
Abstract
This study compared the prevalence of chronic pediatric health conditions for youth in public housing with youth not in public housing using clinical electronic health record (EHR) and housing data. Youth (ages 2-17 years) in a large urban health system were identified and categorized into two housing types—public housing (n = 10 770) and not in public housing (n = 84 883) by age (young childhood, middle childhood, young adolescence). The prevalence of some pediatric conditions was higher in public housing but varied by age. Disparities in health conditions among youth in public housing were more common in early adolescence: asthma (26.4 vs 18.6; P < .001); obesity (28.5 vs 24.6; P < .001); depression/anxiety (19.2 vs 17.3; P = .008); behavioral disorders (8.1 vs 5.3; P < .001). These results show that chronic pediatric conditions like asthma and obesity that lead to significant morbidity into adulthood are more common among youth living in public housing. However, this pattern is not consistent across all chronic conditions.
Introduction
The health goals outlined for the U.S. in Healthy People 2030 identifies housing and housing insecurity as a key social determinant of health. 1 Aligned with this goal, the American Academy of Pediatrics recommends routine screening for housing status in its 2016 policy statement (American Academy of Pediatrics, 2016). 2 The housing environment has long been known to be an important factor in early development where harmful exposures can influence health into adulthood.3,4 The US Department of Housing and Urban Development (HUD) administers Federal aid to local housing authorities that manage low-income housing options (ie, public housing) for eligible residents. Public housing is typically located in economically underserved and under resourced areas and generally characterized as a place of concentrated poverty with physical, social, and economic barriers to prioritizing health behaviors and managing chronic health conditions among residents. The prevalence of chronic illnesses like asthma, obesity, and heart disease among adults living in public housing (and other federally subsidized housing)5 -9 are higher than low-income residents not in public housing. Except for an extensive literature on asthma and lead poisoning, chronic conditions among children living in public housing are less frequently examined.10 -15 If the burden of chronic conditions among adults is any indication, children living in public housing are also likely to suffer disproportionately from chronic conditions. There is some evidence that youth living in public housing are at risk for health problems like unintended injuries,16,17 mental health problems,18,19 and less access to behavioral health services. 20 Fortunately, likely due to concerted health care delivery efforts, children living in federally assisted housing (including public housing) are more engaged in primary care than other low-income children. 20 While identifying patients in the clinical setting can be an ideal touchpoint to engage this high-risk population, most clinical practices are not equipped to assess or mitigate their social needs. Addressing these health concerns among public housing populations requires multi-level engagement from various stakeholders to identify and target at-risk families including clinical, social, and policy sectors. In addition, community-based organizations and government agencies including housing authorities that serve these communities rely on health data to inform their collaborative programming agendas and evaluate the success of interventions. Linking health system data from electronic health records (EHR) with data on housing and neighborhood may provide an opportunity to provide information that can inform the efforts of partnerships to address the health needs of public housing residents particularly children.
The current study used residential address data of a large urban health system in the Bronx, NY to identify youth living in public housing seen in the primary care setting. The objective of the study was to compare the prevalence of major chronic pediatric conditions across the age range of early childhood to early adolescence living in public housing and those not in public housing using data captured in the EHR. The hypothesis was that public housing is a key risk factor for major chronic pediatric conditions and disparities in prevalence can be observed early in childhood.
Methods
Study Sample and Population
All youth (ages 2-17 years) with ≥ 1 primary care outpatient visit between November 1, 2016 and October 31, 2018 were identified in the EHR for inclusion in the study sample using Looking Glass™ Clinical Analytics (Streamline Health, Atlanta, Georgia). 21 Primary care was defined as visits to internal medicine, family medicine, pediatrics, and non-specialty obstetrics/gynecology departments. While the sample was defined by the patients having a primary care visit during the study timeframe, outcome data could come from any encounter, including primary care, specialty care, urgent care, emergency department (ED), or inpatient settings. The study was approved by the Albert Einstein College of Medicine Institutional Review Board.
The data were geocoded in ArcGIS using the New York State Street and Address Composite geocoding services tool. The initial sample consisted of 112 020 youth ages 2-17. Geocoding matches were made for 97.2% of patients (n = 108 882). Of these patients, 95 653 resided in Bronx County, NY and were included in analyses.
Measures
Health conditions
Common chronic pediatric conditions were included in our analysis and data for these variables were extracted from the EHR. Patients were identified as having a given condition if they had a diagnosis code in their record between November 1, 2016 and October 31, 2018. Detailed descriptions of these health conditions can be found in Table 1. All health conditions, except for obesity and overweight, were identified using International Classification of Diseases, 10th edition (ICD-10) diagnosis codes. In cases where multiple ICD-10 codes were used to characterize a health condition, we referred to prior studies examining health outcomes using clinical data for case definitions. 22 To identify patients that were obese or overweight, we extracted the latest measured body mass index (BMI) from clinical records (Table 1).
Health Conditions and Definitions.

Defined as occurring between November 1, 2016 and October 31, 2018
Public housing and covariates
Public housing
Public housing is defined as a housing property managed by the New York City Housing Authority (NYCHA) and receiving aid from HUD to provide low income rental units to eligible patients. The criteria for eligibility is available on the NYCHA website. To identify individuals residing in public housing, each patient’s residential address was first geocoded. A tax lot shapefile from the PLUTO NYC database was then joined with a map of NYC public housing developments, which then identified the tax lots associated with public housing. 23 If their residential address geocoded to public housing-associated tax lots, patients were flagged as living in public housing. All other patients were considered not to reside in public housing.
Covariates
Individual-level data were extracted from the EHR using Looking Glass™ Clinical Analytics. 21 We include age at outpatient visit (early childhood: 2-5 years, middle childhood: 6-10 years, early adolescence: 11-17 years), sex, race/ethnicity (Hispanic, non-Hispanic black, non-Hispanic white, non-Hispanic Asian/Pacific Islander, a combined other category, and a missing indicator), and payer type (Medicaid, Medicare, commercial insurance, none or missing data). Due to the limited number of individual socioeconomic status variables, area-based poverty at the Census block group level was included as a covariate, specifically the percentage of the population living below the poverty level. Due to concerns about missing individual race/ethnicity data, data on area-based race/ethnicity, also at the Census block group level, was included. Area-based poverty and race/ethnicity data came from the 2012-2016 American Community Survey and were collected at the block group level, the smallest unit of geography for which this data is available. 24 Patients who were geocoded to block groups with zero population according to the Census (n = 124) were excluded from analyses that included these area-level variables.
Analysis
We first tested for differences in the characteristics of youth living in public housing versus those who did not using chi-squared tests. Then, for each outcome, we estimated separate fully-adjusted logistic regression models for each age group (early childhood, middle childhood, early adolescence) to assess whether these relationships may vary by age for those who lived in public housing versus those not living in public housing. These analyses also accounted for clustering of individuals within Census block-groups. Multivariable-adjusted prevalence estimates are presented with 95% confidence intervals. All statistical analyses were completed using Stata 13.1 (StataCorp, College Station, TX) and mapping was done in ArcGIS 10.3 (Environmental Systems Research Institute, Redlands, CA). Statistical significance was determined at the P < .05 level.
Results
Eleven percent (11.3%) of the study population lived in public housing. Youth who lived in public housing were more likely to be Black or Hispanic and insured through Medicaid. They were also more likely to live in more racially segregated areas (ie, larger percentage of area residents are Black or Hispanic) and where a greater percentage of the population lives below the poverty line (Table 2).
Patient and Neighborhood Area Characteristics by Housing Type.
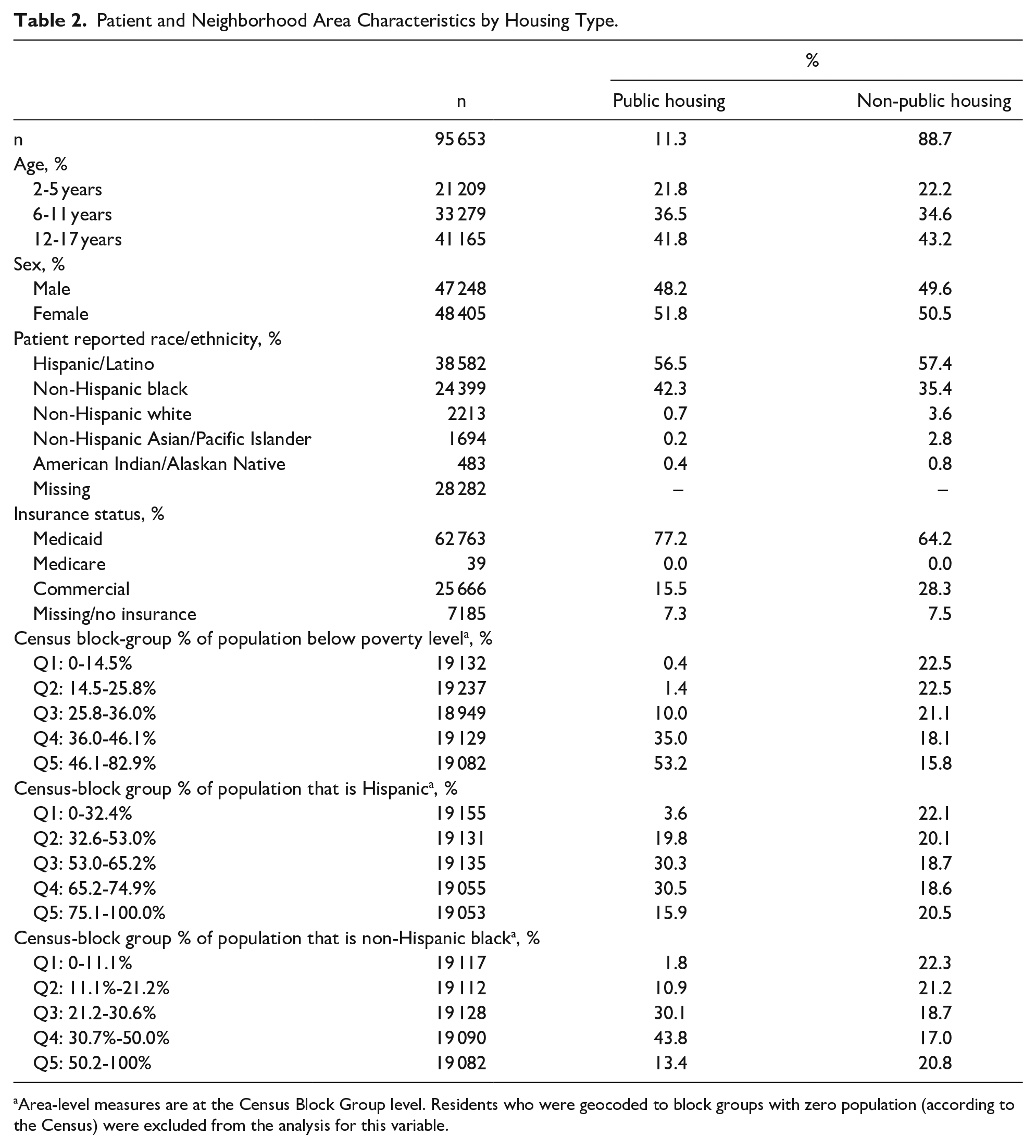
Area-level measures are at the Census Block Group level. Residents who were geocoded to block groups with zero population (according to the Census) were excluded from the analysis for this variable.
Table 3 shows the relationship between housing type in age-specific analyses. The prevalence of asthma was higher among youth living in public housing across all age groups (early childhood: 19.9 vs 15.9, P < .001; middle childhood: 31.1 vs 23.5, P < .001; early adolescence: 26.4 vs 18.6, P < .001). The prevalence of obesity was higher in early childhood (19.0 vs 16.9, P < .05) and early adolescence (28.5 vs 24.6, P < .001) living in public housing compared to the same age groups not living in public housing (Table 3). Youth in middle childhood (8.9 vs 7.0, P < .001) and youth in early adolescence (19.2 vs 17.3, P < .01) living in public housing had a higher prevalence of anxiety/depression, albeit small and not clinically significant, than youth from those age groups not living in public housing. The prevalence of behavioral disorders was slightly higher among youth in public housing across all age groups than their counterparts not living in public housing (early childhood: 2.9 vs 2.2, P < .05; middle childhood: 10.9 vs 9.0, P < .01; early adolescence: 8.1 vs 5.3, p < .001). Contrary to direction of the relationship observed with the other health outcomes, youth in early adolescence living in public housing had a lower prevalence of unintentional injuries (17.0 vs 18.8, p < .05) than youth in early adolescence not living in public housing.
Multivariable-Adjusted Prevalence of Pediatric Health Conditions with 95% Confidence Intervals (95%CI) by Housing Type and Age Group.

Adjusted for sex, area-based poverty, area based % non-Hispanic black, area-based % Hispanic, insurance status, individual race/ethnicity. Multivariable-adjusted analyses account for clustering of individuals within census block-groups.
Discussion
This study was designed to compare the prevalence of chronic health conditions among youth patients seen in our primary care setting living in public housing to youth patients not living in public housing. Our results confirm findings from other reports showing a higher prevalence of asthma and obesity among public housing residents.20,14 Our results show that this relationship is consistent across age groups and increases with older age. As expected, we also showed that mental health problems are statistically more prevalent among youth in public housing, particularly for youth in middle childhood and early adolescence. Behavioral disorders were higher among youth in public housing particularly among youth in early adolescence. Somewhat surprising were the results showing a relatively small difference in prevalence of unintentional injuries between housing types except for youth in early adolescence, where the prevalence was lower among youth in public housing. Other chronic health conditions that were not higher among youth in public housing compared to youth not living in public housing were “other dermatitis/eczema”-with exception of a small difference among youth in early adolescence-, “other unspecified allergies,” “overweight,” and “diabetes.”
The increased risk for asthma and related hospitalizations among public housing residents has been the focus of many public health and primary care efforts but remains persistent among youth in public housing.25 -27 The increase in obesity with age in our study mirrors population trends and shows that the disparity begins in early childhood. Given that a larger proportion of youth in federally assisted housing attend well visits than the general population (84% vs 77%), these results highlight a potential window for more targeted interventions to reach youth in public housing while they are still engaged in primary care.20,28 -30
The results of our study show a higher, albeit small in younger age groups, prevalence of depression/anxiety and behavioral disorders among youth in public housing than their counterparts not in public housing. The higher prevalence of mental health conditions among youth in public housing in our study is consistent with other reports of poor mental health and poor access to mental health services among children residing in public housing and in low quality housing more broadly.20,31 Data from the U.S. Department of Housing and Urban development show that youth in households that receive federal rental subsidies have inadequate access to mental health services compared to other health care services. 20 This unmet need, taken together with the data in this study showing a higher prevalence of behavioral disorders in youth living in public housing and the national data showing an increase in diagnoses of anxiety and ADHD in youth, 32 suggest that further emphasis on integrated mental health services should be a priority for health care delivery with particular attention to youth in high risk living conditions. An example of such integrative partnerships, the Montefiore Behavioral Health Integration Program (BHIP) is a partnership between primary care physicians and behavioral health providers, and includes a mental health evaluation as a part of a full medical evaluation (cite Montefiore BHIP program as a potential model). Through BHIP, patients are also able to meet confidentially with behavioral health providers during primary care visits. Services include screening, diagnosis, and treatment (including individual counseling and group therapy) for both adults and children. Another example of health care systems and community collaborations meeting this need can be seen through Home and Community Based Services (HCBS) Medicaid waivers, 33 which extends the reach of Medicaid (public health care insurance for low-income residents) to provide mental health services for youth whose family incomes exceed the Medicaid limit.
Unintended injuries are the leading cause of morbidity and mortality among youth in the US. 34 Somewhat surprising in our study was the lower burden of unintended injuries among youth in early adolescence living in public housing. This was unexpected given reports of more hazardous conditions and maintenance deficiencies in public housing residences that could increase the risk for accidents in and around the home. 35 The difference in prevalence, albeit small, is important to consider when evaluating overall health concerns among youth.
Study Limitations
This study is cross sectional so the temporal relationship between housing type and health conditions cannot be determined. While studies show that the quality of low-income housing may influence the chronic health conditions observed in this study, 14 it is also possible that residents with chronic conditions are more likely to seek out residence in public housing and are ill prior to their public housing tenure. 36 Although the adjusted analyses attempt to address potential confounding by including individual and neighborhood-level factors, there are likely unmeasured factors that may make public housing residents appear less healthy than residents not in public housing. Another limitation of this study is that our non-public housing group is quite broad and contains many other housing arrangements including potential homelessness. While we are attempting to better define housing type in our clinical cohort, we are unable to do so for this analysis. Lastly, the use of diagnosis codes from the EHR, especially for mental health and behavioral health conditions, is a potential limitation as some conditions may not be a part of systematic screening. 37 While this is a concern when using these data, we do not expect this bias to be differential. Missing data is also a common concern in EHR data. 38 In Tables 1 and 2, we report the percentage of missing covariate data but we did not make any attempt to use analytic methods (eg, multiple imputation) to address missing data apart from including this “missing” category in multivariable analyses. Despite these limitations, our study has the advantage of a large sample size of children seen in primary care, reports on a broader range of health conditions among youth in public housing than prior studies, 20 and uses objectively measured health outcomes that do not rely on self-report.20,39
Conclusion
Our study provides data on one health system in a focused geographic area aimed to support collaborations between health systems and community-based organizations to improve health outcomes for residents. For many years, federal housing budgets have been stretched thin and have to prioritize management and maintenance operating costs over connecting residents to necessary health services. 40 Partnerships between housing authorities and health systems can pick up the slack and have the potential to improve the health outcomes for patients in public housing. Examples of such partnerships between primary care and housing authorities include Public Housing Primary Care 41 and the Chicago Family Case Management Demonstration. 42 These partnerships provide linkages to increase access to health care options for public housing residents. Identifying the housing-related needs of young patients is a necessary step to developing clinical-community partnerships to improve health among residents.9,43,44
Footnotes
Author Contributions
ECC: conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript.
CH: carried out the initial analyses, and reviewed and revised the manuscript.
KM and KF: critically reviewed and revised the manuscript for important intellectual content.
CDR: coordinated and supervised data management and analysis, and critically reviewed the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Heart, Lung, and Blood Institute (NHLBI) grants K01HL125466 and 1R03HL140265. Dr. Fiori was supported by AHRQ K12 funding (# HS026396).
Ethics Statement
The Institutional Review Board (IRB) of the Albert Einstein College of Medicine/ Montefiore Health System approved this study protocol (IRB- 2016-6669).