
Abstract
In contrast to patients with an apparent life-threatening event (ALTE), the American Academy of Pediatrics recommends very limited evaluation for patients categorized as lower-risk brief resolved unexplained event (BRUE). This retrospective review aims to explore potential missed diagnostic opportunities for patients with a lower-risk BRUE (n = 10) through comparison with a subset of patients with ALTE (n = 72). None of the patients with a lower-risk BRUE had laboratory, imaging or ancillary studies that were diagnostic. Among patients with ALTE, 5 had laboratory and 3 had imaging studies that were diagnostic. None of the patients with a lower-risk BRUE had recurrent events during hospitalization or a serious underlying diagnosis identified within the 90 day follow-up period. As recommended by the AAP, patients with a lower-risk BRUE do not need diagnostic evaluation and can be discharged home with outpatient follow-up.
Keywords
Introduction
Parents commonly seek care for their infants following frightening yet transient changes in their breathing, color, tone or mental status. Termed “apparent life threatening events” (ALTE), these infants historically underwent a varied diagnostic evaluation and were hospitalized.1-4 To standardize the approach to these infants, the American Academy of Pediatrics (AAP) published a clinical practice guideline where they retire the term ALTE, define a brief resolved unexplained event (BRUE), provide an approach to risk stratification, and offer recommendations for the evaluation and management of patients categorized as lower-risk. 5 The rate of diagnostic testing for patients with a BRUE has declined since publication of the clinical practice guideline, but few studies have examined whether a shift toward the limited testing suggested by the AAP results in missed diagnostic opportunities.6,7 Thus, the aim of this study is to examine the yield of diagnostic testing in patients with a lower-risk BRUE in comparison to patients with ALTE.
Methods
Study Design
This retrospective study was conducted at an inner-city free-standing children’s hospital with a level 1 trauma center and approximately 80 000 pediatric emergency department (PED) visits annually.
Ethical Approval and Informed Consent
This study was approved by the institutional review board (IRB) at Wayne State University (IRB# 021817MP4E).
Selection of Participants
Patients ≤ 365 days of age seen in the PED between January 1, 2010 and April 30, 2016 with an International Classification of Diseases (ICD), Ninth or Tenth Revision discharge diagnostic code consistent with a BRUE were reviewed. 8 Patients with co-morbid conditions or insufficient PED documentation were excluded. Using medical record review, patients were categorized as BRUE, ALTE or “other” by one author (RH) using published definitions for BRUE and ALTE.1,5 Categorizations were confirmed by a second author (AD). Patients with BRUE were then stratified as lower-risk based upon published criteria. 5 Discrepancies were resolved through consensus (RH, AD). Patients categorized as “other” were excluded from further review. A subset of patients with ALTE was selected based upon key demographic characteristics to align with patients stratified as lower-risk BRUE. The demographic characteristics used in this process were age (±15 days), gender, and season of presentation (winter, spring, summer, fall). Season of presentation was included to account for the known seasonal variability in pediatric viral illnesses. 9 The electronic medical record for all patients with a lower-risk BRUE and the identified subset of patients with ALTE was reviewed in detail using a standardized data collection form. Data for the index visit and any return visits to our institution within 90 days were abstracted. Data accuracy was verified by 2 authors (RH, SP) with ambiguous elements reviewed by 2 authors (RH, AD). Study data were collected and managed using Research Electronic Data Capture (REDCap). 10
Definitions
ALTE: An ALTE was defined as “an episode that is frightening to the observer that is characterized by some combination of apnea, color change, marked change in muscle tone, choking, or gagging.” 1
BRUE: A BRUE is a sudden, brief, and now resolved episode in a well appearing infant <1 year of age comprising one or more of: (1) cyanosis or pallor; (2) absent, decreased, or irregular breathing; (3) marked change in tone or (4) altered responsiveness. Patients with additional symptoms, abnormal vital signs for age, or an explanation for the event based upon the documented history and/or physical examination do not meet the definition of BRUE and were therefore not classified as a BRUE. Patients were further stratified as lower-risk if they: (1) were >60 days age; (2) had no history of prematurity or were born 32 to 37 weeks gestation with a corrected gestational age of ≥45 weeks; (3) did not have cardiopulmonary resuscitation performed by a medical provider; (4) had an event <1 minute in duration and (5) had a single event. 5
Diagnostic testing: Laboratory studies were interpreted as normal or abnormal using published reference ranges, with values falling outside of these ranges classified as abnormal. 11 Imaging studies and electroencephalograms (EEGs) were categorized as normal or abnormal based upon the interpretation provided in the institutional electronic medical record. Electrocardiograms (ECGs) were reviewed by a pediatric cardiologist and classified as normal or abnormal. Abnormal studies were considered diagnostic or clinically significant if they led to a change in patient management or contributed to a specific diagnosis.
Outcomes
The primary outcome of interest was the yield of diagnostic testing in patients with a lower-risk BRUE compared with patients with an ALTE. Secondary outcomes included recurrent events during the index encounter, a return hospitalization for an ALTE/BRUE, or a serious underlying diagnosis identified within 90 days of the index PED visit.
Statistical Analysis
We summarized and reported the categorical variables by numbers and percentages. We analyzed normally distributed continuous variables by mean and standard deviation, whereas non-normally distributed continuous variables are reported by median and interquartile range (IQR). We used SAS (version 9.4, SAS Institute Inc. Cary, North Carolina) to perform the statistical analyses.
Results
A total of 3325 charts were identified and 661 (20%) were excluded: 644 (97%) had a co-morbid condition and 17 (3%) had insufficient ED documentation. Of the remaining 2664 charts, 1204 (45%) met the definition for ALTE, but not BRUE, due to choking (655/1204; 54%), abnormal vital signs (316/1204; 26%), or an abnormal history or physical exam (233/1204; 19%). 98 (4%) met the definition for BRUE of which 10 (10%) were classified as lower-risk. Patients with a higher-risk BRUE are reported separately. 8 From the ALTE patients, 72 (6%) were identified who met the aforementioned criteria and were compared to the 10 patients with a lower-risk BRUE.
Demographics
Patients with a lower-risk BRUE were African American (80%) males (50%) with a median age of 128 days (IQR: 113, 300). One-third (30%) were transferred from another ED and 70% were hospitalized. Patients with ALTE were significantly younger (P = .03) but otherwise there were no differences in the demographic characteristics of patients with a lower-risk BRUE or an ALTE (Table 1).
Demographic Characteristics.

Includes nurse practitioner and physician assistant.
Diagnostic Evaluation
There were no significant differences in the number of individual laboratory, imaging or ancillary tests performed for patients with a lower-risk BRUE or an ALTE (Table 2). Overall, 8/10 (80%) of patients with a lower-risk BRUE had laboratory testing performed, but none of the 64 tests were diagnostic. Conversely, 59/72 (82%) of patients with ALTE had laboratory tests performed of which 5/543 (0.9%) were diagnostic. One patient was diagnosed with Bordetella pertussis, and 4 patients were diagnosed with respiratory syncytial virus. Most patients with a lower-risk BRUE (7/10; 70%) and ALTE (55/72; 76%) had imaging performed, but none were diagnostic for patients with a lower-risk BRUE. In contrast, 3/68 (4%) imaging studies were positive for patients with ALTE, with 3 chest radiographs consistent with pneumonia. Ancillary studies were performed in fewer patients (lower-risk BRUE 2/10, 20%; ALTE 21/72, 29%) and were never diagnostic (Figure 1; Table 2).
Laboratory, Imaging and Ancillary Studies.
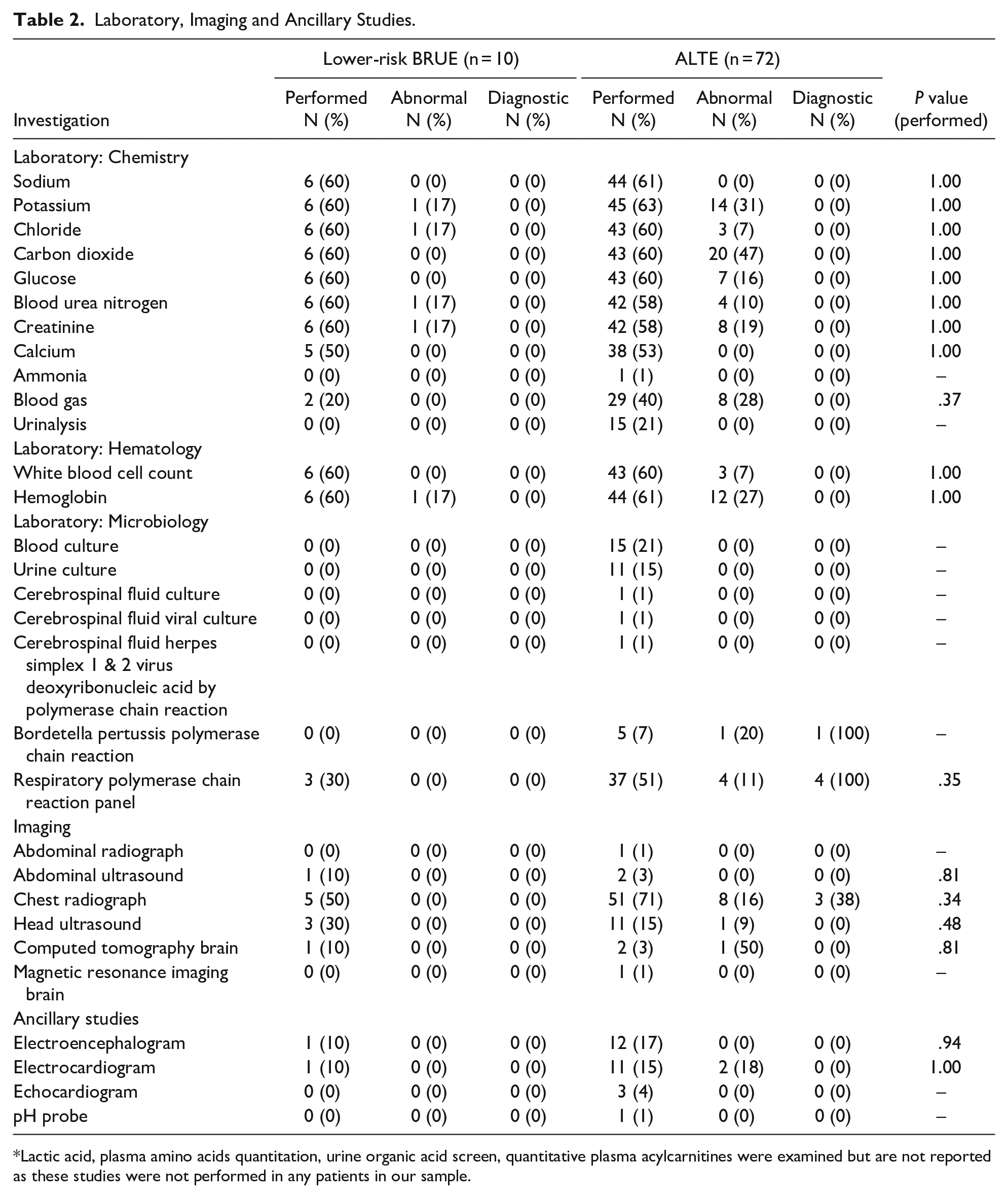
Lactic acid, plasma amino acids quantitation, urine organic acid screen, quantitative plasma acylcarnitines were examined but are not reported as these studies were not performed in any patients in our sample.
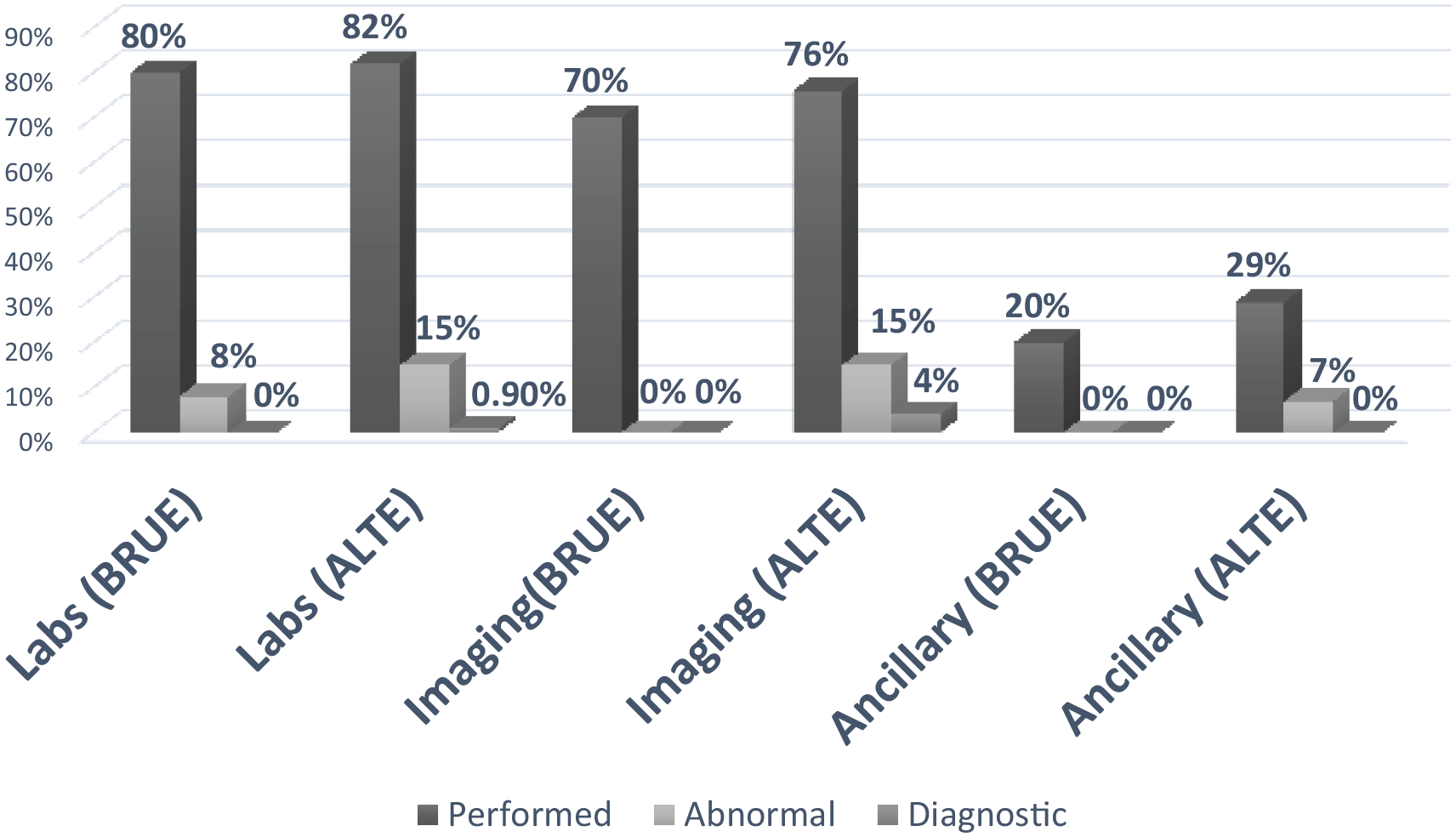
Diagnostic evaluation among patient with ALTE and BRUE.
Management and Follow Up
Most patients (BRUE: 6/10, 60%; ALTE 76/78, 97%) were admitted for cardiorespiratory monitoring. None of the patients in either group required critical interventions, including intubation, cardiopulmonary resuscitation, or ionotropic support. One patient with ALTE but none of the patients with a lower-risk BRUE had a recurrent event during hospitalization. One patient (10%) with a lower-risk BRUE and 8 patients with ALTE (11%) had a return visit to our institution within 90 days for reasons related to their index visit. The patient with a lower-risk BRUE saw a pediatric neurologist in a clinic setting and had an EEG performed that was negative. The patients with ALTE had a total of 17 return visits: 10 (59%) with a pediatric subspecialist in a clinic setting, 4 (24%) in the PED and 3 (18%) for outpatient diagnostic testing, including a skull radiograph, an esophagram and an upper gastrointestinal series. Final diagnoses for these 8 ALTE patients included gastroesophageal reflux (1; 13%), non-accidental trauma (1; 13%), seizure (1; 13%), laryngomalacia (1; 13%), plagiocephaly (1; 13%), breath holding spell (1; 13%), paroxysmal spell (1; 13%), and non-specific movements (1; 13%).
Discussion
Our study demonstrates that the published recommendations for the evaluation of patients with a lower-risk BRUE do not result in missed diagnostic opportunities. Inpatient admission is of little value for patients with a lower-risk BRUE, and no serious diagnoses were identified among these patients during follow up visits.
Unlike ALTE, the term BRUE specifies an age limit, characterizes the event, removes parental assessment of severity and requires that alternate explanations first be excluded by history and physical examination. 5 As a result, very few patients with ALTE meet the more precise definition for a BRUE. In our sample, most patients were not classified as BRUE due to an abnormal history, particularly reports of choking or gagging attributed to gastroesophageal reflux, abnormal vital signs and/or an abnormal physical examination. Overall, based upon our results and published studies to date, 493/2137 (23%) of patients with ALTE were classified as BRUE, with less than one-quarter of these patients classified as lower-risk (97/493; 20%).7,12,13 Thus, compared with ALTE, lower-risk BRUE is a relatively uncommon clinical entity, and is a diagnosis that relies upon a detailed history and physical examination. 5
The shift away from diagnostic testing for patients with a lower-risk BRUE differs markedly from the traditional approach to the evaluation of ALTE.2,3 ALTE has been associated with numerous conditions, including seizures, GERD, infections, and non-accidental trauma. 3 Therefore, evaluation was geared toward identifying a potential etiology for the event, resulting in a non-standardized approach to diagnostic testing. 2 In the absence of certain high risk features, however, such as age and prematurity, the yield of diagnostic testing is extremely low.2,3 Thus, the AAP indicates that clinicians should generally not perform diagnostic testing for patients with a lower-risk BRUE. 5 Unlike patients with ALTE, none of the patients with a lower-risk BRUE had positive diagnostic testing. Thus, our results are among the first to demonstrate that the published recommendations for the management of patients with a lower-risk BRUE do not result in missed diagnostic opportunities in the ED.
The AAP does suggest that an ECG and testing for pertussis may be considered for patients with a lower-risk BRUE. 5 Arrhythmias have been noted in up to 2% of patients with ALTE, 3 but none of the patients in our sample had an abnormal ECG. Prolonged QT was noted in one hospitalized patient with a higher-risk BRUE, but among patients with a lower-risk BRUE, arrhythmias appear to be uncommon.12,13 Pertussis is diagnosed in up to 7% of patients with ALTE, 3 and one patient with ALTE in our sample had pertussis. Conversely, none of the patients with a lower-risk BRUE in our study, or in the published literature, were diagnosed with pertussis.7,12,13 Although limited by a small sample size, both ECG and pertussis testing appear to be low yield; thus, current management recommendations for patients with a lower-risk BRUE should be prospectively evaluated.
Following diagnosis, the AAP indicates that clinicians may “briefly monitor patients with continuous pulse oximetry and serial observations” and “need not admit the patient to the hospital solely for cardiorespiratory monitoring”. 5 Our sample was derived prior to these recommendations, and 1/3 were transferred from an outside ED, yet none of the patients with a lower-risk BRUE had recurrent events or required critical interventions. Thus, our findings provide further support for the AAP recommendations for ED discharge home for patients with a lower-risk BRUE. 5 Although none of the patients with a lower-risk BRUE in our study were diagnosed with a serious condition, Colombo et al reported that one patient with a lower-risk BRUE was diagnosed with seizures upon outpatient follow up. 13 Thus, outpatient evaluation remains an important component of PED discharge for patients with a lower-risk BRUE. 5
Limitations
The results of this study are limited by its retrospective design. Event characterization may be inaccurate due to incomplete documentation, but all cases were reviewed by 2 authors prior to inclusion. Conservative application of the BRUE definition may have also resulted in an underestimation of the BRUE cases as patients with additional symptoms (e.g. choking) were not classified as a BRUE. Furthermore, the electronic query did not include codes for serious diagnoses associated with ALTE (e.g. non-accidental trauma). As a result, we may have overlooked potentially eligible patients and missed serious underlying diagnoses among patients with a lower-risk BRUE. We were also only able to obtain return visit information for our institution which provides a limited understanding of short term outcomes. Finally, this is a single center study with a small sample size which limits the ability to draw firm conclusions regarding patients with a lower-risk BRUE.
Conclusion
In conclusion, our results provide additional support for the AAP recommendation to discharge patients with a lower-risk BRUE home from the PED without performing an extensive diagnostic evaluation. Future prospective studies are needed, however, to evaluate the longer term clinical and economic impact of adherence to these recommendations.
Footnotes
Acknowledgements
The authors thank XX, MSBE, for assistance with data abstraction.
Author Contributions
AD: conceptualized and designed the study and obtained research funding.
RH and AD: designed the data collection instrument.
RH and SP: collected the data and managed quality control.
AD: supervised data collection.
AF: analyzed the data.
RH and AD: drafted the manuscript and all authors contributed substantially to its revision.
RH: takes responsibility for the paper as a whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.