
Abstract
Regular physical activity (PA) is essential in cystic fibrosis (CF). This study assessed the impact of a motivational interviewing (MI)-based project titled “Just move it . . . move it,” aimed at improving the PA of pediatric CF patients. At baseline and month 6, body mass index, spirometric values, and duration of extracurricular sport activities were collected. Concurrently, the maximum oxygen uptake (VO2max) was estimated. MI was performed during each visit. Overall, 19 CF children were included. Ten patients (52.7%) increased their regular PA (mean 1.9 hours/week) between both visits (PA+ group), while 9 did not (PA− group). No significant differences in functional and nutritional values were observed between the groups, while extracurricular sport time significantly increased in the PA+ group. “Just move it . . . move it” seems to be an efficient approach, as it was able to motivate several CF patients to initiate or increase their PA, yet without improving functional parameters.
Introduction
Cystic fibrosis (CF) is the most prevalent inherited genetic disorder in the Caucasian population. 1 The condition is caused by a mutation in a single gene that encodes the cystic fibrosis transmembrane conductance regulator protein (CFTR). The absence or dysfunction of this protein results in an abnormally thick and viscous mucus. Although CF affects many different organ systems, its most serious consequence is a progressive deterioration of pulmonary function. Despite marked improvements in CF therapeutic management, pulmonary disease is still associated with increased morbidity and mortality. The second organ most affected by the condition is the pancreas with malabsorption of dietary fat and proteins, resulting in chronic undernutrition and poor growth. Both declining pulmonary function and malnutrition lead to physical exercise intolerance.2,3 Regular physical activity (PA) is an essential component in the therapeutic management of CF patients, which seeks to improve their pulmonary function, physical status, and even survival.1,4 Indeed, regular exercise training brings about improvements in ventilatory-muscle endurance, involving both aerobic and anaerobic capacity, and sputum clearance. By these means, regular exercise prevents the decrease in bone mineral density and enhances mental well-being.1,4,5 Furthermore, evaluating exercise tolerance is indicative of the cardio-respiratory status of CF patients, including their functional capacity, quality of life, and prognosis. 6 Despite the benefits of PA for CF children, only few of them regularly practice a sport, whereas they still have a good lung function.1,5 There are several explanations for this, including exercise intolerance secondary to nutritional status, reduced muscle size and strength, deficiency in aerobic and anaerobic capacity, as well as a lack of time to devote to sport, due to the amount of time that is taken up by the treatment. In addition, as some CF patients are regularly hospitalized, it is difficult for them to follow a regular PA. In comparison with healthy children, economic factors, social factors like habits of family life, and psychological factors like apprehension or anxiety constitute other barriers. Behavioral strategies like motivational interviewing (MI) are likely interesting to promote PA in young CF patients.7,8 Indeed, MI is a communication method that is based on partnership building, empathy, and interpersonal sensitivity, as well as exploration of personal values, interests, and concerns. MI strategy is centered on fully supporting the patient’s autonomy and collaboration, in addition to evocating the patient’s concepts regarding change. 8 It is now considered to be a counseling approach that is designed to promote behavior change, which has been reported to be effective and associated with low-intensity intervention and low-cost strategy. 9 To explore the motivations and obstacles at each level, whether medical, psychological, or social, MI can be applied by a multidisciplinary team. Operationally, the health care professional uses open-ended questions, reflective listening, affirmation like compliments, while eliciting change talk.
The purpose of this pilot study was to evaluate the impact of a multidisciplinary project titled “Just move it . . . move it” focused on PA of pediatric CF patients followed-up in our center. This MI project has been developed in order to undertake or increase CF patients’ PA, with their effects on nutritional and functional parameters studied as well.
Method
Study Design and Patients
This was a longitudinal prospective pilot study including CF children aged between 6 and 15 years and attending the pediatric CF center of the Brussels Free University, Belgium. The patients were included during a period of 2 months on the occasion of their follow-up visit. The patients with a medical contraindication to practice a sport, including hypoxemia, post-pneumothorax status severe, hemoptysis, or osteoarticular abnormalities, were excluded from participation. The study was integrated into the regular patient follow-up, scheduled to take place every 6 weeks, which included 3 follow-up visits. The first consisted of a routine visit to explain the project. Following the signing of patient or parental informed consent forms, the second visit was performed at starting the practice of sport (T0), and the third took place at month 6. The body mass index (BMI) and spirometric values, including forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and 25% to 75% forced expiratory flow (FEF) were collected, along with the duration of extracurricular PA (hours/week). Data were expressed as z-scores based on GLI-2012 reference.
10
An incremental shuttle test (IST) was performed at T0 and month 6 in order to assess maximum oxygen uptake (VO2max). A variety of tests was applied to evaluate the children’s physical status. Cardiopulmonary exercise testing (CPET) is considered the gold standard, yet it requires expensive equipment and specialized personnel.3,11 Therefore, IST may be a good alternative, given that it is simple, inexpensive, and reliable.6,12 In this study, we performed a 15 m IST, conducted in an enclosed corridor on a flat 15 m-long course. Patients were instructed to run around 2 cones following the rhythm dictated by the audio signal. Subjects had to run at the prompting of a sound at regular intervals, to reach the next pole before the next sound goes on. The 15 m IST has 17 levels. Each level includes an increasing number of shuttles and the speed therefore increases as the level advances. The 15 m test begins with a running speed above 7.71 km/hour at Level 1 and ends with a speed of 12 km/hour at Level 17. The end of the test is determined by the patient, when he/she becomes unable to maintain the required speed, or by the experimenter if the patient fails to complete a shuttle during the time allowed. Different parameters (oxygen saturation, heart rate, and respiratory rate) are documented before, just after, and 3 minutes later the beginning of the test. This test evaluates aerobic fitness in a maximal effort. A correlation between the test performance and VO2max can be extrapolated and permits to evaluate the cardiorespiratory status of the patients. We estimated the VO2max using the Matsuzaka equation
13
: VO2max (mL/minutes/kg) = (25.9 − 2.21 × G) − 0.0449 × A − 0.831 × Y + 4.12 × MS; G = 0 for boys and G = 1 for girls; A = age in years; Y = BMI; and MS = maximum speed.
To evaluate the project’s effects on nutritional and functional parameters, the patients were classified into 2 groups depending on the PA increases: a first group without change (PA−) and second group with a minimum increase of 1 hour/week (PA+).
The “Just Move It . . . Move It” Project
All CF team members (physiotherapist, dietician, psychologist, social worker, nurse, and pediatric pulmonologists) participated in this project. They underwent MI training and then applied this method during each CF patient visit. The physiotherapist explained PA usefulness and presented different sports accessible to CF patients. The motivations and barriers to the practice of sport were discussed with the CF children and their parents, and solutions were then found to undertake or increase PA. The physiotherapist also performed an IST with the patients. The dietitian provided advices on hydration and nutrition during sports, and also participated to the IST in order to motivate the patients. The psychologist identified potential psychosocial barriers to PA. The nurse reinforced the patients’ motivation during lung function testing. Thereafter, once a sport activity had been chosen, the social worker looked for sports clubs near the child’s house or school and proposed financial assistance, in collaboration with the CF Association, as necessary. Finally, pediatric pulmonologists reviewed the medical approach and sports’ usefulness in terms of physiology and well-being, while using a motivational approach, as well.
In collaboration with parents and CF patients and using the MI, each CF team member attempted to change the patient’s behavior. The team primarily focused on the individuality and relevance of finding pleasure in PA. Indeed, providing individually designed exercise programs for CF patients appears essential, whatever their disease severity. PA should be viewed by the children as both fun and therapy.
This study was approved by our hospital’s ethics committee (CEH no. 29/13).
Statistics
The statistical analyses were conducted using SPSS Statistics, Version 15.0. Mann-Whitney testing was employed to compare anthropometric, spirometric, and performance values between both groups. A Wilcoxon test was carried out to compare these values before and after MI within each group. A Fisher’s exact test was employed to compare gender and pancreatic insufficiency between the 2 groups.
Results
Among the 70 patients followed in our referral center, 36 were eligible to participate in the study. We proposed the project to all patients coming at the follow-up consultation during 2 months. No patient refused to participate to the project. Overall, 19 children were included in the study, 9 of whom were girls (58%), and the group’s median age was 10 (6-15 years). No children had a medical contraindication to practice a sport. The patient clinical characteristics and their extracurricular sports times are listed in Table 1. The sport activities practiced by the CF children followed-up at our center included swimming, tennis, badminton, climbing, dance, athletics, hockey, basket, aikido, and biking. Nine children exhibited a FEV1 <80% (47%). At T0, the median estimated VO2max and time of extracurricular PA were 47.6 ± 3.2 mL/kg/minutes and 1.5 ± 1.6 hours/week, respectively. No patient was on CFTR modulator therapy.
Patient Characteristics at the Initial Visit (T0).
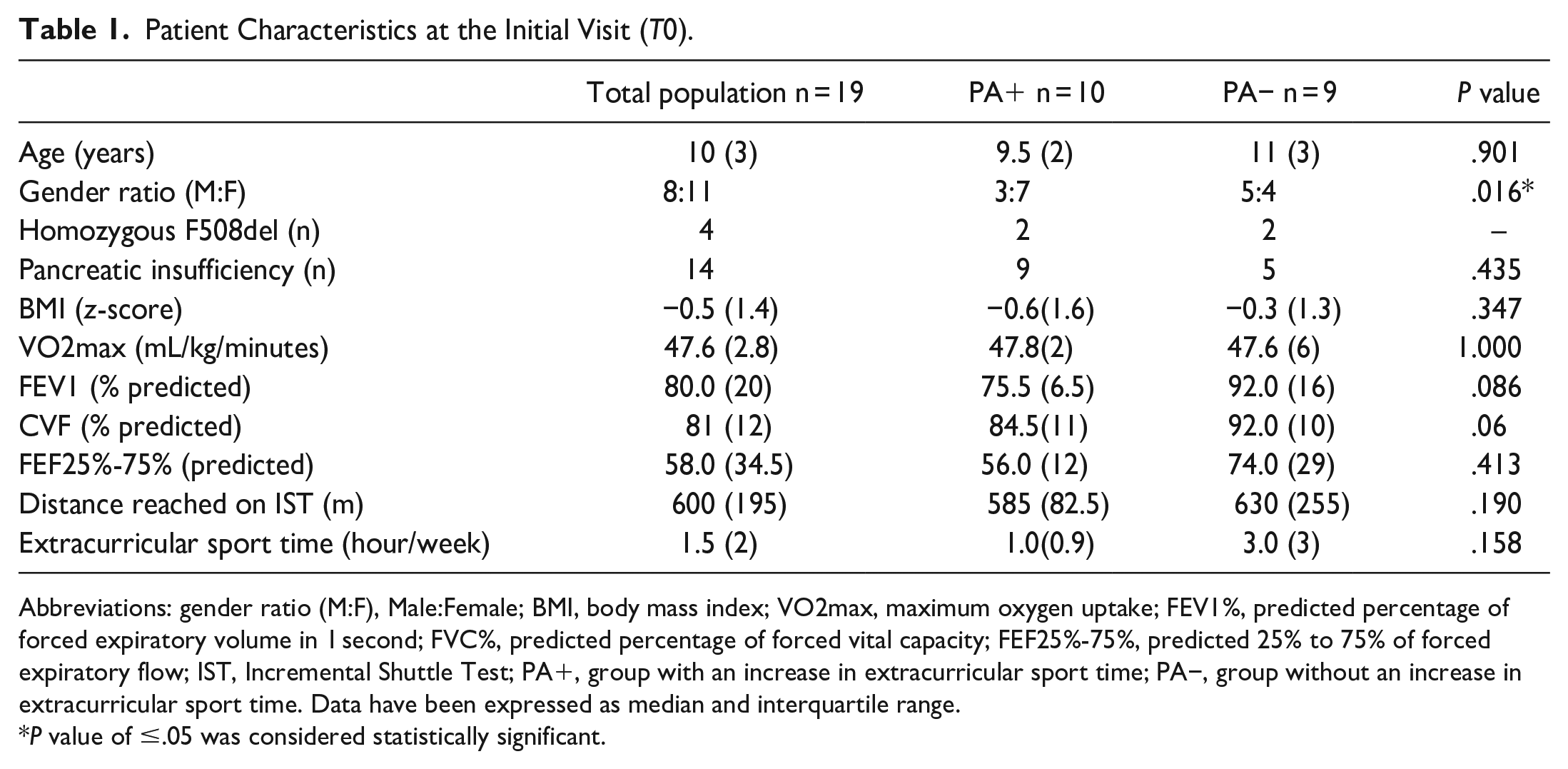
Abbreviations: gender ratio (M:F), Male:Female; BMI, body mass index; VO2max, maximum oxygen uptake; FEV1%, predicted percentage of forced expiratory volume in 1 second; FVC%, predicted percentage of forced vital capacity; FEF25%-75%, predicted 25% to 75% of forced expiratory flow; IST, Incremental Shuttle Test; PA+, group with an increase in extracurricular sport time; PA−, group without an increase in extracurricular sport time. Data have been expressed as median and interquartile range.
P value of ≤.05 was considered statistically significant.
Ten patients (52.7%) increased their regular PA (mean 1.9 hour/week) between T0 and month 6 (PA+), and they were compared with the 9 patients without any PA improvement (PA−). The characteristics of both groups according to the PA at T0 are summarized in Table 1.
We observed a statistically significant difference between the PA+ and PA− groups in terms of gender, whereas no significant between-group differences were observed concerning BMI, spirometric values, and VO2max. However, children belonging to the PA− group spent more hours on extracurricular sport activities than did those of the other group, although the between-group difference was not statistically significant.
At month 6, BMI, VO2max, and spirometric values were compared between the PA+ and PA− groups, without any significant difference observed (Table 2). Yet, a statistically significant difference was observed between both groups regarding extracurricular sport time (P = .03; Figure 1). No significant difference was revealed between T0 and month 6 within each group concerning nutritional and functional parameters. On the other hand, a statistically significant difference was noted within group PA+ between T0 and month 6 regarding extracurricular sport time (P = .03).
Patient Characteristics at Month 6.

Abbreviations: BMI, body mass index; VO2max, maximum oxygen uptake; FEV1%, forced expiratory volume; FVC%, predicted percentage of forced vital capacity in 1 second; FEF25% to 75%, predicted 25% to 75% forced expiratory flow; IST, Incremental Shuttle Test; PA+: group with an increase in extracurricular sport time; PA−, group without an increase in extracurricular sport time. Data have been expressed as median and interquartile range.
P value of ≤.05 was considered statistically significant.

Box-whisker plot of extracurricular sport time at T0 and month 6 between PA+ and PA− groups.
Discussion
This study sought to evaluate if the “Just move it . . . move it” project was able to get our CF patients to start or increase PA. It was based on the MI approach in addition to multidisciplinary support by each CF team member. Using this approach, we obtained a significant increase in PA in more than 50% of our patients. Contrary to the literature, we did not observe any effect on nutritional and functional parameters. According to the review article of Stevens and Williams, 2 several studies investigating the effects of exercise training in CF children actually reported increased VO2max values. Among these studies, Gulmans et al investigated the effects of a 6-month home-based cycling program conducted on 14 CF children. The program consisted of 5 ergometer cycling sessions per week, each lasting 20 minutes, with an increase in intensity undertaken over time. Similar conclusions were made in a 12-week randomized, controlled study following an anaerobic training program involving 11 CF children. The training consisted of two 30 to 45 minutes sessions per week of anaerobic exercises, such as sprints, chest passes, exchange runs, and others. 14 The difference with the present project is that these studies included training programs with intense PA. The objective and approach of our project differ. Indeed, our primary objective was to initiate or increase PA of our pediatric CF patients by rendering them aware of PA’s relevance as part of CF treatment through both a motivational and personalized approach. The increase in PA achieved only by increased extracurricular sport time is unlikely to influence the functional parameters and, therefore, a more intensive program should be added to this project. However, the lack of any effect on VO2max can also be explained by the relatively good initial PA and baseline values of our population. Indeed, considering the long time taken up by CF treatment, our patients seem to be rather physically active, as confirmed by their extracurricular sport time and VO2max. Likewise, they seem to be as active physically as other CF populations. Indeed, Nixon et al 5 reported a mean VO2max of 36 mL/kg/minutes in their pediatric CF population. Moreover, a few studies investigated the effects of behavioral counseling intervention like MI in order to increase PA. Among these studies, only 2 sought to increase PA in CF population, 1 using verbal and written guidelines and recommendations for aerobic physical exercises, 15 and the other one by means of counseling sessions. 16 The results are similar for both studies, and they are comparable to ours. They authors actually increased their CF children’s PA, without any relevant improvement in their lung function.
Another observation is that, although more than half of the cohort joined the project, we were unable to observe an increase in extracurricular PA in the entire population. This could be explained by the fact that the PA− group was actually the group with the most extracurricular PA hours at T0, whereas most of the group’s members decreased their PA during the study. For these patients, it might be interesting to further promote PA using a more personalized approach, such as a training program specifically focused on the individual children’s interests and their individually available time for PA. Programs that are shorter in duration but higher in intensity could be more efficacious for these children. Indeed, as CF treatment is already time-consuming, it may be difficult to further increase PA. Finally, to further enhance the adherence to exercise programs, web-based platforms are available and could thus be used, especially by adolescents, as shown in the Cox et al 7 study.
Finally, we observed that there were more girls in the group that increased their extracurricular sport time. This could be accounted for by the observation that girls were usually less active than boys and were less likely than boys to engage in sport activities.17,18 Consequently, they were more inclined to participate in the study than boys, whereas the latter were more active at the first visit.
This study displays some limitations that must be mentioned, such as the small population size, its observational character, as well as its short time length.
Conclusion
This pilot study has suggested our CF population to be physically active, with most of the patients practicing a PA before starting our project. The “Just move it . . . move it” project based on MI seems to be an efficient approach to motivate patients increasing their PA level. However, personalized exercise programs that are well adapted to their everyday life and disease severity should be developed to increase PA and integrated in the management of the CF population.
Footnotes
Acknowledgements
We would like to thank Sidali Namane for his assistance with the statistics; France Burny for her assistance with data collection; Alicia Vandenoetelaer for her participation in the project’s conception; and the Belgian CF Association for their funding support.
Author Contributions
VS: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. VG: contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. VW: contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. KS: contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. CK: contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. LH: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study has received financial support from the Belgian CF Association “L’AssociationMuco.”