
Abstract
Rhinoscleroma is a rare benign granulomatous disease in children, the pathogen of which is Klebsiella rhinoscleromatis. Rhinoscleroma almost always affects the respiratory tract, the nasal cavities are the most common site, but can also be found over the entire extent of the respiratory tree, clinically the patient often presents with nasal obstruction with other non-specific signs, Histology is the basis of the diagnosis of rhinoscleroma. Early and appropriate medical treatment improves the prognosis and prevents progression to disabling sequelae. We present the case of a 9-year-old child who presented to the pediatric emergency department with a 2-month history of nasal obstruction unresponsive to medical treatment (Oxymetazoline). This was accompanied by mild nasal swelling and intermittent episodes of epistaxis. A CT scan of the paranasal sinuses was performed, ruling out a malignant tumor in the nasal cavity due to the absence of bone lysis. A nasal cavity biopsy with histopathological examination was conducted, confirming the diagnosis of rhinoscleroma. This was supported by the presence of an infiltrate rich in histiocytes and plasma cells, along with the identification of Russell bodies during PAS (Periodic Acid Schiff) staining. The patient underwent a medical treatment regimen involving a sulfamide-based antibiotic therapy (trimethoprim/sulfamethoxazole) for 8 weeks, along with a short-term corticosteroid therapy at a dose of 1 mg/kg/24 hours. At the first follow-up after 1 month, there was a noticeable reduction in nasal swelling and an improvement in nasal obstruction. A second follow-up 3 months later showed favorable results, with complete disappearance of both the swelling and nasal obstruction. Considering the possibility of recurrence, an annual follow-up was decided upon.
Introduction
Rhinoscleroma is a rare and chronic granulomatous condition that progresses insidiously and slowly. It primarily develops within the nasal passages in 95% of cases, 1 but it can also localize in other sites of the respiratory tract. Its causative agent is Klebsiella rhinoscleromatis1, a Gram-negative coccobacillus with an affinity for the upper airways. 2 It is a specific condition characterized clinically by a pseudo-tumoral evolving granuloma, and histologically by the presence of Mikulicz cells. 2 Diagnosis sometimes presents a challenge, with confirmation relying solely on histological examination. Its treatment is primarily medical. 13
Case Report
We present the case of a 9-year-old child who presented to the pediatric emergency department with a nasal obstruction persisting for 2 months, unresponsive to medical treatment (Oxymetazoline). A slight nasal swelling and a few episodes of epistaxis appeared. A CT scan of the paranasal sinuses was performed, ruling out a malignant tumor in the nasal cavity due to the absence of bone lysis (Figures 1 and 2).
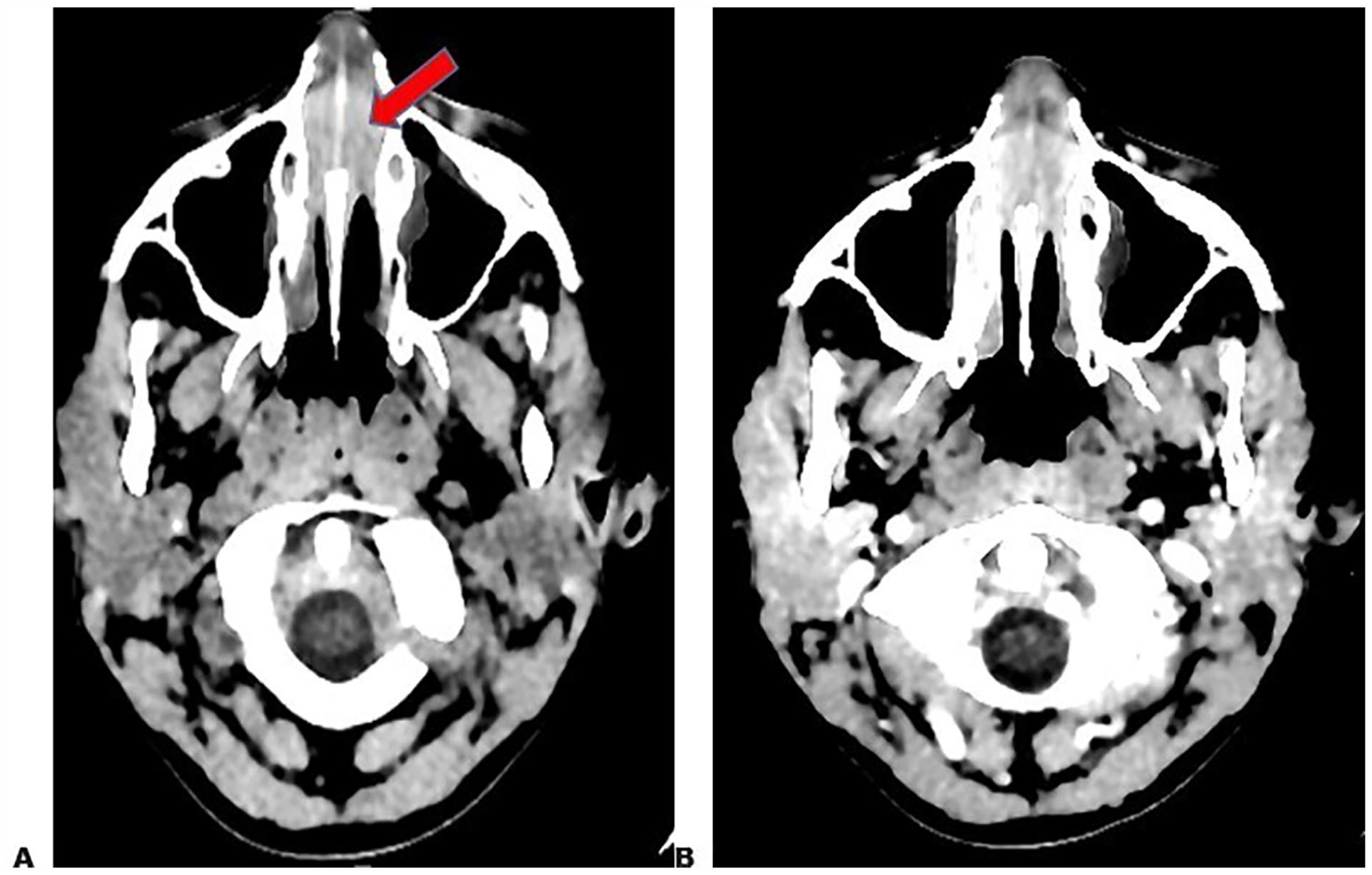
CT scan of the paranasal sinuses axial section (A): without injection A showing a spontaneously hyperdense tissue lesion process centered on the nasal cavity, (B) With injection: showing the weak enhancement in a homogeneous way after injection of contrast product of the process.

CT with a bone window confirms the absence of bone lysis.
A nasal cavity biopsy with histopathological examination was conducted, confirming the diagnosis of rhinoscleroma through the observation of an infiltrate rich in histiocytes and plasma cells, along with the presence of Russell bodies as visualized by PAS (Periodic Acid Schiff) staining (Figure 3).

Histology ((A) HEX10, (B) HEX20) showing an edematous nasal mucosa largely remodeled by an inflammatory infiltrate rich in histiocytes and plasma cells, (C) Histology: PAS staining shows RUSSEL courses and particle-laden histiocytes.
The patient underwent a medical treatment regimen, combining sulfamide-based antibiotic therapy (trimethoprim/sulfamethoxazole) for 8 weeks and a short-term corticosteroid therapy at a dose of 1 mg/kg/24 hours.
At the first follow-up after the treatment period, there was a notable reduction in nasal swelling and improvement in nasal obstruction. A second follow-up 3 months later showed favorable results, marked by the complete disappearance of swelling and nasal obstruction.
Given the likelihood of recurrences, an annual follow-up was decided upon.
Discussion
Rhinoscleroma is a rare granulomatous condition triggered by enterobacteria from the Klebsiella family (Klebsiella rhinoscleromatis). 1 Its occurrence in children is exceptionally rare, which can give rise to challenges in achieving a positive diagnosis. Therefore, it’s essential to consistently consider this condition when encountering any centrofacial granuloma in endemic areas.
Rhinoscleroma predominantly impacts the respiratory system, with the nasal cavities being the most commonly affected site. However, it can extend throughout the entire respiratory tract, reaching as far as the bronchi. 2
Although it is becoming increasingly rare, rhinoscleroma still persists as an endemic condition in certain regions of Africa (such as Egypt and tropical zones), Southeast Asia, Mexico, Central and South America, as well as Central and Eastern Europe. 3 Only a few sporadic cases have been reported in Western Europe, likely resulting from the migration of individuals from endemic areas. 4
Communities with lower socioeconomic status are disproportionately affected due to inadequate hygiene, nutritional deficiencies, and weakened immune systems, which are the primary contributing factors. 5
The exact mode of infection is not well-defined, but the occurrence of multiple cases within the same family could lend support to the hypothesis of transmission through close and prolonged direct contact3. Rhinoscleroma primarily affects young adults in their third and fourth decades of life (85% of cases), 3 with a 60% predominance among female cases. 6
Rhinoscleroma appears to be increasingly rare in Morocco, being more common in regions with dry or semi-desert climates and among disadvantaged socioeconomic groups. It is systematically considered when faced with any centrofacial granuloma.
A case of a child with rhinoscleroma in Morocco has not been found in the literature.
In our case, the child comes from an underprivileged family residing in a city with a dry climate.
Three phases characterize the evolution of rhinoscleroma, it begins in the form of a crusty chronic rhinitis, fetid with nasal obstruction, and generally lasts from weeks to months, then develops a granulomatous formation essentially in the anterior part of the nasal cavity hard from the months to years. 7 Finally, the evolution is scarring leading to a stenosis of the nostrils 3, It is a disease with very slow evolution over many years, which can lead to advanced stages, nasal deformities, anosmia, oral anesthesia, dysphonia, dysphasia and stridor. 7 Fortunately, in our case, the child underwent an early-stage CT scan, which prompted the decision to perform a biopsy to establish a diagnosis.
Radiological imaging is essential for early diagnosis of rhinoscleroma, differentiation of rhinoscleroma from similar granulomatous and neoplastic lesions, and detection of disease extensions and complications. 8 In our case, we were able to readily exclude a neoplastic origin of the tumor due to the absence of associated bone lysis.
Imaging is also important for the determination of treatment and follow up post-therapy. 8 In our case, given its early discovery, a decision was made for medical treatment, and the clinical improvement that followed rendered a post-treatment CT scan unnecessary, as it would have provided no useful information while exposing the child to unnecessary radiation.
CT and MRI are the recommended radiological examinations. On CT scan, bilateral or unilateral expanded nasal masses of variable size.8 Characteristic lesions are homogeneous, hyperdense and non-enhancing masses with well-defined borders. 9 Scleroma usually extends into the max-illary sinuses through the ostiomeatal units. 10 Scleroma can also extend into the ethmoid and sphenoid sinus with intracranial extension. 10 It lines the sinus wall causing bone sclerosis, bone thinning (pressure atrophy) or it may absorb it with extramaxillary sinus extension. No bone destruction which helps to differentiate it from malignant lesions. 8 Nasal masses can also obstruct the ostiomeatal units, and secretions may be retained in the related sinuses.
Differential diagnosis before performing the biopsy is essential to rule out a neoplastic cause such as naso-sinus adenocarcinoma or lymphoma, which can be easily ruled out on CT due to the absence of bone lysis. 11
The other differential diagnoses are other infectious granulomatous diseases such as tuberculosis, mucocutaneous leishmaniasis, etc. And non-infectious diseases such as sarcoidosis. 11
Histology is the basis of the diagnosis of rhinocleroma, it shows an inflammatory infiltrate rich in histiocytes and plasma cells with the presence of mikuliz cells and russell bodies. 12
The therapeutic management of rhinoscleroma is primarily medical, centered around extended systemic antibiotic therapy for several months, 13 coupled with thorough nasal cleaning using saline solution. Currently, rifampicin and fluoroquinolones stand as the most effective treatments due to their high concentration within macrophages. The optimal treatment duration has not been definitively established, varying between 6 weeks and 6 months according to different authors. In our case, a 2-month treatment proved sufficient. Generally, the goal is the sterilization of the infectious focus.
Generally, sterilization of the infectious focus is achieved around the third month. 14 Other antibiotics are also effective, but due to their cochleo-vestibular or hematological toxicity, they are used less frequently: streptomycin, cotrimoxazole, oxytetracycline, and sulfonamides. 14 Iron therapy is occasionally administered in cases of anemia. Corticosteroid therapy can be employed to mitigate the sclerotic process. Recurrence is common, occurring in 41% of cases between 1 to 3 years 3 . After 6 months in our patient’s case, no local recurrence was observed following treatment cessation. Surgical intervention is considered for fibrosclerotic lesions, aiming to restore nasal passages permeability and calibration.
Conclusion
Rhinoscleroma is a condition that appears to be increasingly rare. Its occurrence in children is exceptional, which can create challenges in achieving a positive diagnosis. Hence, it is important to consistently consider this diagnosis when faced with any centrofacial granuloma in endemic regions. Early diagnosis, appropriate treatment, and rigorous, extended monitoring are necessary to eradicate this infectious disease and prevent de-bilitating consequences.
Footnotes
Author Contributions
All authors contributed equally to this work
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.