
Abstract
The incidence of type 2 diabetes in children and adolescents in the United States rose at an annual rate of 4.8% between 2002-2003 and 2014-2015. Type 2 diabetes progresses more aggressively to complications than type 1 diabetes. For example, in one large epidemiological study, proliferative retinopathy affected 5.6% and 9.1% of children with type 1 and type 2 diabetes, respectively. Screening begins at age 10 or at onset of puberty, and is recommended among children with a BMI% ≥85 with risk factors such as a family history and belonging to a high risk racial or ethnic or racial group. HbA1C% is preferred for screening as it does not require fasting. As distinguishing between type 1 and type 2 diabetes is not straightforward, all children with new onset disease should undergo autoantibody testing. Results of lifestyle interventions for control of type 2 diabetes have been disappointing, but are still recommended for their educational value and the potential impact upon some participants. There is limited evidence for the benefit of newer mediations. Liraglutide, a GLP-1 agonist, however, has been shown to significantly reduce HbA1C% in one study and is now approved for children. Liraglutide should be considered as second line therapy.
We have known that the incidence and prevalence of type 2 diabetes in children and adolescents is steadily rising.
We provide an overview useful to clinicians which describes the epidemiology, diagnosis, prognosis, and treatment of type 2 diabetes, with an emphasis upon studies published in the past 5 years.
We believe more studies on newer type 2 diabetes agents are needed, to improve its prognosis in children and adolescents and the quality of life among those affected.
Introduction
The rising worldwide prevalence of childhood obesity is well known. 1 Roughly 18.5% of American children and adolescents had obesity in 2016 compared to 14.6% in 1999. 2 The problem also affects children in less developed countries. Data from 45 countries in Africa, for example, reveals an obesity prevalence of 6.9%. 3 Less well known is the related parallel increase in the incidence and prevalence of type 2 diabetes. Obesity increases the risk of incidence of type 2 diabetes in children and adolescents more than 4-fold. 4 Children from non-European backgrounds are severely affected. Among American Indian/Alaskan Native children 29.7% of whom have obesity, 5 for example, type 2 diabetes makes up 80% of all diabetes cases. 6 Affected children are more likely to suffer complications than children with type 1 diabetes. 7 Despite the magnitude of the problem, the problem remains unfamiliar to many clinicians. In one survey, albeit from 2003, just 15.3% of pediatricians felt well-prepared to manage type 2 diabetes. 8 Furthermore, significant gaps exist in our overall understanding of the epidemiology, prognosis, and treatment of type 2 diabetes in youth. Our goal was to summarize the most recently available epidemiological data, and to provide recommendations for diagnosis and treatment based on recent guidelines and studies. We reviewed available data from the Search for Diabetes in Youth (SEARCH) and Treatment Options for Type 2 Diabetes in Adolescents in Youth (TODAY) study, as well as other relevant published reports included in the PubMed database from 2015 to 2020. Data comes primarily from the United States, but our recommendations are broadly applicable.
Epidemiology
Epidemiological data comes primarily from SEARCH, a population-based, American registry and cohort study of youth onset (<20 years of age) diabetes of all types. Since 2001, incident and prevalent cases of youth-onset diabetes have been recorded across 4 geographical areas in the US including Native American reservations.6,9 Type 2 diabetes incidence and prevalence estimates are restricted to youth 10 to 19 years of age, due to few cases <10 years of age. 10
Prevalence is estimated every 8 years. In 2009 there were 46 cases of type 2 diabetes/100 000 youth (95% CI 31/100 000, 37/100 000). 11 American Indians had the highest prevalence (120 cases/100 000). Prevalence was lowest among non-Hispanic whites (17 cases/100 000) (Table 1). With the exception of American Indian and Asian Pacific Islander youth, the prevalence increased across all age, sex and racial and ethnic groups between 2001 and 2009, with an overall increase of 30.5%. Prevalence estimates for 2017 are still being calculated.
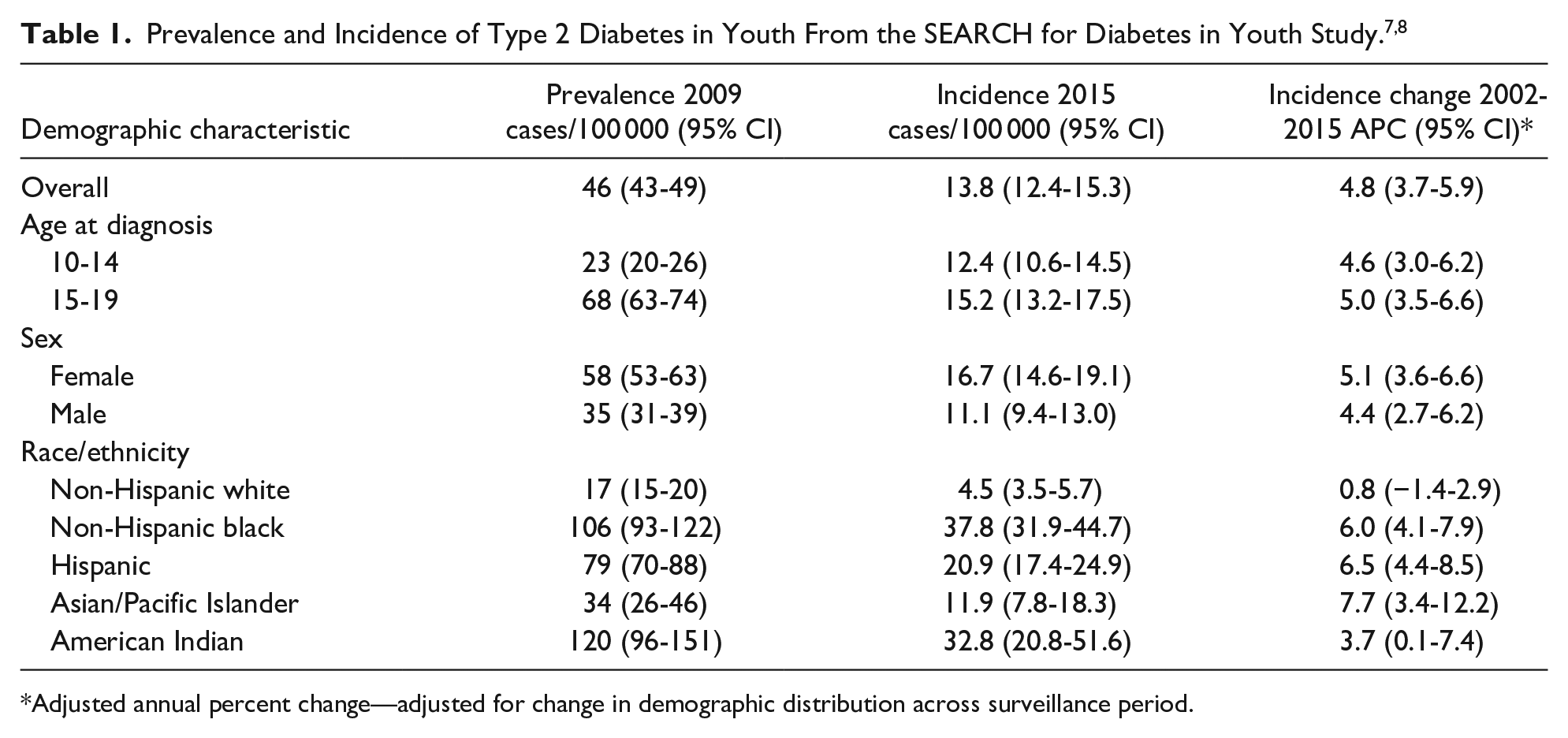
Adjusted annual percent change—adjusted for change in demographic distribution across surveillance period.
As opposed to prevalence, more recent incidence estimates are available. The 2014-2015 incidence was 13.8 cases/100 000. Incidence was higher in girls (16.7 cases/100 000) than boys (11.1 cases/100 000) and among older (ages 15-19 years (15.2/100 000)) versus younger (10-14 years (12.4/100 000)) participants. From 2002-2003 to 2014-2015, after adjusting for demographic changes, there was a 4.8% annual percent increase in incidence (Table 1). 7
What Have We Learned About Prognosis?
Our understanding of long term consequences is limited. Most evidence indicates that type 2 diabetes progresses aggressively. Relative to type 1 diabetes diagnosed in adolescence, children with type 2 diabetes are more likely to develop ≥1 complications as teens or young adults (72% vs 32%). 12 Specific complications are discussed below.
Peripheral Neuropathy
In SEARCH, 22% of participants with type 2 diabetes had evidence of clinical peripheral neuropathy 13 and 34% had evidence of subclinical diabetic peripheral neuropathy. 14 Male sex, smoking, lower HDL, and longer illness duration increased risk. 10
Kidney Disease
In SEARCH, kidney disease affected 19.9% of type 2 diabetes participants, comparable to the prevalence of 18% identified in the TODAY Study (see below for description). 15 Albuminuria progresses more rapidly among children with type 2 compared to type 1 diabetes. Risk factors for progression include poor glycemic control, lack of private insurance, African American race, and lower insulin sensitivity. 16
Retinopathy
In one pilot SEARCH study, the prevalence of any retinopathy was 42% among those with type 2 diabetes compared with 17% among those with type 1 diabetes. 17 In a larger SEARCH study, proliferative retinopathy was found among 9.1% of type 2 versus 5.6% of type 1 children with diabetes within just 5 to 10 years of diagnosis 13 —once again substantiating the relative aggressiveness of type 2 diabetes. Retinopathy was present in 13.9% of TODAY participants at the end of the study. 18
Cardiovascular Risks
Criteria for metabolic syndrome include hypertension, HDL cholesterol ≤1.0 mmol/L (40 mg/dL), triglycerides ≥2.8 mmol/L (110 mg/dL), and waist circumference >97th percentile. 19 In SEARCH, among youth with type 2 diabetes, at a mean participant age of 15.5 years, and mean disease duration of 2.6 years, 31.7% met criteria for metabolic syndrome. 14 This is comparable to the prevalence of metabolic syndrome among all children with obesity. 20
Arterial stiffness, a marker of vascular damage prognostic for atherosclerosis, was detected in 47.4% of SEARCH participants (mean age 22 years at assessment) and 50% of TODAY study participants.6,21
Autonomic dysfunction of the cardiovascular system (CAN) is a significant risk factor for cardiovascular morbidity. CAN is diagnosed based on an abnormal response to a series of cardiovascular autonomic reflex tests. CAN affects roughly 20% of adults with diabetes and is associated with a 5-fold increase in mortality.22,23 In SEARCH, among participants with a mean (SD) disease duration of 8 (±2) years, 17% met criteria for CAN. Risk factors included elevated triglycerides and albuminuria. 24
Mortality
Through linkage of SEARCH and the U.S. National Death Index data through 2010, and among type 2 diabetes participants diagnosed from 2002 to 2008, the mortality rate was 185.6 deaths/100 000 person-years as compared to an expected mortality rate of 70.9 deaths/100 000 person-years. The age, sex, and race-standardized mortality ratio was 2.4 (95% CI: 1.3-3.9) for type 2 diabetes participants. By contrast, no increase in mortality was observed for type 1 participants. 25
Diagnosis
Screening and Diagnostic Criteria
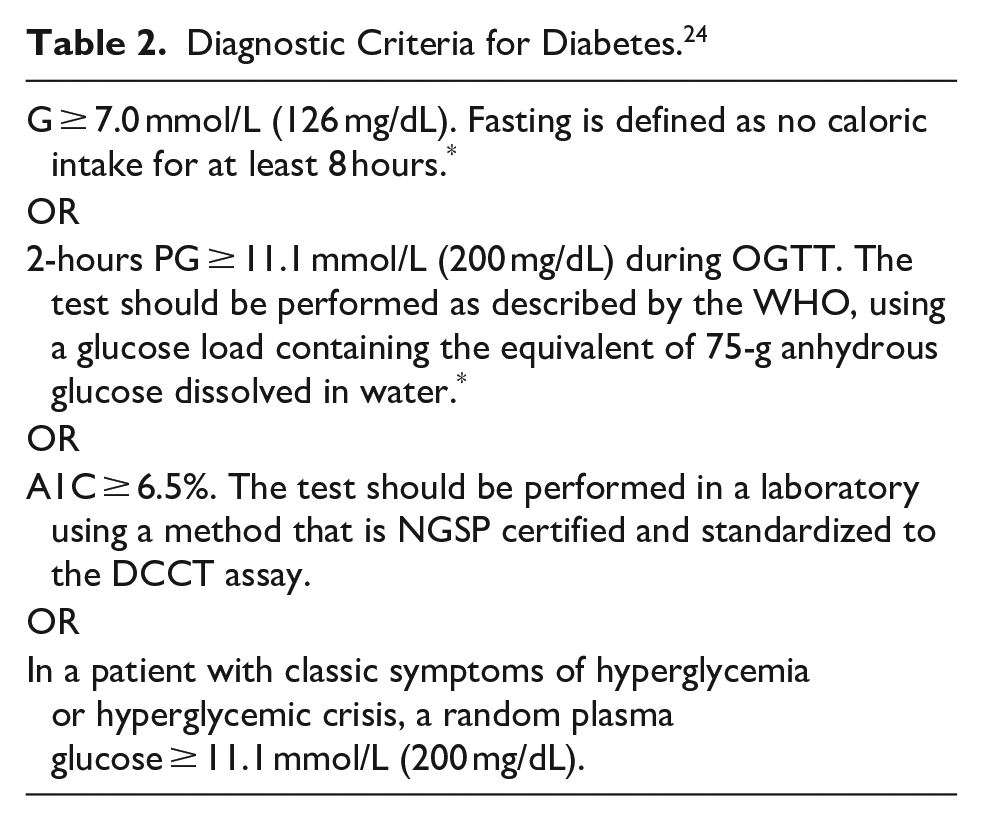
Criteria are nearly uniform among different international guidelines.26-28 Screening begins at age 10 or at puberty if it occurs earlier and should be based on the presence of risk factors, which include overweight or obesity (BMI ≥ 85th percentile) plus ≥1 additional risks. Additional risks include: maternal gestational diabetes; a family history of type 2 diabetes (first or second degree relative); belonging to a specific race or ethnicity. In the US, these include Native American, African American, Latino, Asian American, and Pacific Islander; and signs of insulin resistance and associated metabolic conditions including acanthosis nigricans, hypertension, dyslipidemia, polycystic ovaries syndrome (PCOS) or small for gestational age birth weight. 5 Screening should be repeated every 3 years, or more frequently if BMI is increasing rapidly. 5 A diagnosis can be made based upon fasting plasma glucose, the 2-hour oral glucose tolerance test, HbA1C% level, or random glucose in the presence of typical diabetes symptoms. Diagnostic criteria are well established and are summarized in Table 2. 29 These are based on adult criteria and have not been validated in children. The usefulness of HbA1C% level, in particular, has come under a great deal of scrutiny. Several studies have shown poor sensitivity when compared to the oral glucose tolerance test (OGTT).30-32 By contrast, Chan et al 33 reported that both OGTT and HbA1C% predict free-living glycemia equally well. No long-term studies have demonstrated the correlation between HbA1C% in children and diabetes outcomes. However, this is also true for the other tests. 34 All things considered, as studies confirming the long-term validity of diagnostic criteria are unlikely to emerge in the near future, we believe clinicians should rely on recommended criteria. As HbA1C% does not require fasting, it is often easier to perform in children 35 and has been associated with higher screening rates. 36
Diagnostic Criteria for Diabetes. 24
Distinguishing Between Type 1 and Type 2 Diabetes
Distinguishing between type 1 and type 2 diabetes in children can be challenging. The classic type 1 diabetes phenotype of a thin child who presents with diabetic ketoacidosis (DKA) is valid, but many children with type 1 diabetes also have overweight or obesity. Also, roughly 11% of children with type 2 diabetes present with DKA. 37 The presence of specific autoantibodies including islet antigen-2 antibody (IA-2), glutamic acid decarboxylase-65 antibody (GAD65), and insulin autoantibody (IAA), which indicate the pancreatic B-cell destruction, can be useful in distinguishing diabetes type. 38 Even here, many children with a clinical phenotype consistent with type 2 diabetes have autoantibodies. For example, among 1206 children initially assessed for enrollment in the TODAY study, 9.8% were antibody positive. These children were, however, less likely to be obese and more likely to require insulin sooner and therefore bore more resemblance to typical children with type 1 diabetes. 39 For these reasons, it is recommended that autoantibody testing be considered in all children with a new diagnosis of diabetes, with one or more positive antibody test strongly indicative of type 1 diabetes or antibody-positive type 2 diabetes. 6 A reasonable autoantibody testing panel includes GAD65 with at least one of IA-2, IAA, islet cell cytoplasmic antibody IGG, (ICA), or zinc transporter 8 antibody (ZnT8). 40
Monogenic Diabetes
Though rare, clinicians should be familiar with monogenic diabetes which is in the differential diagnosis of type 2 diabetes.
Unlike type 1 and type 2 diabetes, monogenic diabetes is inherited in an autosomal dominant fashion. It includes neonatal diabetes and different forms associated with mutations in 14 genes known as maturity-onset diabetes of the young (MODY). MODY is often misdiagnosed as type 1 or type 2 diabetes. It represents approximately 1.2% of cases of pediatric diabetes. 41 Neonatal diabetes represents an additional 0.2% of cases. 42 Most individuals with MODY are non-obese, diagnosed before age 25, and have a parent with MODY. 43 Pancreatic autoantibodies are absent and C-peptide is detectable 3 to 5 years after diagnosis. 44 Next generation genetic testing should be considered under such circumstances. Treatment depends upon MODY subtype. For example, glucokinase-maturity-onset diabetes of the young (GCK-MODY) is characterized by only mild hyperglycemia requiring no treatment. By contrast, the most common type, hepatocyte nuclear transcription factor 1A-maturity-onset diabetes of the young (HNF1A-MODY) is characterized by insulin secretory defects, and microvascular complications are strongly related to glycemic control. 45 Further details about monogenic diabetes are beyond the scope of this review.
Treatment
Lifestyle Approaches
Among newly diagnosed children, lifestyle management is the recommended initial approach.20,21 This should include encouragement of healthy eating, 30 to 60 minutes of moderate or vigorous physical activity ≥5 days/week, and strength training ≥3 days/week. Also recommended is comprehensive diabetes education and self-management support. Unfortunately, the likelihood of successful control through lifestyle intervention is low. Even among adults in one large study, only 3.5% were able to achieve diabetes remission through an intensive lifestyle-based intervention after 4 years. 46 A large proportion of youth with type 2 diabetes fail to achieve a healthier weight or improved control. 47 Adherence by children in non-research settings is a significant issue. In a study of non-Hispanic black youth in New York with type 2 diabetes, 39% dropped out of medical care within 2 years, and 78% within 5 years. 48
Lessons From TODAY and Other Studies
The TODAY study was a multiethnic, multicenter randomized trial which compared 3 treatment approaches in obese children age 10 to 17 with type 2 diabetes: metformin alone; metformin plus the thiazolidinedione rosiglitazone; and metformin plus an intensive lifestyle intervention. 49 The TODAY lifestyle program (TLP) was designed to promote a weight loss of 7% to 10% of initial weight through counseling. 50 The primary outcome was treatment failure, defined as a persistently elevated HbA1C% ≥8%. Rates of failure were 51.7%, 38.6%, and 46.6% for metformin alone, metformin plus rosiglitazone, and metformin plus TLP, respectively, with no statistically significant difference between metformin alone and metformin and TLP. A decrease of at least 7 percentage points in percent overweight for individual enrollees was considered to be clinically meaningful. This degree of reduction after 6 months was achieved in 31.2% in the metformin plus TLP group, 16.7% in the metformin plus rosiglitazone group, and 24.3% in the metformin alone group. The difference between the metformin and metformin plus TLP groups was not statistically significant.
The discouraging impact of lifestyle changes in the TODAY study is echoed by the huge number of published studies of treatments for overweight and obesity in general. In a comprehensive overview of 6 Cochrane systematic reviews, Ells et al 51 reported that multi-faceted behavior change programs can have at best a modest impact upon weight status in children and that overall reports of effectiveness show no improvement since 2009. However, we still support recommending lifestyle changes. First, lifestyle management programs do not generally have adverse effects. 27 Second, even if participation and engagement is poor by youth and families, they are still likely to receive some useful information about what changes are beneficial. Finally, type 2 diabetes has an enormous impact upon a child’s current and future health. It is hard to predict which children will benefit significantly from a lifestyle management program. A highly positive impact on a small number of children can be viewed as a success, even if the majority of children do not achieve improved outcomes. We do advise clinicians to be realistic about the success of lifestyle management, and to recognize that many children will require pharmacotherapy.
Newer Pharmacotherapies
The newer classes of diabetes medications include glucagon-like peptide 1 (GLP-1) agonists, dipeptyl peptidase -4 (DPP-4) inhibitors, and sodium-glucose co-transporter-2 (SGLT2) inhibitors. Newer agents have revolutionized adult diabetes care. The SGLT2 inhibitors, for example, have been shown not only to control diabetes, but also to improve renal and cardiovascular outcomes. 52 Newer agents were not available at the time of the TODAY study, nor are they explicitly recommended in current guidelines. The evidence base is, however, growing.
GLP-1 agonists improve glucose control through enhanced insulin secretion, suppression of glucagon secretion, and delaying gastric emptying. They also promote weight loss. 53 In 2019, the results of a trial comparing the GLP-1 agonist liraglutide plus metformin to placebo plus metformin among 134 children with type 2 diabetes who were receiving metformin with or without insulin, were published (Ellipse trial). After 26 weeks, HbA1C% declined by 0.64 points in the liraglutide arm compared with an increase of 0.42 points in the placebo arm (difference of −1.06, 95% CI, −1.65 to −0.46). 54 Moreover, in June 2019, liraglutide became the first GLP-1 agonist approved for type 2 diabetes treatment in children and the first non-insulin treatment approved for children since metformin was approved in 2000. 55 It is administered daily subcutaneously which may limit acceptability. Gastrointestinal side effects are common. It is very expensive (retail cost >$1100 per month). 56 An oral form of the GLP-1 agonist, semaglutide, has recently become available but has not been studied in children. 57 Studies of other newer agents are very limited in number and include primarily only pharmacokinetic/pharmacodynamic and safety outcomes. Based on a search of ClinicalTrials.gov, Table 3 summarizes 3 clinical trials of newer agents with outcomes (including the Ellipse trial).
Studies of Newer Agents for Type 2 Diabetes in Children.

Clinicaltrials.gov. Bethesda (MD). National Library of Medicine. Identifier NCT01204775. Study to evaluate the efficacy, safety, tolerability, and pharmacokinetics of saxagliptin as monotherapy in pediatric patients with type 2 diabetes. April 18, 2017. Cited January 1, 2020. https://www.clinicaltrials.gov/ct2/show/study/NCT01204775?term=pediatric+type+2+diabetes&cond=saxagliptin&draw=2&rank=1
Clinicaltrials.gov. Bethesda (MD). National Library of Medicine. Identifier NCT01434186. A multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of saxagliptin (BMS-477118) in combination with metformin IR or metformin XR in pediatric patients with type 2 diabetes who have inadequate glycemic control on metformin alone. April 18, 2017. Cited January 1, 2020. https://www.clinicaltrials.gov/ct2/show/results/NCT01434186?term=bms-477118&draw=2&rank=2
Given the aggressiveness of type 2 diabetes and the promising results with liraglutide and other agents, we believe strongly that newer agents should be considered as second-line treatment after metformin and prior to or along with insulin. We also believe that more GLP-1 agonists, DPP-4 inhibitors, and SGLT-2 inhibitors will be approved for use in children, transforming care for type 2 diabetes just as they have among adults.
Research Gaps
Type 2 diabetes appears to follow a more aggressive course than type 1 diabetes in youth. Many questions remain, however, about the long term impact. For example, it is unknown how early onset type 2 diabetes affects reproductive health and the health of offspring.
Lifestyle approaches to management of type 2 diabetes have so far proven disappointing. New strategies are needed to engage children and families in sustainable lifestyle changes for better control and to slow disease progression. As non-European children are at high risk, new culturally sensitive approaches which take into account dietary and taste preferences, eating patterns and other factors are essential.
Finally, the options available for pharmacological treatment of type 2 diabetes in youth are expected to increase rapidly in the coming years. There is a need for studies of additional GLP-1 agents, SGLT-2 inhibitors, and DPP-4 inhibitors in youth with type 2 diabetes.
Footnotes
Author Contributions
GR and ETJ contributed equally to the conception, design, analysis and interpretation of data, drafting, and revising of this review article. Both authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.