
Abstract
Obstructive sleep apnea (OSA) in children is leading to several consequences as reported in adults. A continuous positive airway pressure (CPAP) machine is one of the effective treatments in pediatric OSA. However, the CPAP adherence rate is approximately 50%. This study aimed to evaluate if any interventions that improve CPAP adherence in pediatric patients with OSA using a systematic review. We included intervention studies on CPAP adherence in pediatric patients with OSA regardless of machine types. Five databases were used for article searching. Search terms included OSA, adherence, compliance, and CPAP. The outcomes of this study were adherence rate and usage hours/minutes. The outcomes were compared between the intervention and comparator groups with descriptive statistics. There were 2931 articles from 5-database searching. There were 41 articles related with children. There were 7 articles conducted with any intervention on CPAP compliance. Of those, 4 studies included in the analysis. There were 3 significant differences between both groups in 2 studies. Those with caregiver support had significantly longer CPAP use/night by 86.60 minutes (95% CI 10.90, 162.30) and percentage of CPAP usage more than 4 hours/night by 18.10% (95% CI 3.87, 32.33) than those without caregiver support. Those who received BPAP therapy had higher chance of good PAP adherence than those who received CPAP by 18.17 times (95% CI 5.19, 63.70). Caregiver support and BPAP therapy significantly improved CPAP adherence in children with OSA. Further studies are required to add additional comparisons and also other interventions.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a disease with collapse of upper airway repeatedly resulting in intermittent hypoxemia during sleep. 1 A diagnosis of OSA in children can be made by polysomnography with an apnea-hypopnea index of 2 times/hour. 2 In adults, OSA is reported to be associated with several cardiovascular diseases. 3 Similarly, OSA in children is associated with several conditions including attention deficit and hyperactivity disorders, poor attention, lower IQ, failure to thrive, hypertension, left ventricular hypertrophy, and poor quality of life. 4 Children with OSA had significantly lower IQ than control group (85.8 vs 101.1: P .002). 5
A continuous positive airway pressure (CPAP) machine is one of the effective treatments in pediatric OSA. 2 A previous study found that adolescent patients with OSA and being adherent to CPAP had significantly improved school performance and quality of life than those without CPAP (P .012 and .034). 6 Even though CPAP is effective in 90% of patients, it has a compliance of approximately 50%. In adults, meta-analysis studies showed that an additional intervention such as educational, behavioral, or telemonitoring intervention was shown to improve CPAP adherence by 0.54 to 0.70 hours/night.7,8 However, there is limited data on an effect of additional interventions to improve CPAP adherence in pediatric patients with OSA. This study aimed to evaluate if any interventions that improve CPAP adherence in pediatric patients with OSA using a systematic review.
Methods
This study was a systematic review to evaluate if any interventions on PAP therapy in pediatric patients with OSA were associated with good CPAP adherence. We included intervention studies on CPAP adherence in pediatric patients with OSA. The studies were either observational or randomized controlled trial studies with 2 groups: intervention and comparator group. We excluded studies with any of the following: non-English, conference paper, study protocol, case report, case series, commentary, or non CPAP treatment.
There were several available positive airway pressure machine (PAP) that can be used to treat OSA patients including standard CPAP, automatic CPAP or APAP, Bi-Flex CPAP, or bi-level PAP or BPAP. The standard CPAP has a fixed-level of CPAP pressure, while the APAP has variable CPAP pressure depending on severity of OSA. The Bi-Flex CPAP is a specific technology of the Philips Respironics which lower pressure during late inspiration and expiration. The Bi-Flex technology may improve comfort or adherence. 9 The BPAP, non-invasive ventilator, produces positive airway pressure during inspiration and expiration. This machine may be used to improve adherence of PAP machine. 10
We searched 5 databases in this review: Pubmed, Central database, Scopus, CINAHL Plus, and Web of Science. Search terms included OSA, adherence, compliance, and CPAP. The full list of search terms are shown in an Appendix 1-5. The final search was performed on February 15, 2021. After duplication removal, initial screening was carried out for non-relevant articles. Only pediatric articles were eligible. Those articles without intervention were excluded. Of these, any articles met the study criteria were included in the final analysis. Data extraction and the full-text reviewed were performed by 2 independent authors (BS, KS). A prima flow chart of article searching and included studies was shown in Figure 1.

Searching results on adherence or compliance of continuous positive airway pressure machine in patients with obstructive sleep apnea.
The outcomes of this study were adherence rate and usage hours/minutes. The definition of good adherence of CPAP in pediatric patients with OSA may be varied, while the usage data was average use of CPAP per night. The outcomes were compared between the intervention and comparator groups with descriptive statistics. For numerical variables, mean differences between both groups were calculated and reported with their 95% confidence interval (CI). Odds ratio with 95% CI was computed to compare differences of proportions between both groups for categorical variables. Heterogeneity was computed and reported as and I square (I2) when appropriate. A forest plot of each comparison was created.
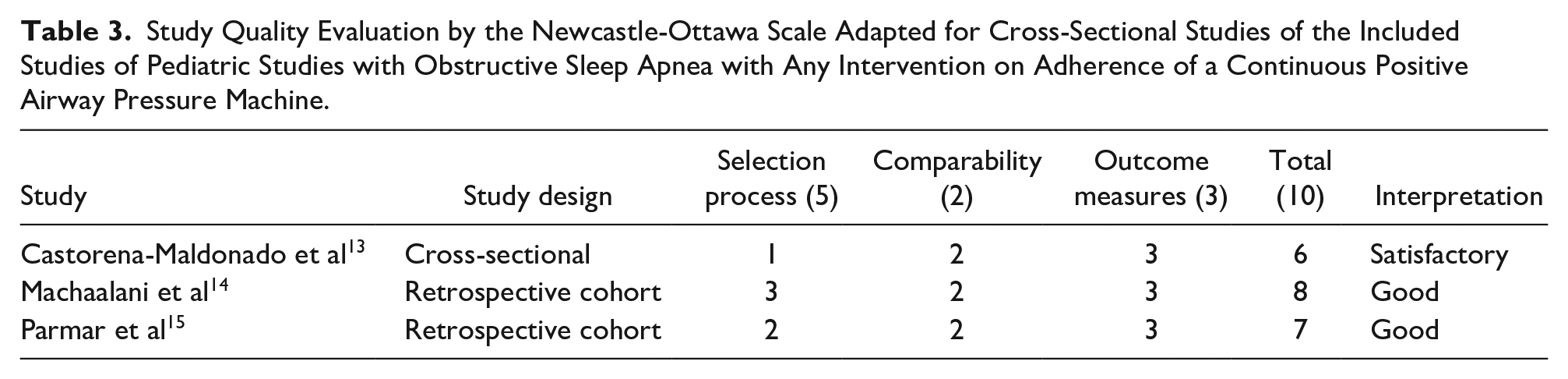
Biases of eligible studies were evaluated across 6 domains (sequence generation, allocation concealment, blinding of participants/personnel and outcome assessors, incomplete outcome data, selective outcome reporting, and other potential sources of bias) for randomized controlled trial. Biases were categorized as low risk, high risk, or unclear according to the guidelines specified in the Cochrane Handbook for Systematic Reviews of Interventions. 11 For observational studies, the Newcastle-Ottawa Scale adapted for cross-sectional studies was applied to evaluate study quality. 12 The scale comprised of 3 categories: selection process, comparability, and outcome measurement with a score of 5, 2, and 3 points, respectively. The total score was 10 points and classified as very good (9-10 points), good (7-8 points), satisfactory (5-6 points), and unsatisfied (0-4 points). Biases or study quality were evaluated by 2 authors independently (BS, CN). Disagreements were reviewed and reported by a third reviewer (KS). All analyses were performed by Review Manager 5.4.
Ethical Approval and Informed Consent
Not required.
Results
There were 2931 articles from 5-database searching. Of those, there were 1798 articles after removal of duplicated articles. There were 41 articles related with children. Of those, 34 articles were excluded due to not intervention (16 articles), review/book (10 articles), case series (2 articles), poster presentation (2 articles), non-English (2 articles), and commentary (1 article). There were 7 articles conducted with any intervention on CPAP compliance. Of those, 3 articles were excluded due to no comparison group (2 articles) and study protocol (1 article). There 4 articles published from 2008 to 2020 and conducted in 4 countries: Mexico, USA, Australia, and Canada (Table 1).9,13-15 One study was a randomized controlled trial, 9 while others were retrospective (2 articles) and cross-sectional study (1 article). Adherence data were objectively evaluated by download data from the PAP machine in all 4 articles with the longest follow up of 1 year. 14 The comparator was CPAP machine, while the intervention groups were caregiver support, BPAP, APAP, or Bi-Flex CPAP.
Characteristics of Pediatric Studies with Obstructive Sleep Apnea (OSA) with Any Intervention on Adherence of a Continuous Positive Airway Pressure Machine (CPAP).

Abbreviations: APAP: automatic CPAP; BPAP: bi-level positive airway pressure machine.
There were 247 pediatric patients enrolled in these 4 articles: 148 patients in the intervention group and 99 patients in the comparator group (Table 2). Regarding outcomes between the intervention and comparator groups (Table 2 and Figures 2–9), 3 studies reported on average PAP used/night and adherence rate.13-15 Among the outcomes, there were 3 significant differences between both groups in 2 studies as shown in Figures 2 to 4.14,15 Those with caregiver support had significantly longer CPAP use/night by 86.60 minutes (95% CI 10.90, 162.30) and percentage of CPAP usage more than 4 hours/night by 18.10% (95% CI 3.87, 32.33) than those without caregiver support (Figures 2 and 3). Those who received BPAP therapy had higher chance of good PAP adherence than those who received CPAP by 18.17 times (95% CI 5.19, 63.70) as shown in Figure 4. For study quality of those observational studies, 2 studies were good studies and 1 study was satisfactory (Table 3). There were 2 questionable biases and low risk for biases in 4 items including blinding of participants/personnel/outcome assessment, incomplete outcome data, selective reporting, and others (Figure 10).
Details and Outcomes of Pediatric Studies with Obstructive Sleep Apnea (OSA) with Any Intervention on Adherence of a Continuous Positive Airway Pressure Machine (CPAP).

Indicated proportion.
Abbreviations: APAP: automatic CPAP; BPAP: bi-level positive airway pressure machine.

Usage of continuous positive airway pressure machine (minutes) in pediatric patients with obstructive sleep apnea compared between those received caregiver support and those did not receive caregiver support.

Percentage of usage of continuous positive airway pressure machine more than 4 hours/night in pediatric patients with obstructive sleep apnea compared between those received caregiver support and those did not receive caregiver support.

Proportions of adherence in positive airway pressure machine (PAP) in pediatric patients with obstructive sleep apnea compared between those received bi-level positive airway pressure machine (BPAP) and those received continuous PAP (CPAP).

Hour usage of positive airway pressure machine (PAP) in pediatric patients with obstructive sleep apnea compared between those received bi-level positive airway pressure machine (BPAP) and those received continuous PAP (CPAP).

Percentage of day usage of positive airway pressure machine (PAP) in pediatric patients with obstructive sleep apnea compared between those received bi-level positive airway pressure machine (BPAP) and those received continuous PAP (CPAP).

Proportions of adherence in continuous positive airway pressure machine (CPAP) in pediatric patients with obstructive sleep apnea compared between those received automatic CPAP (APAP) and those received CPAP.

Hour usage of continuous positive airway pressure machine (CPAP) in pediatric patients with obstructive sleep apnea compared between those received automatic CPAP (APAP) and those received CPAP.

Minutes usage of continuous positive airway pressure machine (CPAP) in pediatric patients with obstructive sleep apnea compared between those received Bi-Flex CPAP and those received CPAP.
Study Quality Evaluation by the Newcastle-Ottawa Scale Adapted for Cross-Sectional Studies of the Included Studies of Pediatric Studies with Obstructive Sleep Apnea with Any Intervention on Adherence of a Continuous Positive Airway Pressure Machine.

Biases of a randomized controlled trial of pediatric studies with obstructive sleep apnea with any intervention on adherence of a continuous positive airway pressure machine.
Discussion
This systematic review showed that caregiver support and BPAP significantly improved CPAP adherence in pediatric patients with OSA.
Adherence of medical devices or CPAP may be complex. 16 There are several factors associated with medical devices such as perception, or experiences on the device. 17 A qualitative study conducted in patients with chronic obstructive airway disease who required to be treated with non-invasive ventilation. Similarly to CPAP, discomfort may be associated with chances of non-adherence.18-20 Experiences of CPAP users with side effects were another factor of non-adherence.20,21 Note that these experiences were reported by adult patients with OSA. In children or adolescent patients with OSA, factors associated with non-adherence including sex, development status, and perception.22,23 Girls had higher rate of CPAP adherence than boys (56.5% vs 43.5%; P .01) and those with developmental delay had higher chance of CPAP adherence than those without developmental delay (odds ratio of 2.55; P .007). Additionally, perceptions or experiences with CPAP for non-adherence were some excuses such as does not use when away from home (47%), just want to forget about OSA (43.1%), not feeling well (42.0%), or forgets (39.2%).
Even though there are several factors for CPAP non-adherence, caregiver support, and BPAP may increase CPAP use almost 1 hour. A previous report found that children with OSA do not use CPAP because no one helps them to use CPAP at night in 31.4%. 23 Therefore, caregiver support may significantly improve CPAP adherence. Additionally, parents or caregivers may assist children to solve with some CPAP issues such as mask leakage. 24 BPAP, non-invasive ventilation, is more comfort than CPAP resulting in better adherence. 25 A previous study showed that BPAP had significantly used hours/night than CPAP (2.72 vs 1.49 hours, P < .001) in OSA patients with poor adherence to CPAP. 10 The patients using BPAP reported that BPAP is more comfortable than CPAP by visual analog scale (P .02).
There are some limitations in this study. First, there are no definite criteria for adherence in children. Criteria used in the included studies may be varied. Second, the maximum duration of follow up period was 1 year. Third, interventions had only 1 included study resulting in unable to calculate as a meta-analysis. Finally, some interventions are not studied such as educational intervention.
Conclusion
Caregiver support and BPAP therapy significantly improved CPAP adherence in children with OSA. Further studies are required to add additional comparisons and also other interventions.
Footnotes
Appendix
Searching Strategy for EBSCO (Retrieved on 15 February 2021).

| Search ID | Search terms |
|---|---|
| S1 | TI (obstructive sleep apnea or osa) OR AB (obstructive sleep apnea or osa) |
| S2 | TI sleep apnea syndrome* OR AB sleep apnea syndrome* |
| S3 | S1 OR S2 |
| S4 | TI compliance OR AB compliance |
| S5 | TI adherence OR AB adherence |
| S6 | (TI adherence OR AB adherence) AND (S4 OR S5) |
| S7 | TI (continuous positive airway pressure or cpap) OR AB (continuous positive airway pressure or cpap) |
| S8 | TI predict* OR AB predict* |
| S9 | TI independent OR AB independent |
| S10 | TI factor* OR AB factor* |
| S11 | TI variable* OR AB variable* |
| S12 | (TI variable* OR AB variable*) OR (S8 OR S9 OR S10 OR S11) |
| S13 | ((TI variable* OR AB variable*) AND (S8 OR S9 OR S10 OR S11)) AND (S3 AND S6 AND S7 AND S12) |
Author Contributions
BS conceived of the study, conducted the initial reviews, analyzed data, and composed the draft of the article. CN performed the article searches. CN and KS assisted with the reviews of the articles and their analyses and helped prepared the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.