
Abstract
Background. Undernutrition is a global problem and the biggest threat to human life and economic progress. It is the main cause of child morbidity and mortality especially in sub-Saharan Africa including Ethiopia. The severity of the problem is even worse when children are infected with human immunodeficiency virus. However the seriousness of the problem, there were limited studies conducted in the study area. Therefore, this study was conducted to assess the magnitude of undernutrition and its associated factors among HIV-infected children on follow up in Amhara Region Referral Hospitals. Methods. A facility-based cross-sectional study was conducted from February to April 2020. The data were collected through an interviewer-administered questionnaire. The collected data were coded and entered into Epi data 3.1 and exported to SPSS 26.0 for analysis. P-value <.05 was considered as statically significant. Results. The magnitude of undernutrition in this study was 30.3%. Dietary diversity (AOR = 1.73; CI 1.07-2.81), nutritional counseling (AOR = 2.42; CI 1.45-4.04), family size (AOR = 0.50; CI 0.27-0.93), WHO staging (AOR = 1.77; CI 1.08-2.88), and adherence to antiretroviral therapy (AOR = 1.75; CI 1.06-2.87) were predictors of undernutrition. Conclusions. Nearly one-third of the children included in this study had undernutrition. Poor dietary diversity, adherence to ART, nutritional counseling, family size, and WHO staging were factors significantly associated with undernutrition. Early screening and treatment of opportunistic infections, close attention to dietary counseling for caregivers and proper feeding habits will alleviate the problem.
Introduction
Undernutrition is remaining a global problem and the biggest threat to human life and economic progress 1 ; affecting majority of the world’s population at some point in their lifecycle. 2 It’s an imbalance nutritional which could be due to inadequate nutrients intake as required by the body. Undernutrition is defined by 4 conditions which are low weight for height (wasting), low height for age (stunting), low weight for age (underweight), and low body mass index (BMI) for age (thinness). 3 It is the main risk factor for various medical problems such as poor cognitive developments, premature death, and other health consequences. 4 Mortality and morbidity due to undernutrition is high especially in sub-Saharan Africa including Ethiopia.5,6
Undernutrition and Human Immunodeficiency Virus (HIV) are the main contributors to global health. HIV-infected children are more prone to undernutrition compared to HIV un-infected due to inadequate dietary intake, nutritional losses, metabolic changes, and increased requirements for both macro and micronutrients. 7 Both disease are interact each other with a vicious cycle that increases vulnerability and worsens the severity of each condition.8 -11 Based on the national HIV care and World Health Organization (WHO) recommendations, the energy requirement of HIV infected children increased by 10% in asymptomatic child as compared to a non-infected child, 20% to 30% in case of symptomatic HIV infection, and 50% to 100% in cases of severe malnutrition.12,13
Globally, there are different strategies, programs, and policies which provide aspiring and far-reaching goals on prevention, treatment, and health coverage, such as sustainable development goals (SDG) agenda, it was released in 2015 to be achieved by 2030. 14 From this agenda, ending hunger and no malnutrition was the main target among 17 other strategies. 14 Improving children’s nutritional status requires effective and sustained multi-sectorial nutrition programming over the long term. 15 However these strategies are implemented, the problem is still not alleviated.
Studies in developing countries have shown that most children infected with HIV have extreme immune suppression and poor nutritional status. Human immune virus (HIV) affects nutritional status of an individual by altering immune functions and due to HIV-related co-infections.11,16,17 Besides malnutrition, Ethiopia is considered to be one of the countries affected by HIV epidemic; malnutrition affects several individuals either before or after the initiation of ART. Several studies were done in adult HIV-infected individuals regarding their nutritional status.18 -20 There were also a few studies conducted to describe the magnitude of undernutrition and associated factors among HIV infected children in Ethiopia.21,22 These studies did not incorporate factors like adherence to ART, feeding frequency and CD4 count, but these factors are significant in other study.23,24 Therefore, this study tried to show the magnitude of undernutrition and its associated factor among children infected with HIV at regional level.
Methods and Materials
Study Period and Setting
This study was conducted among HIV infected children in Amhara regional state which is located in the North-Western part of Ethiopia. Bahir Dar is a capital city of Amhara regional state located 563 km Northwest from Addis Ababa, the capital city of Ethiopia. According to the regional health bureau report in 2019, the region has 81 government hospitals, 850 Health Centers, and 3500 Health Posts. Among the 81 hospitals, Dessie, Felege-Hiwot, Tibebe Ghion, University of Gondar, Debre Birhan, and Debre Markos hospitals are Tertiary care (Referral) hospitals. The study was conducted from February 25 to April 25, 2020.
Study Design and Population Characteristics
A facility-based cross-sectional study was conducted among HIV infected children in Amhara region referral hospitals. All HIV infected children whose ages from 5 to 14 years old on follow up at ART clinic in Amhara region referral hospitals were considered as the source population and HIV infected children whose ages from 5 to 14 years old on follow up at ART clinic in the selected referral hospitals during the study period were study population. Children who visited the health facilities for the first time, and those who did not have medical records with complete information and children having physical deformity (like spinal deformity) were excluded.
Sample Size Determination and Procedure
The sample size was determined by using a single population proportion formula, assuming a 95% level of confidence, and 5% margin of error. The Estimated proportion (P) = 60.2% which is the overall malnutrition. 21 By adding 10% non-response rate, the final sample size was 405.There are 6 public Referral Hospitals in Amhara region and only 5 are giving ART services. These are Dessie, Debre Markos, Debre Birhan Referral Hospitals, and 2 comprehensive specialized hospital (Felege-Hiwot and University of Gondar). From the 5 Referral Hospitals 3 Hospitals namely Dessie, Felege-Hiwot, and Debre Markos were selected by using simple random sampling method. Then the total sample size for the study was proportionally allocated to each selected hospitals. Study participants were selected using systematic random sampling techniques and K-value was calculated for each selected hospital. The K-value of each referral hospital was given as; Dessie Referral Hospital K1 = N/n = 271/168 = 1.61 to 2, Debre Markos Referral Hospital K2 = N/n = 141/87 = 1.62 to 2, Felege-Hiwot Comprehensive Specialized Hospital K3 = N/n = 243/150 = 1.62 to 2. The numerators 271, 243, and 141 were the number of HIV positive children currently on follow up at Dessie, Felege-Hiwot, and Debre Markos Referral Hospital respectively.
Operational Definitions
To determine Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS) progression, we used the WHO clinical staging system, a 4-stage classification system. We classified the first 2 stages as “early stages” (stage 1 and 2) and clinical HIV stages 3 and 4 as “advanced stages.” We retrieved the data on WHO clinical stage from the medical files of each patient. The health workers update the clinical stage on a routine basis with each patient visit to the facility.5,12,29
Data Collection Tools and Procedure
Data were collected by interviewer-administered structured questionnaire. The questionnaire was developed by reviewing different related literatures and it consisted of 4 parts: socio-demographic characteristics, anthropometric measurements, nutritional related factors, and clinical related factors. The questionnaire was prepared in English and translated to Amharic and then translated back to English to check its consistency. Child weight and height was measured during their visit. Weight measurement was taken by standardized weight measurement which is appropriate for the age of the child by calibrating after each measurement with a precision of 0.05 kg. On the other hand height measurement was done based on the age of the child. Standing height was measured with a precision of 0.01 m for those who are able to stand. Whereas children who cannot stand up or are too weak to do so was measured in recumbent position. The clinical related factors were taken from the child ART follow up chart.
To determine the minimum individual dietary diversity score (DDS) of the child, the mother/caregiver was asked about the food items consumed by the child in the previous 24 hours before data collection. Then, the food items consumed by the child were grouped into 8 food groups according to Food and Nutrition Technical Assistance (FANTA) individual dietary diversity assessment tool. 30 Namely: cereals, roots, and tubers; legumes and nuts; dairy products (milk, yogurt, cheese); vitamin A rich fruits and vegetables; flesh foods (meat, fish, poultry, and liver/organ meats); eggs; fat and oil; and other fruits and vegetables. 31
Data Collection Method and Quality Control
The data collectors were 6 BSc Nurses from all health facilities, who trained on comprehensive HIV care and currently involved in follow up care. Prior to the actual data collection time the questionnaire was pre-tested on 5% of the sample size at Debre Tabor hospital to check for its clarity, consistency, acceptability, and applicability of the tool. One day training was given for 3 supervisors and 6 data collectors to create a common understanding on the procedure and approaches to be used during data collection. Data were checked for its completeness throughout the data collection time by supervisors and data collectors and the completeness of the data were checked during entry.
Data Processing and Analysis
The data were checked; coded and entered into Epi data version 3.1 and exported to SPSS version 26 for analysis. The anthropometric data were entered in to Antroplus software version 1.04 to calculate anthropometric indices. Descriptive statistics; including frequencies, percentages, and summary statistics (mean, median) and figures were used to describe the independent variables in relation to the outcome variable. Bivariable logistic regression analysis was carried out to check the association of independent variables with the outcome variable and to select candidate variables for multivariable logistic regression analysis. Then, those variables with P-value ≤.25 from the bivariable analysis were entered into multivariable logistic regression analysis using a backward likely hood ratio method to examine the association between the dependent and independent variables. Model fitness was checked by using Hosmer-Lemeshow goodness of fit test. Finally, the strength of association between the dependent and independent variables were showed using Adjusted Odds Ratio (AOR) and its 95% confidence interval (CI). P-value <.05 was considered as statistically significant predictor of undernutrition.
Ethical Consideration
Ethical clearance was obtained from ethical review board of Bahir Dar University, College of Medicine and Health Sciences with a protocol number of 0028/2020. Then official letter was submitted to Dessie, Felge-Hiwot, and Debre Markos referral hospitals administrative bodies. A necessary explanation was given for the respondents about the purpose and the procedure of the study and their right to participate or not to participate in the study. Confidentiality of the response was declared to the respondents by the anonymity of the interviewer-administered questionnaire. Participant’s oral informed consent was taken before recruitment to participate in the study. Name and other personal information that can violate the confidentiality of the respondents were not taken. During data collection, the privacy of respondent was kept and the duration of the interview was also explained.
Results
Socio-Demographic Characteristics
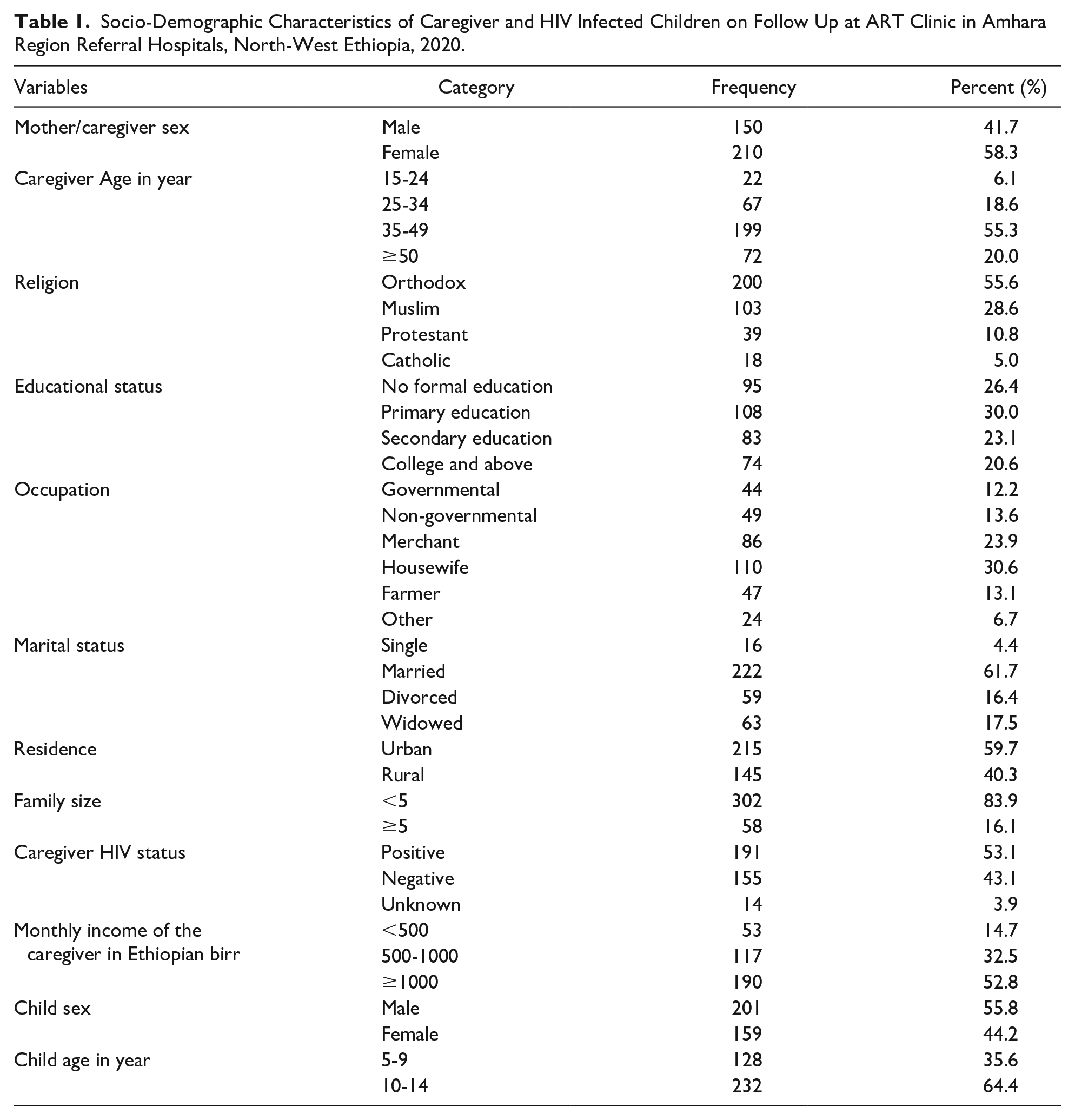
A total of 360 children age from 5 to 14 years old were included in this study with the response rate of 88.90% were participated in this study. More than half of the caregivers 210 (58.3%) were females and mean age of caregivers was 40.97 ± 10 (SD) years. About 200 (55.6%) of respondents were Orthodox Christian in religion and nearly one-third (30.6%) of the caregivers were house wife in their occupation. More than half of the respondents (59.7%) live in an urban setting. Regarding to the sex and age of children, 201 (55.8%) were males and the median age was 11 years with IQR 5 years (Table 1).
Socio-Demographic Characteristics of Caregiver and HIV Infected Children on Follow Up at ART Clinic in Amhara Region Referral Hospitals, North-West Ethiopia, 2020.
Nutritional and Dietary Related Factors of HIV Infected Children on Follow at ART Clinic
About 278 (77.2%) of the children were fed <4 meals per day and more than half (58.9%) of the children’s caregiver didn’t received nutritional counseling (Table 2).
Nutritional Related Factors among HIV Infected Children on Follow Up in Amhara Region Referral Hospitals, North-West Ethiopia, 2020.

Dietary Diversity by Food Group Among HIV Infected Children on Follow at ART Clinic
There were 8 food groups consumed by the child in past 24 hours, from this cereal food group, vitamin A rich fruit, and vegetable and fat/oil were the food groups predominantly consumed by the participants during the 24-hour recall, 85.6%, 74.7% and 78.6% respectively, whereas the least consumed food groups by the children were flesh food (27.8%) and dairy products (28.6%) (Figure 1).

Food groups consumed by the child in the last 24 hours. before the survey among children infected with HIV who are on follow up at ART clinic in Amhara Region Referral Hospitals North-west Ethiopia, 2020.
Magnitude of Undernutrition Among HIV Infected Children on Follow Up at ART Clinic
The prevalence of overall undernutrition among children living with HIV who were attending ART clinic in Amhara region referral hospitals was 30.3% (95% CI 25.3-35.2). This study also shows the prevalence of undernutrition in females was greater than males 32.1% and 28.9% respectively. The magnitude of stunting and thinness in this study was 19.4%, 19.2% respectively.
Clinical and Related Characteristics of HIV Infected Children on Follow Up at ART Clinic
Regarding to the health-related characteristics, 245 (68.1%) of the children were on first-line ART regimen and 221 (61.4%) children were currently on WHO clinical stage I and II. About 251 (69.7%) had opportunistic infection in the past 6 months of these 65 (25.9%) of children had pneumonia in the past 6 months. More than one-third (37.2%) of children developed eating difficulties in the past 6 months, among them 42 (31.3%) of children complained swallowing problem. About 257 (71.4%) of children have been on follow-up for >5 years (60 months) (Table 3).
Clinical and Related Characteristics of HIV Infected Children Who are on Follow Up at ART clinic in Amhara Region Referral Hospitals, North-West Ethiopia, 2020.
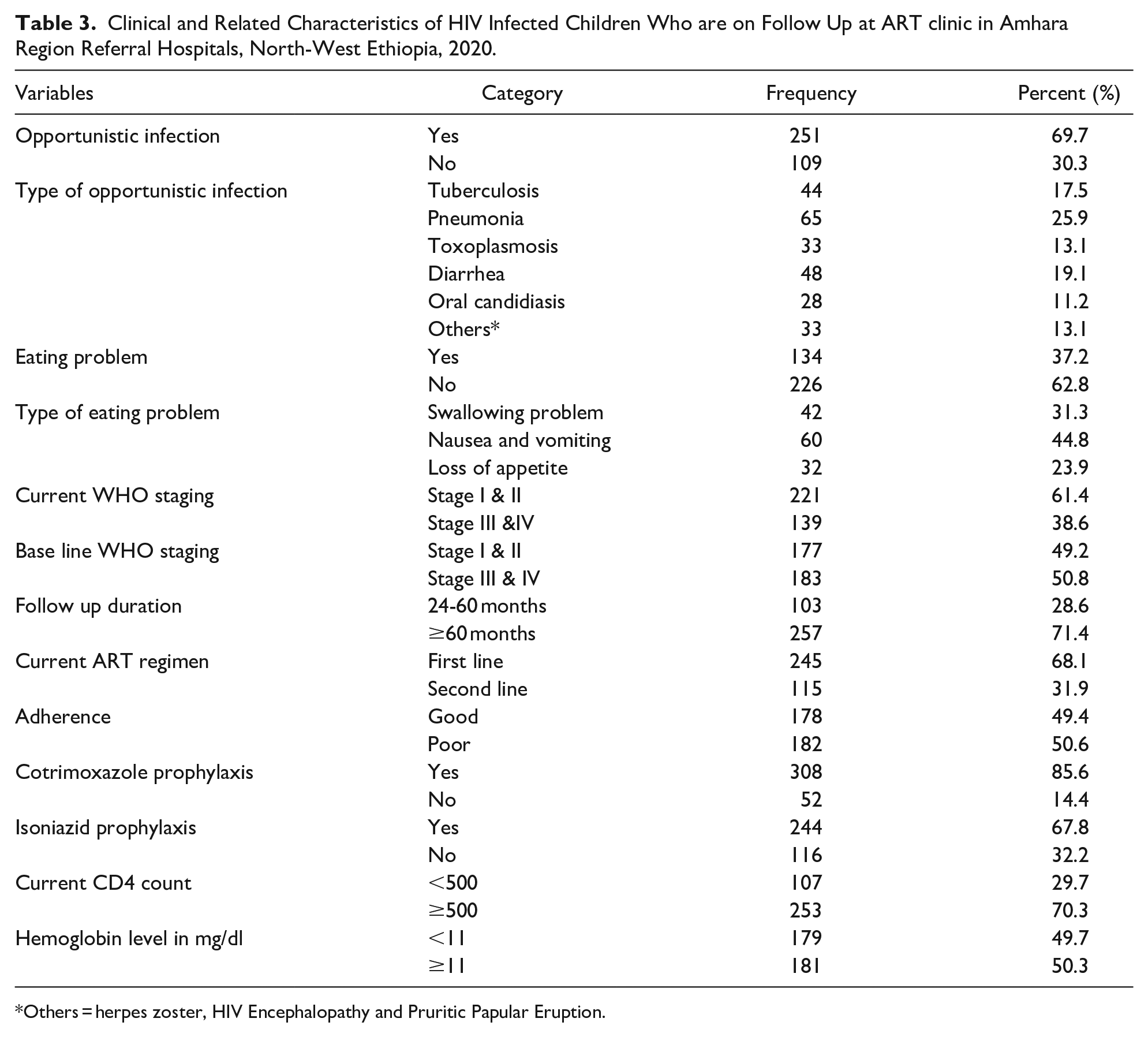
Others = herpes zoster, HIV Encephalopathy and Pruritic Papular Eruption.
Factors Associated With Undernutrition Among HIV Infected Children on Follow Up at ART Clinic
In bivariable logistic regression analysis factors with P-value of ≤.25 were educational status of caregiver, family size, monthly income of the caregiver, nutritional counseling, dietary diversity, current WHO staging, adherence to ART, hemoglobin level, current CD4 count, opportunistic infection, follow up duration, and age of the child.
To control for possible confounders all independent variables with P-value ≤.25 on bivariable analysis were included in multivariable analysis and P-value <.05 in multivariable logistic regression were considered as significant. The multivariable analysis indicated that family size, dietary diversity, nutritional counseling, current WHO staging and adherence to ART were significantly associated with undernutrition.
Children who had poor individual dietary diversity were 1.7 times more likely to be undernourished than those children who had good dietary diversity (AOR = 1.73; CI 1.07-2.81). Children living in households with a family size <5 members were 50% less likely to be undernourished than those children living in households with a family size ≥5 family members (AOR = 0.50; CI 0.27-0.93). Children currently with clinical-stage III and IV were about 1.8 times more likely to develop undernutrition compared to those clinical stages I and II (AOR = 1.77; CI 1.08-2.88). Children whose caregivers didn’t get nutritional counseling were 2 times more likely to be undernourished as compared to those who were getting nutritional counseling by a health professional at ART clinic(AOR = 2.42; CI 1.45-4.04). Those children who had poor adherence to HAART in the past 6 months had 1.7 times more likely to develop undernutrition than those children who have good adherence (AOR = 1.75; CI 1.06-2.87) (Table 4).
Factors Associated with Undernutrition Among HIV Infected Children on Follow at ART Clinic in Amhara Region Referral Hospitals, North-West Ethiopia, 2020.

P-value ≤.05.
Discussion
In this study, the magnitude of undernutrition in HIV infected children who were on follow up at ART clinic was 30.3% (95% CI 25.3-35.2). Magnitude of undernutrition in this study was lower than a study done in Thailand (43%), west and central Africa (42.3%), east and west Gojjam (Ethiopia) (60.2%).10,21,27 The difference is due to differences in socio-economic and demographic-related characteristics of the study participants, sample size difference. 10 Moreover, a possible reason for the lower magnitude of undernutrition in this study could be attributable to the adoption of the recent WHO 90-90-90 test and treat policy, which has seen many more HIV infected children initiated on HAART early there by it brings change undernutrition comorbidity.32,33
The magnitude of stunting in this study was 19.4% which is in line with study conducted in Malaysia (20.8%). 9 But, the result the current study is lower than a studies conducted in India (58%), Tanzania (61.9%), El Salvador (33.2%), Addis Ababa (35.3%), and Hawassa (60.2%)22,25,26,29,34 respectively. The difference is due to differences in socio-economic and socio-demographic characteristics of the participants, sample size difference; relatively large sample size was used by study conducted in Tanzania and Addis Ababa Ethiopia and study period. The magnitude of thinness in this study was 19.2% which is in line with study conducted in Tanzania (21.1%) and India (19.5%).28,29
According to this study, children whose caregivers did not receive nutritional counseling were more likely to be undernourished than those who got nutritional counseling during their visit. This finding is in line with a study conducted in Hawassa referral hospital. 22 It is fact that receiving nutritional counseling plays a role in the management of undernutrition and child feeding practice. 13
WHO clinical stage III and IV has a significant effect on the likelihood of undernutrition, the odds of undernutrition was higher among children who were in WHO clinical staging III and IV as compared to children who were in WHO clinical staging I and II. This finding was supported by studies conducted in Hawassa, Ethiopia, Thailand, and Tanzania that WHO clinical staging III and IV was a significant association with undernutrition.22,27,35 This is due to children with advanced disease stages are more susceptible to develop co-morbid opportunistic infections. As the HIV infection progresses and the child suffers other infections the amount of additional energy need increases. The amount of additional energy needed increases as the HIV infection progresses and the child suffers other opportunistic infections. Thus, Additional care for opportunistic infections and routine first-line ART may also aggravate the side effects of patients’ like loss of appetite and poor nutritional status and compromise their resistance to the disease.13,36,37 Similarly, the odds of having undernutrition were higher among children who have poor dietary diversity, compared to those who have good dietary diversity. This also supported by other studies.21,22 This is fact that adequate nutrition, which is best achieved through consumption of a balanced healthy diet, is vital for health and survival for all individuals regardless of HIV status. Such feeding less diversified food group practices is due to low income, food insecurity, and poverty. 38
Similar to other studies39,40 in the current study the odds of undernutrition was higher among children from larger families compared to children from a family size <5 members. Large number of household members could contribute to low levels of child care and dietary intake. It is a basic truth that as the number of family members increased, they face the economical insufficiency to meet their family needs. The presence of more children in the family increases the demand for food, compromising availability. The overall good adherence to ART of this study was nearly half (49.4%). Children who had poor adherence were more likely to be undernourished than those children having good adherence. Highly active antiretroviral therapy (HAART) has been shown to be effective in extending survival and enhancing the quality of life of people living with HIV. At least 95% adherence to HAART is needed for HIV treatment to be effective. 12 ART acceptability, adherence, and effectiveness could be enhanced by improved attention to diet and nutrition. 41
Limitation of this study since the study used interviewer administered questionnaire, there might be social desirability and recall bias from respondents. Moreover, only anthropometric measurements were used to assess undernutrition, which assesses mainly the public health burden of undernutrition. The study did not include laboratory methods to assess nutritional status like micronutrient deficiencies.
Conclusions and Recommendation
Nearly one-third of the children included in this study had undernutrition. Poor dietary diversity, nutritional counseling, adherence to ART, family size, and WHO staging were factors significantly associated with undernutrition among children infected with HIV who are attended ART clinic in Amhara region referral hospitals during this study period. Early screening and treating of opportunistic infections, close attention to dietary counseling for caregivers and proper feeding habits will alleviate the problem.
Footnotes
Acknowledgements
The authors thank to staff of Felege Hiwot Comprehensive Specialized Hospital, Dessie referral Hospital, and Debre Markos referral hospital.
Authors’ Contributions
ND, SB, and MB had made substantial contribution to conception, design, and acquisition of data. ND drafted the manuscript. Finally, all authors revised the drafted manuscript carefully for important intellectual contents. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from Bahir Dar University College of Medicine and Health Science, School of Health Science Ethical Review Board with a protocol number of 0028/2020. Then, Officials at different levels in the hospital were communicated through formal letters. Confidentiality of the information was assured throughout the study process.
Data Availability Statement
The data used in this manuscript is available upon reasonable request by contacting the corresponding authors via email.