
Abstract
In recent years, epidemics of respiratory syncytial virus (RSV) have been seen in the summer in Japan. Patients hospitalized in the summer used a high-flow oxygen administration device more frequently than patients hospitalized in the winter. This study was a retrospective study to examine the variables associated with duration of oxygen therapy and severe cases. Subjects were pediatric patients diagnosed with RSV infection and hospitalized for treatment during the 5 years from April 2014 to March 2019. Data from 292 patients were analyzed. Duration of oxygen therapy was significantly associated with bronchial asthma (partial regression coefficient: 0.897, P = .004). Hospitalization in summer was significantly associated with severe condition (adjusted odds ratio: 4.07, 95% confidence interval: 1.16-14.27). The present study showed that bronchial asthma is a risk factor for prolonged oxygen therapy and infection in summer is a risk factor for progression to severe condition in cases of RSV infection.
Keywords
Introduction
Respiratory syncytial virus (RSV) is an RNA virus that belongs to the pneumovirus genus, Paramyxoviridae family, and causes respiratory infection in infants. 1 Infection is established and symptoms appear in early infancy when there are maternal antibodies. Half of infants develop symptoms by the age of 1 year, and almost 100% by the age of 2. The symptoms become severe in 1% to 3% of patients, requiring hospitalization. 2 Only upper respiratory tract infection results from RSV infection in most infants. 3 However, when lower respiratory tract infection including bronchiolitis and pneumonia occurs, expiratory stridor, prolonged expiration, polypnea, and other symptoms are observed and the condition sometimes becomes severe. 2 It is commonly believed that the epidemic occurs in winter in temperate zones, and mainly in December in Japan, while epidemic levels have recently been seen in summer. 4 The same tendency was observed in Tokyo. 5
In our clinical practice in recent years, patients hospitalized for RSV infection in the summer used a high-flow oxygen administration device more frequently than in the winter because nasal cannula alone did not improve their respiratory symptoms such as tachypnea, effort ventilation, and hypoxemia. Currently, premature infants or children with congenital heart diseases are considered to be at an increased risk for progression of RSV infection to a severe condition and therefore prophylactic palivizumab, an anti-RSV antibody, is indicated for these children in many countries. 6 In response to the recent epidemic of RSV in summer, timing of the administration of palivizumab has been examined in many studies.7,8 However, other risk factors for progression of RSV infection to a severe condition have been investigated in only a small number of studies, and it is difficult to predict how hard the treatment would be in daily clinical practice. In this study, we hypothesized that the timing of hospitalization and the presence or absence of bronchial asthma affects the duration of oxygen therapy in RSV infection, and retrospectively examined the children whose RSV infection required hospitalization for treatment.
Methods
The present study subjects were children who were diagnosed with RSV infection and hospitalized for treatment during the 5 years from April 2014 to March 2019 at Showa University Koto Toyosu Hospital (Tokyo, opened at the end of March 2014, a secondary medical care facility) and they were retrospectively examined. All hospitalized patients during the survey period were listed up, and we extracted those with RSV infection. RSV infection was diagnosed using a rapid antigen kit by immunochromatography. The reasons for hospitalization were either oxygen demand, poor feeding, or fever in children under 3 months of age. We defined the following exclusion criteria: (a) subjects hospitalized more than once, (b) chronic pulmonary disease, (c) cerebral palsy, (d) chromosomal abnormality, (e) congenital cardiovascular malformation with abnormal hemodynamics, (f) patients between the age of 0 and 3 months who required ventilator management by tracheal intubation, (g) 6 years of age and older, (h) patients who were indicated for Palivizumab administration on admission, and (i) missing data.
Based on inpatient medical records, sex, gestational age in weeks, age in months, duration of oxygen therapy, presence or absence of bronchial asthma, and use or no use of a high flow system (high flow nasal cannula or venturi mask) were surveyed. Summer was defined as April through September and winter as October through March of the following year, by diving a year into halves using 14.5°C as the threshold temperature, referring to the mean temperature by month in the past 5 years in Tokyo. 9 Gestational age in weeks was categorized into the following 3 groups according to the cutoff ages for administration of palivizumab: <29 weeks, 29 to <36 weeks, and ≥36 weeks. At our hospital, oxygen therapy is started when oxygen saturation as measured using pulse oximetry (SpO2) is decreased to 93% or lower, and the physicians in charge determine the discontinuation timing, considering changes in SpO2, auscultation findings, systemic condition, and other factors. Presence of bronchial asthma was defined as ongoing treatment for wheezing that recurred more than 3 times based on the diagnosis by physicians in charge. A high flow system was introduced when the modified pulmonary index (mPI) 10 was 10 points or higher and the physicians in charge determined that it was necessary. Selection of a device was left to the physicians in charge depending on the circumstances. The use of a device meant that oxygen therapy alone did not maintain oxygenation or improve respiratory status.
In our study, the duration of oxygen therapy was used as an index for treatment duration. In addition, we defined a disease as severe if it met all of the following criteria: (a) a need for oxygen to maintain SpO2 ≥93%; (b) duration of oxygen therapy ≥6 days, corresponding to or above the 75 percentile limit for all hospitalized children with RSV infection; and (c) need for a high flow system. In order to evaluate factors associated with 2 outcomes, duration of oxygen therapy and progression to severe condition, we performed the following analysis. Multiple linear regression analysis was conducted to investigate the variables associated with duration of oxygen therapy and logistic regression analysis was conducted to assess variables related to whether the disease was severe. In the multiple regression analysis, we selected gestational age, age of the time of hospitalization (months), sex and bronchial asthma as explanatory variables because preterm birth, lower age, gender, and bronchial asthma are already known risk factors.11,12 In addition, hospitalization season (summer or winter) was included as an explanatory variable in the model to determine the relationship between hospitalization season and duration of oxygen therapy. In the logistic regression model, to investigate the association between hospitalization season and severe condition, bronchial asthma, which is clinically important for progression to a severe condition, was selected as an explanatory variable due to the small number of patients with severe condition. P < .05 was considered statistically significant. JMP® ver 15.0 (SAS) was used for statistical analysis. This study was reviewed and approved by the institutional review board of Showa University Koto Toyosu Hospital (Institutional Review Board Approval Number, 18T7032).
Results
A total of 367 pediatric patients (with overlap, 210 boys and 157 girls) were admitted to this hospital with a diagnosis of RSV infection during the 5 years from April 2014 to March 2019. Among these, 17 subjects were hospitalized more than once (15 subjects were hospitalized twice and 1 subject was hospitalized 3 times).
Among 350 patients with no overlap, 8 patients who had an underlying disease of chronic pulmonary disease, cerebral palsy, or chromosomal abnormality, 2 patients between the age of 0 and 1 months who required ventilator management by tracheal intubation, 6 patients who were indicated for palivizumab at the time of admission, and 42 patients who had missing data were excluded and finally, 292 patients (172 boys and 120 girls) were analyzed.
Changes in the number of hospitalized patients by month of admission are shown in Figure 1. The number of hospitalized patients was greater in winter than in summer in fiscal year 2014. In contrast, the number of hospitalized patients has been greater in summer than in winter in 2015 to 2019.

Number of patients admitted to this hospital for RSV infection by month.
Ages of our study subjects ranged from 0 months to 4 years and 6 months. One hundred and two subjects (34.9%) were younger than 6 months old, 79 (27.1%) were aged 6 months or older and younger than 1 year old, 91 (31.2%) were 1 year old, and 20 (6.8%) were 2 years or older. Twenty-three subjects (7.9%) had bronchial asthma and 26 (8.9%) were treated using high flow systems. Of those 26 subjects, 20 were classified as severe.
The characteristics of the subjects are shown in Table 1 by condition and subject characteristics are shown by hospitalized season (summer or winter) in Supplemental Table 1.
Characteristics of Subjects.

Values denote median (25th percentile, 75th percentile) or n (%).
Mann-Whitney’s U test, Pearson’s chi-square test, or Fisher’s exact test was applied as a statistical method.
There were no significant differences in the age at the time of hospitalization, proportion of boys and girls, gestational age, or proportion of asthma patients between those with and without severe condition. The number of hospitalized patients in summer was greater than in winter. Subjects hospitalized in summer tended to require oxygen therapy for a greater number of days and to be treated by high flow systems than those hospitalized in winter. The factors related to the duration of oxygen therapy in patients with RSV infection were examined (Table 2). The presence of bronchial asthma was significantly associated with the duration of oxygen therapy (partial regression coefficient; 0.897, P = .004). Age at the time of hospitalization, sex, hospitalization season, and gestational age were not significantly associated with the duration of oxygen therapy. Variables associated with severe condition were evaluated (Table 3). Hospitalization season (summer) significantly increased the odds ratio (OR) for severe condition (OR: 4.07, 95% confidence interval: 1.16-14.27).
Variables Associated With Duration of Oxygen Therapy.
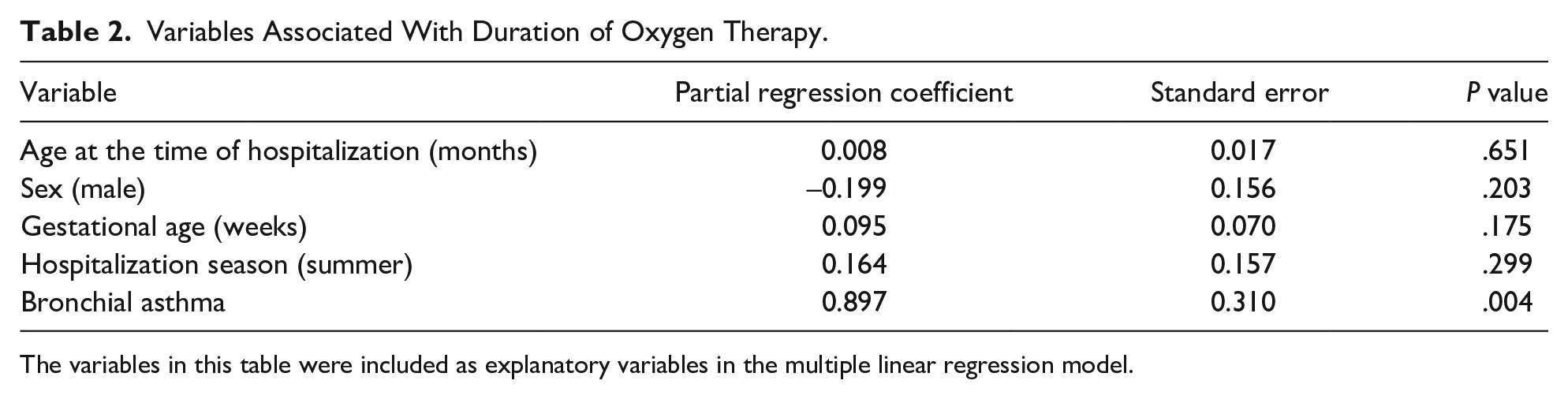
The variables in this table were included as explanatory variables in the multiple linear regression model.
Variables Related to Severe Conditions.

Abbreviations: CI, confidence interval; OR, odds ratio.
The variables in this table were included as explanatory variables in the logistic regression model.
Discussion
In this study, we specified, in a dualistic manner, the duration of oxygen therapy and condition severity as indices for the difficulty of treatment of RSV infection. The results suggested that bronchial asthma is a risk factor for prolongation of duration of oxygen therapy and morbidity in summer is a risk factor for progression to a severe condition.
Being a premature infant, a history of perinatal respiratory disorder, malnutrition, congenital heart disease, and chronic neurological disorder are known risk factors for progression of RSV infection to a severe condition. 13 The American Academy of Pediatrics proposed that bronchiolitis in general involves the risk for progression to a severe condition if it occurs within 12 weeks after birth. 14 For RSV in particular, young age in months has been reported to be a predictive factor for progression to a severe condition. 15 Moreover, RSV infection was reported to be a precipitating factor for bronchial asthma 16 and a risk factor for recurrent wheezing. 17 However, difficulty of the treatment of pediatric patients who have underlying bronchial asthma or who developed RSV infection in summer has been mentioned only in a few reports. 18
The present study showed that, among pediatric patients with RSV infection, the length of the period during which they required oxygen therapy significantly differed between those with bronchial asthma and those without. Considering this finding and the past report suggesting that RSV infection is a precipitating factor for bronchial asthma, we can conclude that the duration of oxygen therapy in cases of RSV infection is prolonged when there is underlying bronchial asthma. The present study also showed that a significantly greater number of patients with RSV infection in summer had severe disease. Among the 17 subjects who had severe disease in summer, only 2 had bronchial asthma. Therefore, we speculated that the progression to a severe condition in subjects who had RSV infection in summer does not reflect the worsening of bronchial asthma, but simply suggests the worsening of lower respiratory tract lesions. Although the subjects in this study included many infants younger than 12 months old, age in months at the time of hospitalization was not a factor influencing the progression to a severe condition. However, the patients who required ventilator management by tracheal intubation that were excluded from the study were 0 and 1 month old. In this study, age was not a risk factor, but we think that infection in newborns requires careful examination. Preterm birth is known to be a risk factor, 11 but it was not a risk factor in this study. This may be due to the small number of preterm infants and the fact that more than half of preterm infants are hospitalized after the age of 1 year. Regarding sex, overseas papers point out that being male is a risk factor, but there has been reports of no sex differences in Japan.11,19 In the subjects of this study, there was no significant difference in aggravation by sex, and there was no difference in the profiles of men and women.
Although excluded from participating in this study, 6 children were indicated for palivizumab during the study period. Of these, 3 were hospitalized before administration of palivizumab and 3 were hospitalized after administration. The 3 subjects treated with palivizumab were not severe. Of the 3 subjects not treated with palivizumab, 2 were severe. These subjects were admitted in September and were infected with RSV before the scheduled day of the administration of palivizumab. Progression to a severe condition might have been prevented by earlier administration of palivizumab in these subjects.
In Japan where the climate is temperate, epidemics of RSV used to be commonly believed to occur in winter, mainly in December. In recent years, however, the epidemic period has changed. In Okinawa, where the climate is subtropical and greatly differs from the climate in other prefectures, the epidemic period has been considered to be from February to September. 20 A similar tendency has recently been observed in the Kanto region. A report indicated that RSV was more active at temperatures of 24°C or higher and 6°C or lower, and most stable when the humidity was 40%. 21 Another report showed that RSV was more active when the relative humidity was 45% to 65%. 22 Still another report demonstrated that RSV preferred a narrow range of humidity and suggested that its detection rate is decreased by 3.8% when the humidity increases by 1%. 23 From 2014 to 2019, the mean temperature in June to September matched the range of temperature at which RSV is considered to become more active. In contrast, from 2014 to 2018, the relative humidity in April to September was 62% to 86%. 24 It means that relative humidity was higher than the humidity at which RSV is considered to be more active. This suggests that RSV becomes more active at higher relative humidity. It is necessary to continue to observe the epidemics and manifestations carefully, paying attention to climate conditions. In this study, the strain, genotype, and viral load of RSV could not be examined. In addition to the weather conditions, it is possible that the above factors may affect the severity. However, this study could not identify the reason why summer infections are a risk factor for aggravation.
Limitations
Because this study was a retrospective evaluation and the medical history of the patients was obtained from their medical record, patients with bronchial asthma might not have been completely categorized into the group with this disease. Duration of oxygen therapy, an indication of high flow systems, was not evaluated strictly based on uniform indices such as numbers and scores and therefore might have been influenced by subjective views of primary physician and physicians in charge. The possibility that these evaluation methods affected the risk factors for prolongation of duration of oxygen therapy and progression to a severe condition cannot be denied. Moreover, genetic search for viruses was not performed and it was not determined whether or not any mixed infection with other viruses occurred because of retrospective method of this study. In the future, it is desirable to collect samples and perform these analyses for patients with severe conditions.
Conclusion
Bronchial asthma was a risk factor for prolongation of duration of oxygen therapy and infection in summer was a risk factor for progression to a severe condition in RSV infection. This study indicated that infection in summer needs to be treated carefully.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X221100950 – Supplemental material for Summer Hospitalization and Bronchial Asthma Make Treatment of Respiratory Syncytial Virus Infection Difficult: A Retrospective Study in Japan
Supplemental material, sj-docx-1-gph-10.1177_2333794X221100950 for Summer Hospitalization and Bronchial Asthma Make Treatment of Respiratory Syncytial Virus Infection Difficult: A Retrospective Study in Japan by Kosuke Oikawa, Hirotaka Ochiai, Kazuhiko Matsuhashi, Motoichiro Sakurai, Manabu Suzuki, Masaya Koganesawa, Tomomasa Terada, Yoko Ishii, Akatsuki Kokaze and Katsumi Mizuno in Global Pediatric Health
Footnotes
Acknowledgements
We express our deep thanks to Dr. Yoshifusa Abe, Associate Professor in the Children’s Medical Center, Showa University Koto Toyosu Hospital, for his kind support and advice. We also thank all patients and parents who participated in the study.
Author contributions
K.O., M.S., and M.K. planned the study; K.M., M.S., M.K., T.T., and Y.I. contributed to acquisition, analysis, or interpretation of data; H.O. and A.K. checked the study design and examined the statistical validity; K.O., H.O., A.K., and K.M. were in charge of manuscript writing. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.