
Abstract

Introduction
The double aortic arch is a rare congenital cardiovascular anomaly, usually diagnosed within toddlers in the first 6 months of life, due to an external obstruction of the trachea and/or esophagus by a vascular ring formed due to persistence of 2 aortic arches.
Imaging is the examination of choice to confirm the diagnosis.
We report the case of a 2 years old infant admitted for acute stridor to which a bronchoscopy performed showed an external obstruction of the trachea suggesting a double aortic arch, confirmed by a chest CT angiography as a complete balanced double aortic arch.
Case Report
A 2 years old toddler with no medical history records was admitted for acute stridor, to which a chest radiograph performed was normal, and a bronchoscopy was required to look for tracheal obstruction, except it showed no airways anomaly but an external obstruction of the trachea. A chest CT angiography performed, revealed the presence of a balanced double aortic arch forming a vascular ring encircling the trachea causing its compression with a reduced lumen (4 mm). The left arch and right arch have almost equal diameters (right arch = 18.9 mm, and left arch = 19.5 mm) and from each arch arises a common carotid artery and subclavian artery, forming a “four vessel” sign (Figure 1).
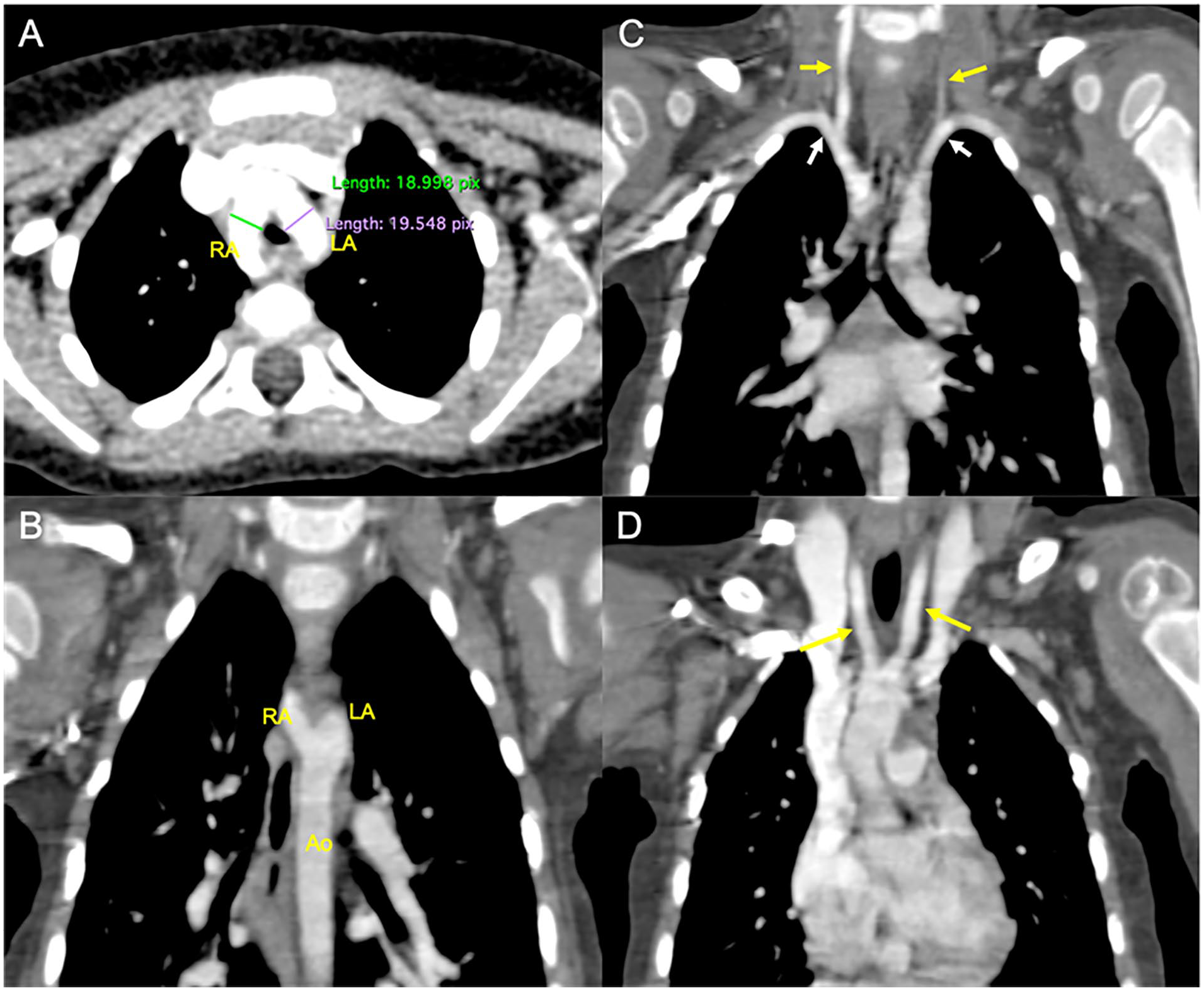
Chest CT angiography of a 2 years old toddler, in axial (A) and coronal (B–D) reconstructions, showing a balanced double aortic arch with a right arch (RA) and left arch (LA) having an equal diameter forming a vascular ring around the trachea (A) joining together to the descending aorta (B). From each arch arises a common carotid artery (yellow arrow) and a subclavian artery (yellow arrow) forming a “four vessels” sign (C and D).
No other anomaly was noted and the diagnosis of a balanced double aortic was retained.
Discussion
The double aortic arch (DAA) is an uncommon congenital anomaly caused by the persistence of a right aortic arch forming with the left aortic arch a complete vascular ring around the trachea and esophagus causing its compression. 1
It was first described by Wolman in 1939, 2 and represents 46% to 76% of complete vascular rings, and 0.8% to 2% of all congenital cardiovascular malformations.1,3
In organogenesis, 6 pairs of aortic arches develop at different stages: the first 2 arches regress forming the maxillary, hyoid, and stapedial arteries. The third pair forms the common carotid artery and part of the internal carotid artery.
The fourth pair of arches forms the right and left aortic arches, normally by the fifth gestation week, the right arch regresses whereas the left will persist forming the aorta.
In case of failure of involution of the right arch, and persistence of the left arch a double aortic arch is formed creating a vascular ring around the trachea and esophagus, and joining together to the descending aorta.1,2,4
Usually in vascular rings, 1 arch is patent while the other is either focally of diffusely narrowed or atretic, and depending of the patency of the arches, 3 types are described:3,4
Right sided dominant DAA: (55%-70%) the right arch is large and posterior and the left one is thinner and anterior.
Left sided dominant DAA: (20%-35%) the left arch is large whereas the right arch is small or atretic.
Balanced DAA: represents 2 arches with an equal diameter and they are extremely rare with only a 5% to 10% incidence of all DAA.
The most common form is the presence of a large right aortic arch, a left sided descending aorta and a left sided ligamentum arteriosum.
The descending aorta stands usually at the opposite of the dominant arch.
From each arch arises a common carotid and subclavian artery leading to a symmetric appearance of the supra-aortic trunks seen in a transverse section imaging as a “Four vessel, four artery” sign. 5
Clinical symptoms of DAA are usually seen within the first 6 months of life, and are mostly represented by respiratory symptoms such as stridor due to an external obstruction of the trachea. 3
Other symptoms include: recurrent respiratory infections, wheezing, and coughing, sometimes symptoms may be falsely taken for asthma.
Bronchoscopy may lead to diagnosis, showing an external compression of the trachea.
Imaging is the examination of choice to confirm diagnosis. Its modalities include: 5
Trans-Thoracic echocardiography, Cardiac MRI (Magnetic Resonance Imaging), and CT (Computed Tomography) angiography.
Trans-thoracic echocardiography is considered as the first line examination in pediatric patients, to lead diagnosis and analysis of other cardiac anomalies.
CT-scan is the examination of choice for diagnosis, it allows a rapid high special resolution imaging of the vascular anomaly with a precise evaluation of the anatomy of the double aortic arch precising its dimensions, position of each arch, the patency of each arch, the relationship of the vascular ring with the trachea and esophagus, their degree of compression, and evaluation of associated anatomical variants of the supra-aortic trunk. 4 However, radiation exposure of the infants is a disadvantage of computed tomography.
Cardiac MRI is an alternative examination allowing a detailed study with less radiation exposure; however, it requires sedation due to the longer acquisition time.
Treatment of DAA is surgical; it is especially indicated for symptomatic patients to relieve compression of the trachea or esophagus, but can also be included for a patient’s surgery to associated cardio-vascular anomalies. Surgical procedure requires division of the lesser arch. Post-operative prognosis is usually good.6,7
Conclusion
In cases of infants presenting recurrent pulmonary infections, wheezing, or stridor, a respiratory cause is usually suspected, however, an external cause of compression of the respiratory tract such as a DAA, shouldn’t be neglected even if uncommon.
Imaging resides as the examination of choice to confirm diagnosis, especially through a chest CT angiography or cardiac MRI.
Footnotes
Author Contributions
LB: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. MO: Contributed to conception and design; Contributed to analysis; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. YEH: Contributed to conception and design; Contributed to analysis; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA: critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. LC: Contributed to acquisition, analysis, or interpretation; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SEH: Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report.