients who had impacted maxillary canines. The participants in this study were included based on the following inclusion criteria:
• Subjects between 13 & 20 years of age.
• Buccally, vestibular, or palatally impacted maxillary canine.
• Unilateral or bilateral impacted maxillary canine with skeletal Class I & II, III relationship.
• Males and females both were included.
• Cone-beam Computed tomography (CBCT) with adequate contrast.
• No serious medical illness, previous facial surgery, deformities, or history of facial or dental trauma.
The participants who were excluded from the study were due to:
• Patients with known medical illnesses.
• Subjects with previous orthodontic treatment.
• Subjects with craniofacial syndromes, facial deformity, asymmetries, or Cleft Lip or Palate.
• Grossly carious maxillary posterior teeth and Rotations of upper posterior teeth.
Statistical Analysis
For analysis of the collected data, SPSS version 23 was used. Mean and standard deviation or median (IQRR) were calculated based on age and intermolar width normality. Frequency and percentage were calculated for gender, skeletal classification, location, and side of impaction. The effect modifiers like age, gender, skeletal classification, location, and side of impaction were controlled through stratification. One sample t-test was used to assess the variance of intermolar width with a mean sample value. The Chi-square test evaluated the relationship between the skeletal base class and intermolar width. A P-value of ≤.05 was considered statistically significant.
Results
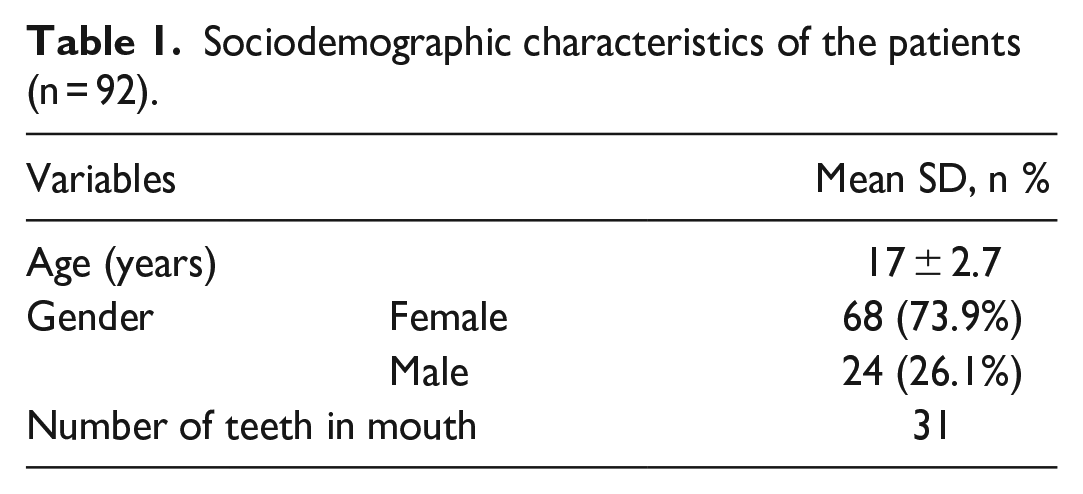
In this study, 92 patients participated, and their data were analyzed. The mean age of the participants was found to be 17 ± 2 years with a minimum of 13 years and a maximum of 20 years of age. Out of the 92 patients, there were 68 females and 24 males. The average number of teeth of the patients was 31, with a median value and IQR of 32, minimum of 28 and a maximum of 32, as presented in Table 1.
Sociodemographic characteristics of the patients (n = 92).
According to the skeletal classification, 50% of the patients were categorized as skeletal class 1, 44% as skeletal class 2, and 6% as skeletal class 3, as shown in Figure 3. In terms of intermolar width, all participants had an average width of 42.5 ± 3.4 mm, with a minimum of 32.2 ± 1.9 and a maximum of 49.8 ± 4.3. Analyzing the location of impactions, approximately 45% of the participants had palatal impactions, 18% with vestibular impactions, while around 32% had buccal impactions, and only 4% had impactions in the line of the arch area. The majority of participants, approximately 80%, exhibited unilateral impaction, whereas only 20% had bilateral impaction when considering the type of impaction. Additionally, around 70% of the participants had impactions on the left side of their mouth, as indicated in Table 2.

Skeletal base class distribution of the patients (n = 92).
Baseline characteristics of the patients (n = 92).

Abbreviations: ANB, angle between points A and B; SD, standard deviation; n, frequency; %, percentage.
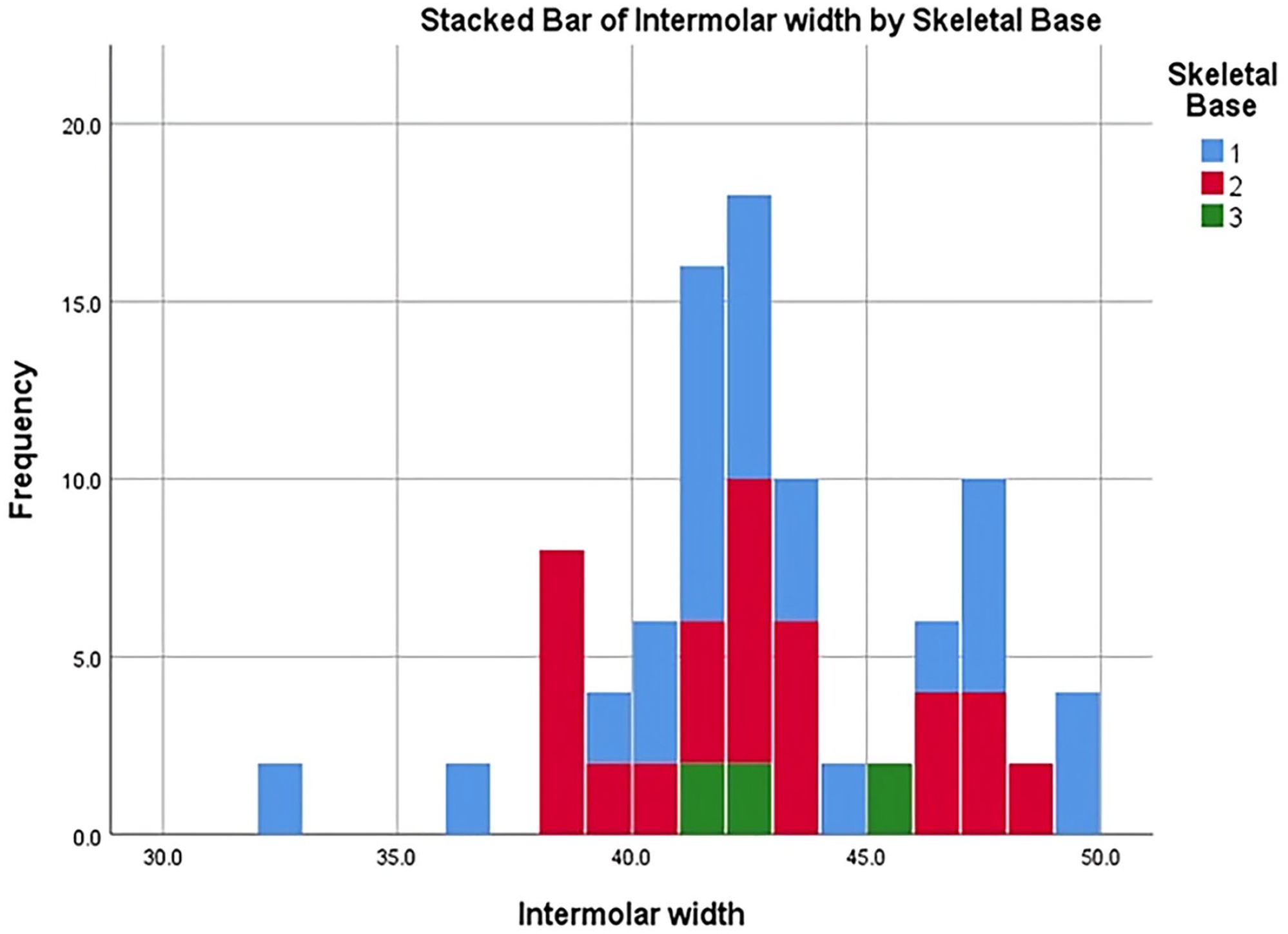
When testing for the significance of covariates, the intermolar width (in mm) was found to be highly significant (P < .001) after applying the one-sample t-test, whereas no statistical difference was found in the gender groups (P = .108). The chi-square test was used to determine the relation of Skeletal Base Class with intermolar width and the P = .040 was found to be statistically significant, which indicates that the skeletal base class influenced intermolar width. Whereas no other variables such as location, type, and side of impaction were found to be statistically significant when tested using the chi-square test, this can be seen in the results contained in Table 3. When the intermolar width was stratified based on Skeletal Base Class, we observed that the distribution range of intermolar width immensely varied for Skeletal Base Class 1, ranging from 32 – 50 mm, significant difference was found within the skeletal class 1values (P = .001). Most Skeletal Base Class 2 cases had an intermolar width between 38 and 43mm, while a few cases of the same skeletal base class were observed to have intermolar widths between 45 and 48mm. Since the frequency of Skeletal Base Class 3 was minimal (n = 6), their intermolar width was observed to be 40 – 45 mm, in both class 2 and 3 skeletal bases the values were not significantly different (P > .05). Furthermore, the results in Figure 4, summarize the varying intermolar widths of different skeletal base classes and signifies the relationship of Skeletal Base Class & Intermolar width (P < .05), as presented in Table 3.
The comparison of intermolar width covariates.

Abbreviation: IW, Intermolar width.
One sample t-test was applied using a prevalence of 45.91 mm with P = .05 as the level of significance.
Chi-square test of independence was applied to keep the level of significance at P = .05.
Distribution of intermolar width (mm) according to the Skeletal Base Class of the patients (n = 92).
Discussion
Maxillary permanent canines are essential teeth in providing smile esthetics, guiding the functional occlusion, biting food, and supporting the upper lip. Canines are essential for providing a consonant smile. When the permanent maxillary canine is missing or impacted due to any etiological factor, functional occlusal and esthetic problems are seen.
The inability of a tooth to erupt in its usual eruption time, even when the root formation is complete, is known as impaction. Canine impactions are usually encountered in the field of orthodontics. After the third molars, maxillary canines are the most commonly impacted teeth.5,17 The prevalence of maxillary-impacted canines ranges from 0.27% to 2.4% in the general population. 18 In our study, it was seen that females had a higher frequency of canine impaction than males. Such findings correspond with a study in the literature that reports a higher incidence of impacted canines occurring in females. 19 The greater frequency of canine impaction in females could be due to the greater frequency of small, peg-shaped, or missing lateral incisors associated with palatally displaced canines. 20 Moreover, this study concluded that palatal impaction of maxillary canines was encountered more than buccal impaction. However, according to a study by Oliver et al, buccally impacted canines are more prevalent in the Asian population. 21
According to the results of our study, we found that the intermolar width was significantly less in patients with impacted canines, as compared to normal values of intermolar widths without impacted canines. Similar findings have been reported in various studies in the literature where the intermolar width is decreased in patients suffering from impacted maxillary canines.22,23 However, this is not always the case, as the intermolar width is sometimes not significantly associated with the impaction of maxillary canines. 14 If this problem is intervened in the mixed dentition stage, we can help the normal eruption of canine into proper occlusion. Other reasons can lead to impaction of the canines due to primary tooth bud displacement, local obstruction, disturbance in normal development, local pathology, genetic cause, or absence of guidance from the distal aspect of the root of the maxillary lateral incisor. 24
It has been noted that impacted canine cases occur more commonly than in previous times. The reason can be that fewer teeth are lost due to caries and periodontal problems because of awareness about dental hygiene. 25 Space deficiency is encountered more commonly due to this reason. Moreover, space discrepancy is an important causative factor for buccal canine impactions. Now general practitioners are more trained in diagnosing impacted canines and referring them to the orthodontic department.
As we already know, diagnosing impacted canines needs clinical and radiological examination. Clinical examination and palpation should be done carefully. On a routine basis, two-dimensional radiographs like periapical view, cephalograms, and panoramic radiographs are used in the orthodontic department. However, a single two-dimensional radiograph does not provide information about the Bucco-palatal location of the maxillary impacted canine relative to the surrounding bone and teeth. 4
Many other techniques can be utilized to analyze the tooth’s buccolingual position through a two-dimensional radiograph, like tube shift and SLOB. 26 For an efficient three-dimensional view, CT and CBCTs are recommended. Due to increased cost, radiation exposure, and medico-legal problems, they are routinely not used. These problems can be reduced by following the ALARA technique. 27 CBCTs have the additional benefit of providing information about the resorption of the root of the adjacent teeth and the relation of the impacted tooth to the adjacent environment 3-dimensionally. With the help of CBCT, damage to adjacent structures around the impacted teeth can be avoided, leading to hemorrhage and paresthesia if damaged. 28
In many studies, it has been noticed that patients with maxillary transverse discrepancy may encounter canine impaction. As the maxillary width is defined early 29 in the mixed dentition stage, we can predict whether there will be a canine impaction or not, especially when other causatives/ risk factors are also present. In our study, we found that the average intermolar width of the patients was 42.5 ± 3.4. However, such findings contrast based on a study by Singh et al, which concludes that an average intermolar width ranges between 33.8 and 36.5 mm in children. 30 This discrepancy between intermolar widths could be due to variations between different ethnicities. When maxillary transverse discrepancy has been diagnosed, an active trans-palatal arch (TPA) or another maxillary expander can be used as interceptive treatment. It has been noticed in many studies that by using these appliances, there are fewer chances of canine impaction.31,32
The patients have a different skeletal base class; depending on this, the treatment plan varies from patient to patient, along with the type of canine impaction. Our study found that most patients with impacted canine belong to class 1 (50%) and class 2 (43.5%) skeletal base classes. Mercuri et al reported similar conclusions where a high prevalence of impacted maxillary canines are found in patients belonging to skeletal base class I. 33 However, our study reports a lower frequency of canine impaction in class III patients, as compared to class I and II patients. Similarly, no significant relationship has been noted in patients with impacted maxillary canine and skeletal class III as concluded by Di Carlo et al 34
According to our study, the most common side of impaction was the left side, with most patients having a palatal-canine impaction compared to a buccal-canine impaction. Furthermore, there was no significant result related to the location and side of impaction. These results are consistent with different studies in the literature that have concluded palatal impactions to be more frequently encountered than palatal impactions and left-sided impactions are more common.33-35
There are many treatment options depending on age, compliance, dental health, hygiene, spacing or crowding in the arch, the position of the canine, attached gingiva, and the shape of teeth. Most of the time patient does not want to go through any treatment. So, we can leave the canine untouched if it is away from the roots of adjacent teeth, with no pathology present, or in a higher position, and it will need invasive treatment.
When left alone, these teeth should be periodically checked through clinical and radiological examination. Radiographs should be taken after every 6 months to 1 year to see if the impacted tooth is causing any problem or not.36-38 The other treatment option will be to extract the impacted canine if proper occlusion is present, given that the lateral incisor and first premolar are in good proximal contact, as pathological growth is associated with the impacted canine, making it challenging to bring it correctly into the arch.
Rapid maxillary expander (RME) and leaf expander have also been shown to produce maxillary expansion similar to dental and skeletal changes. 39 Furthermore, a transverse sagittal maxillary expander (TSME) can transversely cause a maxillary expansion in patients suffering from maxillary hypoplasia. 40 Last but not least, the option will be to surgically expose the canine and bring it to the arch orthodontically.41-44 There are different techniques for exposing impacted canines. A minimally invasive technique should be used for the best outcomes.
Limitations and Future Recommendations
Despite the study’s strengths, including a substantial number of patients and meticulous measurements of intermolar widths, certain limitations were encountered. Firstly, the study did not include the adult population, and the absence of patients in mixed dentition phases limited the scope of evaluating canine eruption patterns. Moreover, the relatively small sample size hindered the comprehensive representation of the population and reduced the generalizability of the findings. Additionally, the inclusion of only patients with impacted canines may have caused selection bias, suggesting the need for future studies with a control group of individuals without impacted canines. To enhance precision, using advanced imaging techniques and involving multiple calibrated examiners for measurements could have addressed potential measurement errors. Furthermore, long-term follow-up studies would have been valuable in understanding the stability and effectiveness of expansion interventions on maxillary intermolar width over time.
Future recommendations for this study include the incorporation of a control group without impacted canines to enable direct comparisons and a deeper understanding of intermolar width differences. Collaborative efforts between multiple centers would enhance the sample size, diversity, and generalizability of the findings. Implementing advanced three-dimensional imaging techniques, such as cone-beam computed tomography (CBCT), could yield more accurate and detailed measurements of maxillary intermolar width. Further studies should evaluate the effectiveness of expansion techniques through early intervention strategies to prevent canine impaction and its impact on maxillary intermolar width. Additionally, exploring the influence of genetic and environmental factors on maxillary intermolar width and canine impaction may offer insights into individual susceptibility and potential preventive measures.
Conclusion
Intermolar width significantly decreased in patients suffering from impacted maxillary canines, as compared to the normal range. The skeletal base class was found to play a significant role in the impaction of maxillary canines. Therefore, the maxillary transverse discrepancy can lead to canine impaction and should be corrected early in life to prevent canine impaction.
Footnotes
Acknowledgements
The authors want to take this opportunity to express their appreciation to the patients who agreed to participate in this study. The authors are grateful to the research development and review cell of Altamash Institute of Dental Medicine Karachi, Pakistan, for guidance and support in this study. The authors’ team also grateful to the Yerevan State Medical University after Mkhitar Heratsi, Yerevan, Armenia, for supporting this project.
Authors’ Note
Artak Heboyan is also affiliated to Saveetha University, Chennai, India.
Author Contributions
HD: contributed to conception or design; contributed to acquisition, analysis, or interpretation; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AFE: contributed to conception or design; contributed to acquisition, analysis, or interpretation; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. HS: contributed to acquisition, analysis, or interpretation; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SM: contributed to acquisition, analysis, or interpretation; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AL: contributed to acquisition, analysis, or interpretation; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA: contributed to acquisition, analysis, or interpretation; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AM: contributed to acquisition, analysis, or interpretation; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AH: contributed to acquisition, analysis, or interpretation; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the Ethical and review committee of Altamash Institute of Dental Medicine (AIDM/ERC/07/2021/03).
Written Informed Consent
Written and verbal consent were obtained from the patients above 18-year old and written informed consent was obtained from the legally authorized representative of the subjects who are less than 18 years of age to ensure voluntary participation.
Trial Registration
Not applicable.