
Abstract
Relatively rare, Rasmussen encephalitis is a chronic inflammatory disease conditioning a single cerebral hemisphere. It is a progressive pathology with different stages clinically and on MRI. Therefore, imaging has an important role in evoking the diagnosis and also excluding other possible etiologies. We report a case of Rasmussen encephalitis with 2 different stages on MRI and also provide a review of the role of imaging in diagnostic criteria, differential diagnoses, and stages of this pathology.
Introduction
Rasmussen encephalitis is a chronic localized encephalitis, characterized by a progressive and unilateral cerebral inflammation of uncertain etiology. 1 It manifests most of the time by drug-resistant partial epilepsy, progressive hemiplegia, and cognitive decline depending on the disease stage. 2 Imaging is the examination of choice to evoke the diagnosis.
We report the case of a 5-year-old girl initially admitted for refractory epilepsy for 8 months with a normal MRI. The patient returned after 6 months with a left hemiparesis with her MRI then showing typical aspects of Rasmussen encephalitis.
Case Report
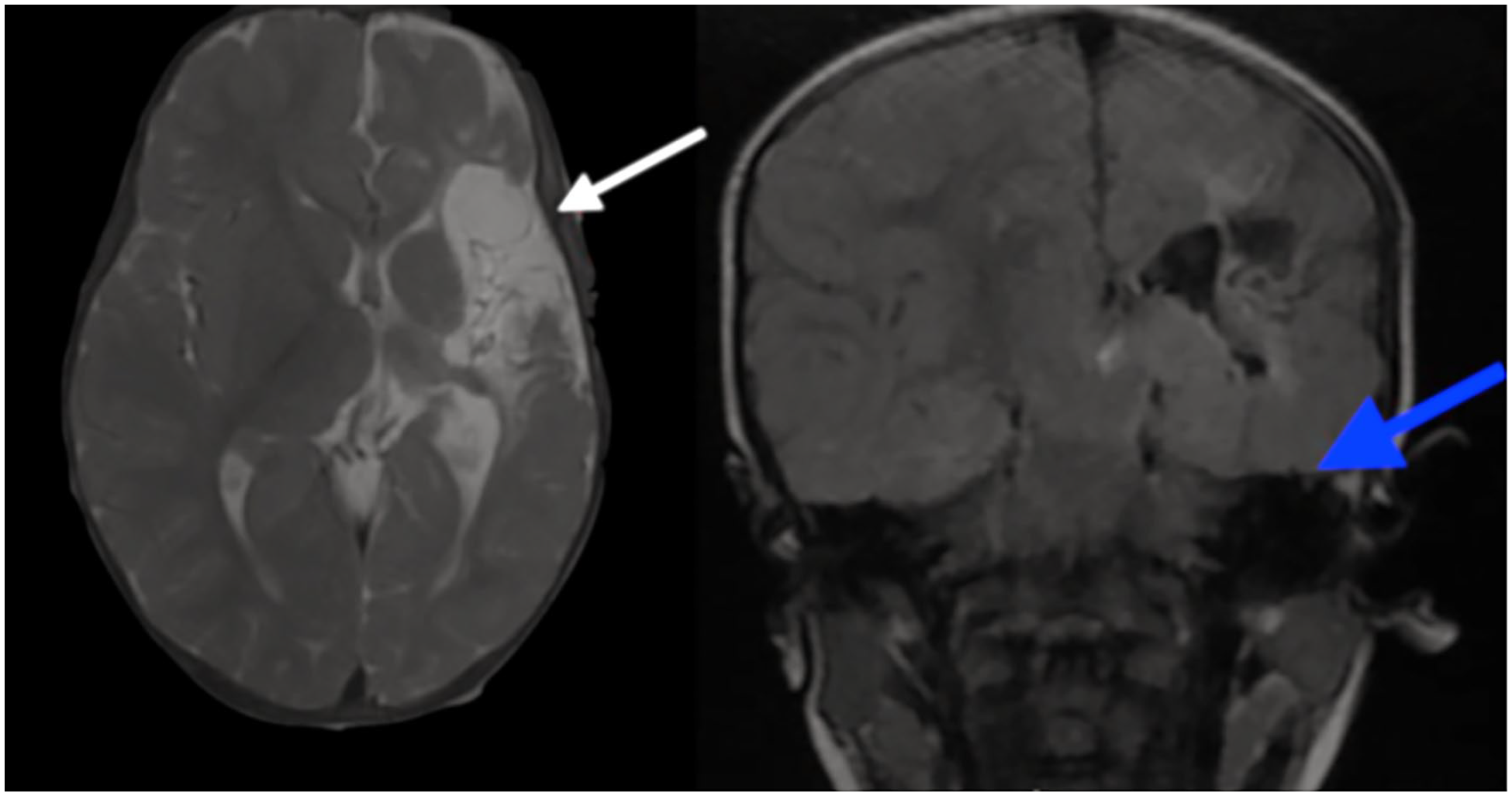
A 5-year-old girl with no particular medical history and a normal perinatal period and developmental milestones, first presented to the pediatrics department with refractory epilepsy for 8 months. It started with clonic movements of the left leg and hand for 2 months which later on progressed to continuous partial seizures refractory to monotherapy. The patient first underwent a brain MRI which turned out to be normal (Figure 1). The infant was then put on triple therapy with no further investigations. Six months later, our patient returned with left hemiparesis. On examination, the left lower and upper limbs showed decreased tone and power (2/5). The brain MRI then showed right cortical hemiatrophy with T2 and FLAIR hyperintense signal in the right para sagittal frontal area, with no restricted diffusion or post-Gadolinium enhancement (Figures 2 and 3). At the same time, those findings were associated with atrophy of the right hippocampus with dilatation of the choroidal fissure (Figure 4).

(a and b) axial FLAIR and (c) axial T1 Gadolinium FS sequences of our patient showing no abnormalities or pathologic enhancement.
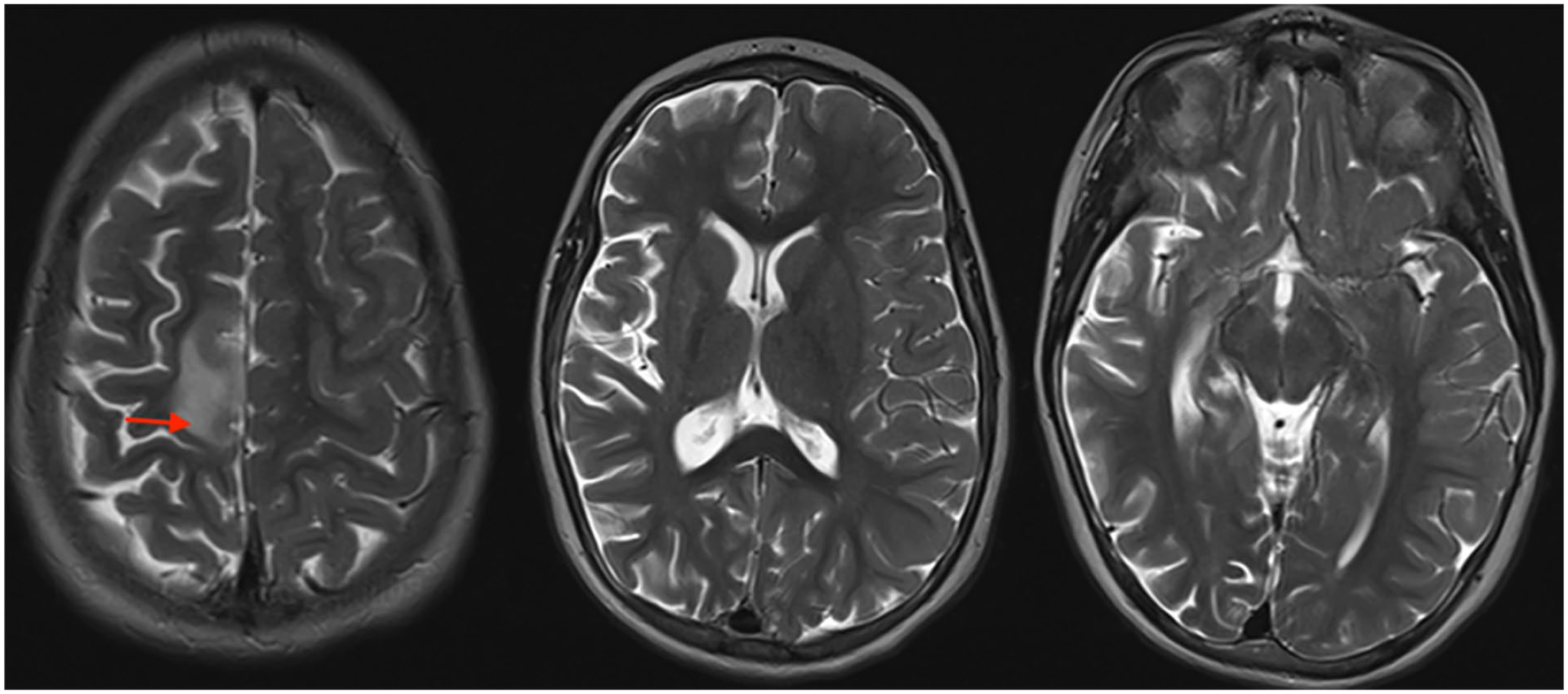
Axial T2 weighted images showing enlargement of the subarachnoid spaces in the right cerebral hemisphere associated to a discreet enlargement of the ipsilateral lateral ventricle in favor of cerebral hemi atrophy.
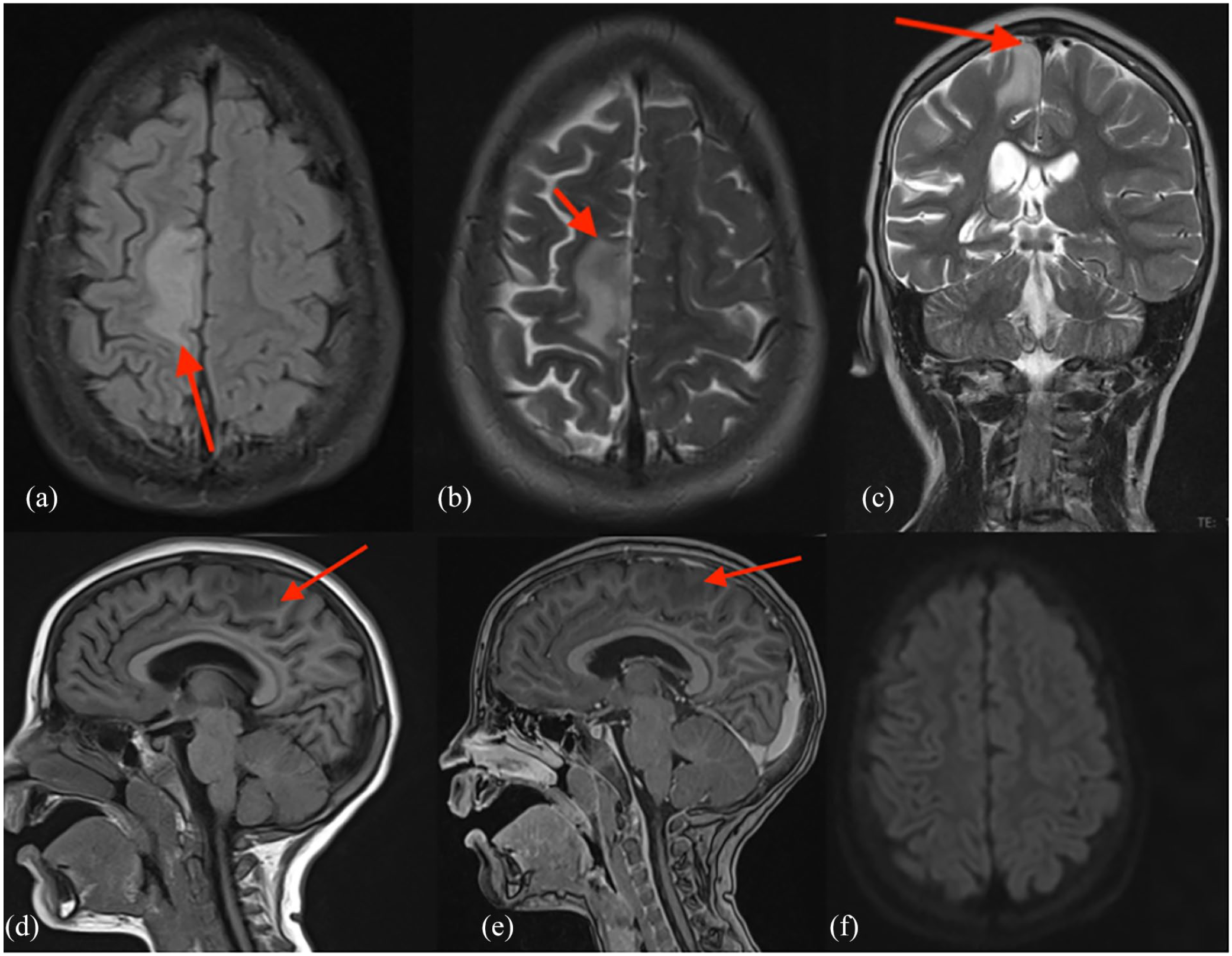
(a) Axial FLAIR, (b) Axial T2, (c) Coronal T2, (d and e) sagittal T1 before and after Gadolinium and diffusion weighted images showing T2 and FLAIR hyperintense signal in the right para sagittal frontal area, with no restricted diffusion or post-Gadolinium enhancement (red arrow).

Axial and coronal T2 weighted images demonstrating atrophy of the right hippocampus (white arrow) with dilatation of the choroidal fissure (blue arrow).
Electroencephalogram (EEG) demonstrated background slowing activity and a marked asymmetry of the tracing.
Discussion
Rasmussen encephalitis is a chronic localized encephalitis of uncertain cause affecting one brain hemisphere (half) progressively. It usually begins in childhood between 6 and 8 years. It was first reported by the American neurologist Theodore Brown Rasmussen in 1958 when he suggested a viral etiology in his original paper. 3 Nevertheless, no significant signs of viral infections were neither excluded nor confirmed with inflammation, gliosis and loss of neurons being all found histopathologically. 1 Clinically, this disease is characterized by refractory epilepsy followed by progressive hemiparesis or cognitive decline which describes 3 phases (Figure 5).
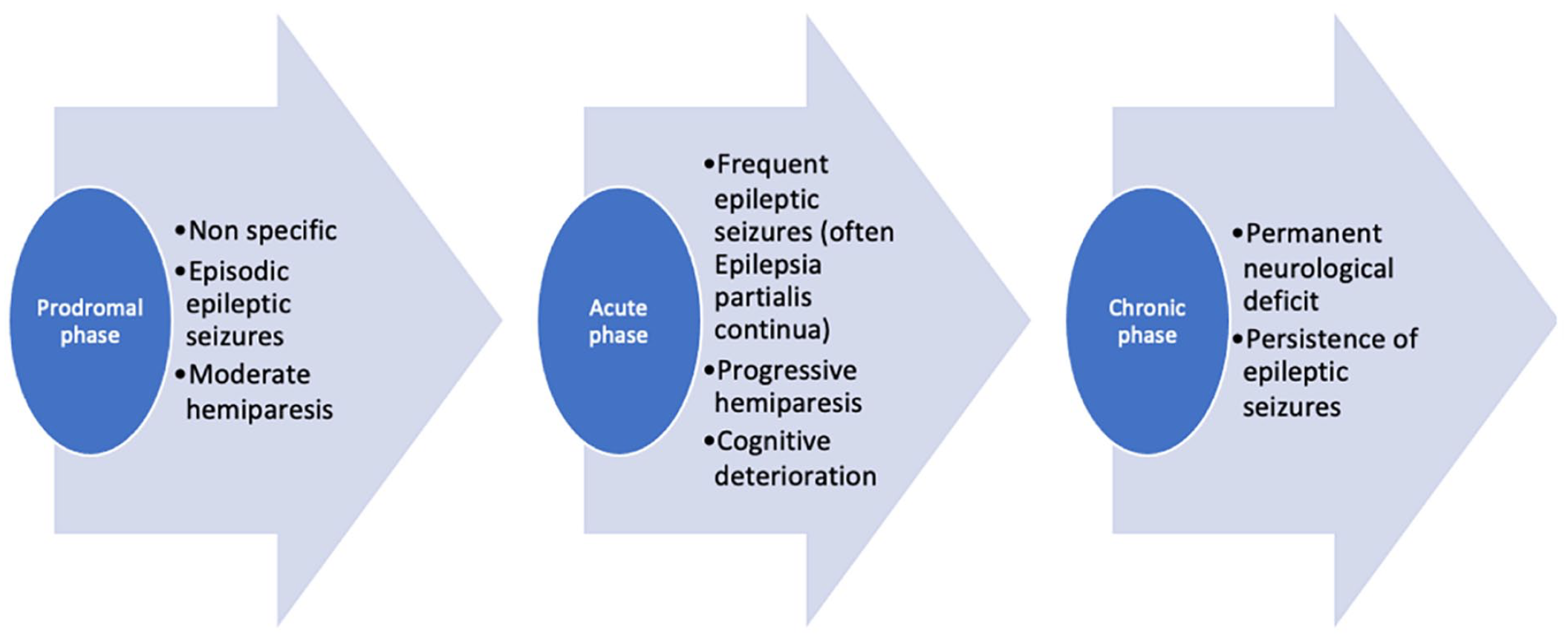
Phases of clinical symptoms of Rasmussen encephalitis.
MRI is the imaging of choice in evoking the diagnosis and findings vary with the disease stage. 4 Initially, unilateral focal cortical swelling may be seen. With time, T2/FLAIR hyperintensity develops in the cortex and subcortical white matter of the involved side (Figure 3). With the disease progressing into chronic stages, we may witness unilateral cerebral and basal ganglia atrophy. In the final phase, hyperintensities may disappear, leaving a marked hemi cerebral atrophy. Those stages were proposed by Bien et al based on a retrospective study on 10 patients and their MRIs (initial and follow-up) and focus essentially on T2 sequences 5 (Figure 6).

MRI stages of Rasmussen encephalitis proposed by Bien et al.
We can conclude that our 5-year-old infant was probably in the prodromal phase when she presented seizures for 2 months with the first MRI being normal. Our patient then installed hemiparesis which means she was in the chronic phase with the MRI showing hemi cerebral atrophy and an area of T2/FLAIR hypersignal which matches stage 3.
Electroencephalogram (EEG) findings are mostly related to disease progression. No specific abnormalities differentiate Rasmussen’s encephalitis from other focal epilepsy etiologies. Initially, EEG is often normal with persistent high-amplitude activity developing in the affected areas within months of seizure onset. Ep-ileptiform abnormalities can also be found with background slowing activity. In some cases, other interictal abnormalities in the non-atrophied hemisphere may emerge within 6 months (in 25% of patients). However, these contralateral EEG findings do not seem to be indicative of bilateral disease even though they can be a marker of cognitive decline.1,6
Cerebral hemiatrophy has other causes such as Dyke–Davidoff–Masson syndrome (DDSM), hemi-megalencephaly, and Sturge-Weber Syndrome, with them all generally associated with hemiplegia and epilepsy. Some clinical and MRI findings are of great help in differentiating these etiologies from RE (Table 1).
Main differential diagnosis with particular clinical and imaging findings.

Axial T2 weighted images (left) and coronal FLAIR (right) showing thickening of the skull vault (white arrow) with left hemi cerebral atrophy and ipsilateral ventricle dilation associated to the elevation of the petrous ridge (blue arrow).

Axial and coronal T2 weighted images of a 1-year-old girl diagnosed with hemimegalencephaly in our department. It shows enlargement of the left hemisphere, contralateral displacement of the posterior falx and enlarged ipsilateral ventricle (red star). Note the pachygyria and abnormal gray-white matter differentiation diffusely (white arrows).
As for the treatment of Rasmussen encephalitis, antiepileptics have a limited effect on epilepsy as well as the progression of the disease, since it tends to be refractory to these drugs. Thus, the main goal of drug therapy is to protect the patient from severe seizures. Whereof, surgery remains the only definite cure for epilepsy caused by this disease. It is based on the complete disconnection of the atrophied hemisphere (hemidisconnection), either as (functional) hemispherectomy or hemispherotomy. 13 Our patient had also been scheduled for surgery in the upcoming weeks.
Conclusion
Rasmussen’s encephalitis remains a rare pathology which can be a diagnostic dilemma for some physicians. We should always evoke ER in front of an elevated frequency of complex partial seizures with a post-ictal deficit in patients between 1 and 15 years old), especially when associated with a “normal” initial imaging and a disease progression marked with drug-resistant epilepsy with progressive atrophy of a hemisphere and areas of T2 hypersignal. Thus, MRI findings can be highly suggestive of Rasmussen Encephalitis diagnosis and also in excluding other causes of cerebral hemiatrophy.
Footnotes
Acknowledgements
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Author Contributions
ELY: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. LK: Contributed to conception and design; Con-tributed to analysis; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. BN: Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA and LC: critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SEL: Contributed to acquisition, analysis, or interpretation; Critically revised the manuscript; Gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the parents of patients for the publication of this case report.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Guarantor of Submission
The corresponding author is the guarantor of submission.