
Abstract
Cerebral aspergillosis is a fungal infection with a bad prognosis. It usually occurs in immunocompromised patients and manifests itself .Cross-sectional imaging reveals suggestive lesions.
Introduction
Aspergillosis is a fungal infection caused by filamentous fungi of the genus aspergillus. With pulmonary tropism, it usually occurs in immunocompromised patients and is accompanied by significant morbidity and mortality.
Observation
A 12-year-old boy, initially diagnosed with a respiratory tract disease was received in our department for investigations on a prolonged fever resistant to antibiotics after 15 days of treatment. His history included chemotherapy for LAT/RE and stage 4 mucositis. A thoracic CT scan showed, in addition to a pneumonia lesion, pulmonary nodules suggesting invasive pulmonary aspergillosis (Figure 1). A laboratory study of the bronchioloalveolar lavage fluid, coupled with culture, confirmed the diagnosis; the patient was put on anti-fungal treatment.
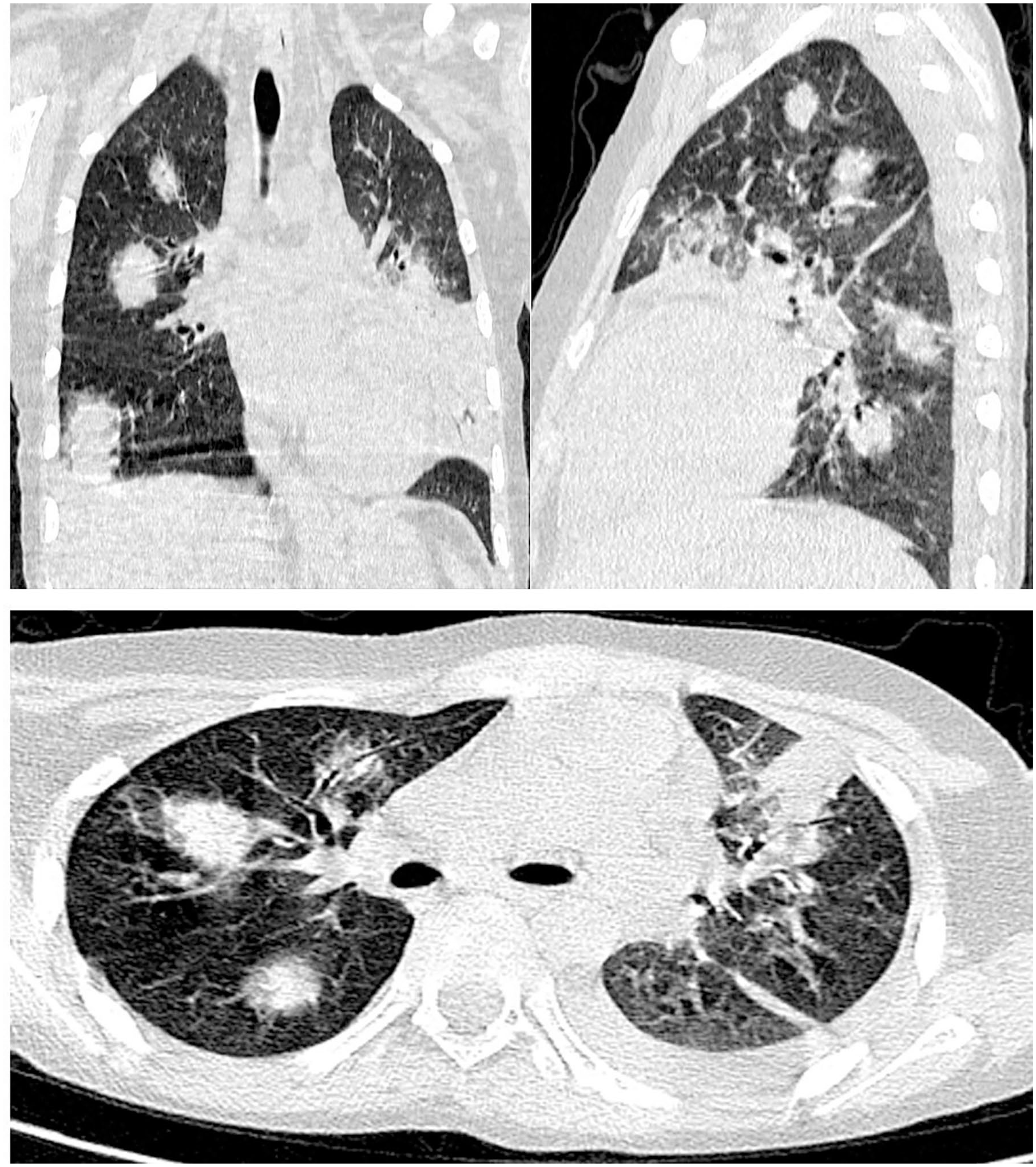
(a, b, c) CT sections in 3 planes, in parenchymal window, showing multiple solid nodules of random distribution, surrounded by halots of ground glass.
Two weeks later, the patient became unconscious with a Glasgow Coma Scale of 3 (GCS = 3), following an aphasia and a right hemiplegia. The blood workup found a correct blood sugar level, there was also a severe neutropenia (500 e/mm3), as well as hyponatremia at 127 mEq/L. A cerebral MRI was performed (Figure 2).His evolution was favorable at 1 month on treatment, marked by the improvement of the Glasgow score from 3 to 9 and the normalization of neutrophil counts.

Bilateral asymmetric subcortical signal abnormalities predominantly fronto-parieto-occipital on the left corona radiata and U-shaped fibers in T2/FLAIR hypersignal (a and b), T1 hyposignal (c), variable in DWI (d) showing heterogeneous gyriform and annular enhancement in some areas (e), related to microabscesses. Microbleeds are also seen (f), reflecting hemorrhagic necrosis.
Discussion
Cerebral aspergillosis usually occurs in immunocompromised patients (neutropenic, with malignant blood diseases, or transplanted).
In rare cases, a disseminated form can be observed, affecting in addition to the respiratory system, the central nervous system, whose involvement is accompanied by a significant morbi-mortality. 1
The neurological manifestations are not specific and can range from a simple vigilance disorder with focal signs to a coma.
Cerebral aspergillosis is suspected when a certain number of elements are present, namely: a terrain at risk of invasive aspergillosis (profound or prolonged neutropenia, hematological malignancy, prolonged high-dose corticosteroid therapy, marrow or solid organ transplantation, AIDS), persistent fever despite antibiotic therapy, respiratory signs such as hemoptysis (an association being observed for 80%-95% of cases). 2
Two forms of manifestation depending on the immune status are to be distinguished in imaging, it can be an abscess with peripheral contrast surrounded by a perilesional oedema in patients with little or no immunosuppression, secondary to sinus aspergillosis or lesions of the white matter, basal ganglia or thalamus which are enhanced after injection and occur by hematogenous dissemination in patients with profound immunosuppression, as in the case of our patient. 3
Cerebral MRI allows a better characterization of these lesions, it finds multiple cortico-subcortical lesions in T2 hypersignal, in T1 hyposignal, with or without annular enhancement after injection of gadolinium. In MRI diffusion weighted imaging (DWI), these lesions present 3 areas with different signals: central and peripheral hyposignal corresponding respectively to necrosis and vasogenic oedema and a hypersignal of the intermediate area with low ADC related to an infarcted area. In some cases, leptomeningeal enhancement may be present, including gradient echo without signals suggestive of microbleeds, thrombosis, or mycotic aneurysms. 4 On the CT scan, these abscess lesions will be seen as hypodensity with annular enhancement and perilesional hypodensity. In the presence of this type of lesion in immunocompromised patients, other causes of annular enhancement should be eliminated, such as toxoplasmosis, cryptococcosis, candidiasis or a malignant lesion (lymphoma). 5
In conclusion, cerebral aspergillosis occurs in immunocompromised patients in general, it manifests in the form of an annular enhanced lesions with 3 zones of different signals on MRI.
It manifests in a form of an abscess and micro-bleedings. However, the diagnosis of this infection passes by the confrontation of a bundle of clinical, biological and imaging arguments.
Footnotes
Author Contributions
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.