
Abstract
Background. Congenital urethral obstruction occurs most frequently as a result of urethral valves. The diagnosis is usually confirmed pre- or neonatally. Though not ideal, delayed diagnosis can occur in childhood, adolescence, or adulthood. Despite a normal prenatal ultrasound, there may still be a delayed diagnosis of urethral valves. Methods. We present 4 patients with delayed diagnosis of posterior urethral valves (PUV) and 1 patient with delayed diagnosis of anterior urethral valves (AUV) who were evaluated by a pediatric urologist at our Institution. We determined the age and symptoms at presentation, physical examination, micturating cystourethrogram (MCU) findings prior to the valve ablation, renal function before and after valve ablation, type of valve ablation, and urine culture and sensitivity. The urological courses following urethral valve ablation including urodynamic study findings are described. Results. The median age at presentation was 33 months. All 5 patients presented with decreased urine output and urinary retention. All 5 patients underwent a MCU that demonstrated bladder trabeculations (3 cases), vesicoureteral reflux (3 cases), and bladder diverticula (2 cases). A urethral valve ablation was performed in all cases. Four patients underwent a renal function panel prior to this procedure, and their serum BUN/creatinine levels decreased 1 day postoperatively. Conclusion. Pediatricians should consider urethral valves as causing urethral obstruction although the prenatal ultrasound may be normal. Early diagnosis and prompt treatment of urethral valves may mitigate the potentially devastating morbidities such as renal failure, congestive heart failure, and respiratory distress that may ensue.
Highlights
Despite a normal prenatal ultrasound, there may still be a delayed diagnosis of urethral valves which may cause congenital urethral obstruction.
Our research determined the presenting symptoms, micturating cystourethrogram findings, and urological courses following urethral valve ablation in 4 patients with delayed diagnosis of posterior urethral valves and 1 patient with delayed diagnosis of anterior urethral valves who were evaluated by a pediatric urologist at our Institution.
Pediatricians should be aware that early diagnosis and prompt treatment of urethral valves may mitigate the potentially devastating morbidities such as renal failure, congestive heart failure, and respiratory distress that may ensue.
Introduction
Initially described by Young et al in 1919, 1 PUV are the most commonly encountered causes of lower urinary tract obstruction in male infants.2-10 PUV are commonly suspected on antenatal ultrasound but may present with a broad array of severity postnatally. Rarely, the diagnosis is missed until adolescence or adulthood when the patient presents with lower urinary tract symptoms. 11 This congenital abnormality of proximal urethral development is theorized to be due to Wolffian duct persistence or congenital obstructive posterior urethral membrane. 7 With an incidence of 1:5000 to 1:25 000 of live births,2-6,8,9 PUV may lead to renal failure in 25% to 43% of affected patients.8,11
First described by Watts in 1906, 12 AUV occur 15 to 30 times less frequently than PUV and are the most common congenital obstructive etiology affecting the male anterior urethra.13,14 They are posteriorly directed semilunar folds arising from the floor of the anterior urethra. AUV often have a low morbidity and mortality, however, several complications have been reported such as urinoma/hematoma, urethral strictures, and urethrocutaneous fistulae. 14
Delayed diagnosis of urethral valves has a worse prognosis compared to early diagnosis due to prolonged renal damage resulting in poor long-term outcomes. Early diagnosis of PUV is associated with severe bilateral vesicoureteral reflux (VUR) and bilateral hydroureteronephrosis, lesser grades and better resolution of VUR, and early relief of urinary obstruction following valve ablation. 15 Contrarily, children diagnosed later may have a higher risk of renal impairment, higher grades and bilateral VUR, and higher serum creatinine levels.15,16
We reviewed 4 patients with delayed PUV and 1 patient with delayed AUV who were evaluated at our Institution. Table 1 highlights the age and symptoms at presentation, physical examination, MCU findings before the valve ablation, renal function panel before and after the valve ablation, type of valve ablation, and urine culture and sensitivity. The diagnosis, treatment, and long-term management of delayed PUV and AUV are discussed.
Features of Patients With Delayed Posterior and Anterior Urethral Valves at Our Institution.
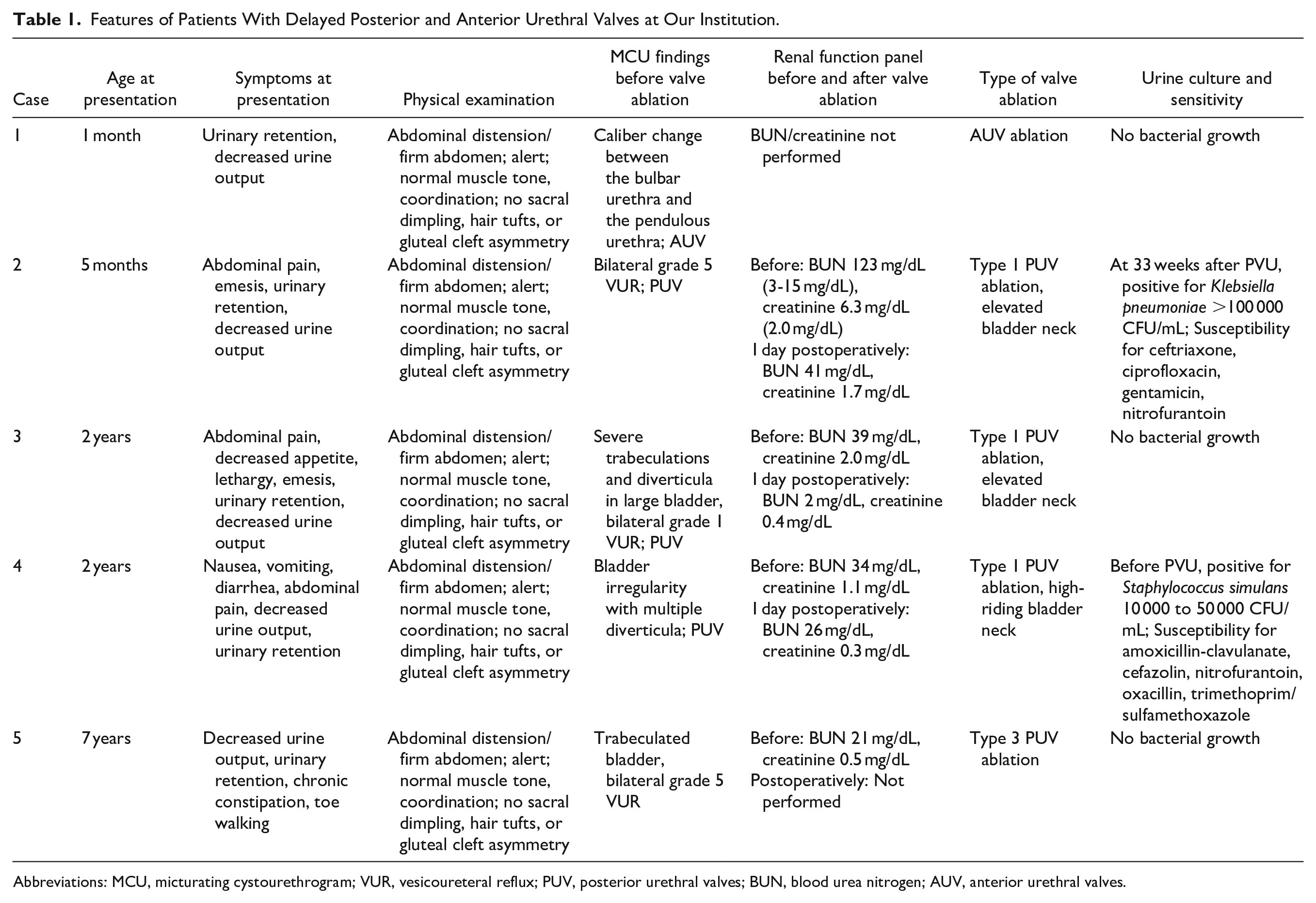
Abbreviations: MCU, micturating cystourethrogram; VUR, vesicoureteral reflux; PUV, posterior urethral valves; BUN, blood urea nitrogen; AUV, anterior urethral valves.
Ethical Approval and Informed Consent
The Chair/Vice-Chair of the University of Louisville Institutional Review Board (IRB Number 19.1050) determined that our study did not meet the “Common Rule” definition of human subjects’ research. Therefore, our study did not require IRB review. As the patients in this study were less than 10 years of age, the patients’ mother and/or guardian provided written consent.
Case Descriptions
Patients Less Than 2 years of Age
Case #1: The 1-month old male was born at term to a mother whose pregnancy was complicated by epilepsy, morbid obesity, and Herpes Simplex Type 2. The prenatal US showed bilateral renal dilatation with no evidence of urethral valves. A renal ultrasound (US) at birth and at 1 month of age demonstrated worsening bilateral hydronephrosis. A micturating cystourethrogram (MCU) at 3 days of age was initially read as normal by the radiologist but abnormal by the pediatric urologist upon referral at 1 month of age. The MCU reading was revised to reveal a caliber change between the bulbar urethra and the pendulous urethra concerning for possible AUV. The patient did not have a history of urinary tract infections. At 5 weeks of age, the patient underwent a cystoscopy with ablation of the AUV. A MCU 5 weeks after this procedure showed normal appearance of the anterior urethra with decreased trabeculation of the bladder wall. The patient had no evidence of a UTI or other urinary symptoms at 13 months of age. A renal US showed right-sided grade 1 hydronephrosis and left-sided grade 2 hydronephrosis. The last creatinine level was normal at 0.2 mg/dL. The patient has not undergone urodynamic studies (UDS).
Case #2: A 5-month-old male was born following an uncomplicated full-term pregnancy without evidence of hydronephrosis on prenatal US. The patient did not have a history of urinary tract infections. A MCU revealed evidence of severe bilateral hydroureteronephrosis and a markedly thickened and trabeculated urinary bladder (Figure 1). There was also grade 5 VUR bilaterally (Figure 2A) and findings consistent with PUV (Figure 2B). The patient underwent a cystoscopy with ablation of the Type 1 PUV using a Holmium laser fiber. A renal US performed 5 days after the procedure demonstrated continued severe bilateral hydronephrosis with significant bladder wall thickening. A MAG3 renal scan 2 months later showed a dilated bilateral renal collecting system with no upper urinary tract obstruction. The urine culture was positive for Klebsiella pneumoniae 33 weeks after the PUV ablation (Table 1). At the age of 22 months, the patient underwent a renal US that demonstrated bilateral high-grade hydroureteronephrosis with no masses or calculi. Due to this finding, the patient was treated with an indwelling catheter to drain urine overnight. His last creatinine level was normal.

A voiding cystourethrogram revealed evidence of a markedly thickened and trabeculated urinary bladder.
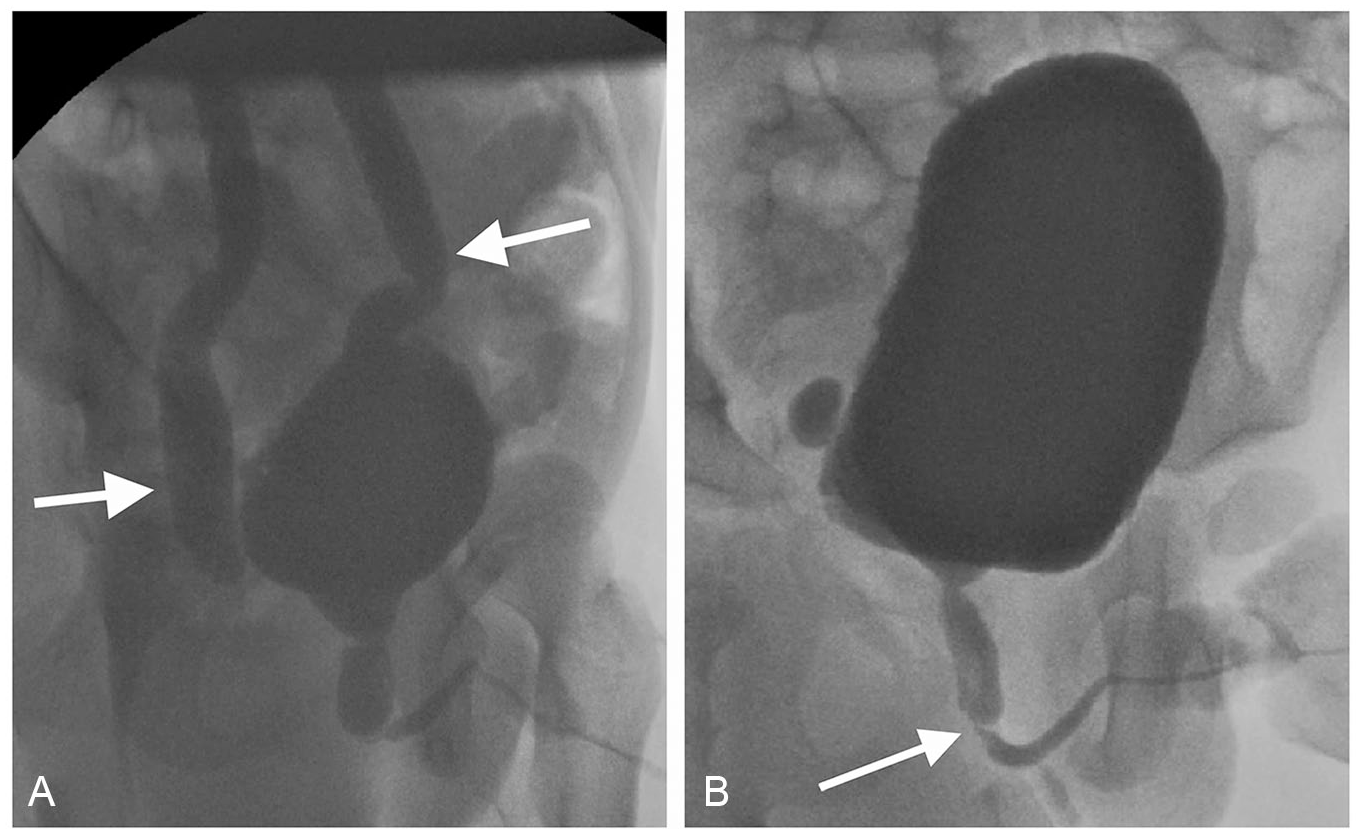
A voiding cystourethrogram demonstrated. (A) Grade 5 vesicoureteral reflux bilaterally (ureters indicated by arrows). (B) Findings consistent with a posterior urethral valve (arrow).
Patients Older Than 2 years of Age
Case #3: A 2-year-old male was born full-term by C-section. The infant experienced intrauterine growth retardation and respiratory distress and remained in the neonatal intensive care unit for 2 weeks after birth. There was no evidence of hydronephrosis or PUV by prenatal US. The pregnancy was complicated by chronic hypertension and Type II diabetes mellitus. The patient did not have a history of urinary tract infections. A MCU demonstrated an abrupt transition to normal anterior urethra, consistent with PUV. There was evidence of obstructive uropathy: a large bladder with severe trabeculations and diverticula as well as bilateral grade 1 VUR. A catheter was placed which drained 1 L of urine. The patient underwent a cystoscopy with ablation of the Type I PUV using a Holmium laser fiber. The patient was evaluated at 4 years of age at which time there was no evidence of chronic renal disease. His last creatinine level was normal. The patient has not undergone UDS.
Case #4: A 2-year-old male was born full-term, and the prenatal US was normal. A MCU was consistent with PUV and demonstrated bladder irregularity with multiple diverticula. The urine culture was positive for Staphylococcus simulans prior to the PUV ablation (Table 1). A cystoscopy was performed with ablation of the Type 1 PUV. A renal US 1 day after the cystoscopy showed continued bilateral hydronephrosis, a markedly thick-walled bladder wall, and a mild decrease in the hydronephrosis. At 3 years of age, a renal US demonstrated high-grade hydronephrosis bilaterally with dilated proximal and distal ureters and cortical thinning. His last creatinine level was normal.
Case #3: A 7-year-old male was adopted from China 5 years earlier and had experienced urinary incontinence and chronic constipation since his arrival in the United States. As the patient was adopted, there were no prenatal records. The patient underwent a lumbar MRI due to the concern for a tethered spinal cord. A lumbar MRI revealed severe bilateral hydronephrosis with no lesions around the distal spinal cord. A MCU showed bilateral grade 5 VUR and PUV with a trabeculated bladder outline. A MAG3 scan demonstrated bilateral hydronephrosis and no upper urinary tract obstruction. The patient did not have a history of urinary tract infections. A cystoscopy was performed for ablation of the Type 3 PUV. A renal US 2 weeks later showed persistent grade 4 bilateral hydronephrosis with right hydroureter. A renal US performed 8 months after the cystoscopy showed improvement in the bilateral hydronephrosis although the bladder remained trabeculated with significant postvoid residual (PVR). A renal US demonstrated improved urinary tract dilatation bilaterally. His last creatinine level was normal.
Urodynamic Studies
Three patients in this case series underwent UDS following the valve ablation. Cases #2 and #4 underwent 1 UDS, while Case #5 had 2 UDS. Table 2 depicts the bladder capacity, compliance, pelvic floor electromyography (EMG), detrusor overactivity, additional findings, and recommendations.
Urodynamic Studies at Our Institution.

Abbreviations: EMG, electromyography; VUR, vesicoureteral reflux; PVR, postvoid residual; PT, physical therapy.
Urodynamic study at 3 months after PUV: non-italics.
Urodynamic study at 22 months after PUV: italics.
Discussion
The presentation of urethral valves varies based on the degree of obstruction and age of the affected patient. AUV and PUV are usually diagnosed by prenatal US. 6 Infants and older children with delayed presentations of urethral valves may present with recurrent urinary tract infections, poor urinary stream, urinary frequency, nocturnal enuresis, urinary incontinence, anemia, and voiding pain or dysfunction.2,4-7,9,11,15,17 In Odetunde and colleagues’ study of 21 patients with late presentation of PUVs, the median age was 3 years (2 days-13 years), and the mean duration of symptoms before presentation was 2.6 years. 18 Nineteen (91%) patients presented with urosepsis, while 8 (36%) patients presented with significant renal insufficiency. The mechanism of late presentation may involve detrusor hypertrophy overcoming the congenital obstruction of the urethra. 3
A renal and bladder US is the most common initial imaging modality for both AUV and PUV and often reveals a thickened bladder wall, bilateral hydronephrosis, elevated PVR volume, as well as a dilated posterior urethra.2,6,9 A MCU confirms these findings and may also demonstrate bladder trabeculation, a circumferential filling defect at the level of the pelvic floor, prominence of the bladder neck, diverticula, and VUR.2,6,7,9 In Ozen and colleagues’ study of 17 boys diagnosed with late-presenting PUVs (mean age 7.35 years), PUVs were observed by voiding cystourethrogram (VCUG) in 10 (58.8%) patients, consisting of 9 with a dilated posterior urethra, 1 with posterior urethral irregularity, and 6 with a normal appearing urethra. Reflux was detected in 9 (52.9%) patients. 17 These authors recommend that cystoscopic examination is preferred to diagnose PUVs regardless of VCUG findings.
An endoscopic valve ablation is the postnatal treatment of choice for urethral valves to resolve the obstruction, preserve renal function, and achieve an appropriate urinary stream. While the goal of valve ablation is to eradicate the sequelae of urinary obstruction, persistence of VUR and voiding dysfunction after valve ablation denote a poor prognosis.13,16 Furthermore, lower urinary tract dysfunction is a common finding in boys after PUV ablation, regardless of their age at presentation.9,11 A repeat VCUG and cystoscopy may be needed in patients who continue to experience voiding difficulties or whose PVR did not decrease. Transurethral valve ablation may be performed for AUV in cases that are diagnosed early, however, there is an option for an open excision of the valve/diverticulum with urethroplasty when there is severe urethral dilatation and deformity. 14
Serum creatinine serves as a significant prognostic indicator in urethral valves.8,13 In their study of 120 patients with a mean age of 2 years with PUV, Sarhan and colleagues reported that the incidence of renal impairment with PUV was 22% when the initial serum creatinine was below 1 mg/dL which increased to 63% when it was above 1 mg/dL. 8 Additionally, the nadir serum creatinine following valve ablation was significantly lower in patients with normal final renal function. In Odetunde and colleagues’ study, the patients displayed a mild-to-marked elevation in serum creatinine prior to the PUV ablation. 18
Representing less than 5% of PUV, Type 3 PUV are exceedingly rare and are characterized by incomplete dissolution of the urogenital membrane leading to a diaphragmatic valvular obstruction. 6 This type is often associated with significant renal impairment. 19 Interestingly, the 7-year-old boy in our case series had evidence of Type 3 PUV.
UDS play a valuable role in testing the efficacy of treatment and determining whether any modifications in treatment may be necessary. 20 Features discerned during UDS may include structural anomalies (diverticuli, residual valves, strictures), VUR, functional problems (detrusor dyssynergia), and bladder emptying abnormalities. Ziylan and colleagues compared 36 males (mean age at diagnosis 8.8 years, range 5-14 years) with late presentation of PUVs to 19 age-matched controls with PUVs diagnosed and treated before 5 years of age. 21 Of the 20 patients who underwent urodynamic evaluation during follow-up, urodynamic bladder abnormalities were detected in 17 (85%) patients, detrusor overactivity in 3 (15%), significant post-void residual in 9 (45%), and bladder capacity greater than expected for age in 9 (45%). Detrusor overactivity was significantly lower in the late presenting group (P = .013), and renal function was significantly impaired in the late presenting group compared to controls (P = .001). In Kajbafzadeh and colleagues’ study of 8 patients who underwent AUV ablation, the major urodynamic dysfunction was bladder hypercontractivity that resolved following valve ablation. 22 None of the patients in their study had low-compliant bladder, detrusor instability, or myogenic failure. Three of the 5 patients in our case series underwent UDS following the PUV ablation, all of whom had an increased pelvic floor EMG and low bladder compliance. Detrusor overactivity was observed in 2 cases, bladder capacity greater than that expected for age in 2 cases, and VUR in 1 case. A host of recommendations were suggested, including oxybutynin, clean intermittent catheterization, PT with pelvic floor retraining, voiding schedule, and to keep a voiding diary with PVRs. Our study confirms the importance of long-term monitoring of patients with delayed urethral valves for urinary abnormalities.
Our case series reflects 4 patients ages 5 months to 7 years with delayed diagnosis of PUV and a 1-month-old infant with delayed diagnosis of AUV. The importance of the present study is that the patients underwent a prenatal ultrasound without evidence of oligohydramnios, hydronephrosis, PUV, or AUV. However, it was possible to see bilateral hydroureteronephrosis and thickened bladder wall for all patients on postnatal ultrasound at which time they were diagnosed with PUV or AUV. This is surprising since the prenatal US were normal. Our study adds to the small but growing body of literature highlighting delayed PUV and AUV presentation and emphasizes the value of a high degree of clinical suspicion when evaluating boys of any age with lower urinary tract symptoms and atypical urologic complaints.
All 5 patients in our case series presented with decreased urine output and urinary retention. Pediatricians should be aware that urethral valves can have a delayed presentation despite a normal prenatal US. Abdominal pain, nausea, and urinary retention may suggest the clinical presentation of urethral obstruction caused by urethral valves. In order to rule out a delayed diagnosis of urethral valves, a pediatric urologic consultation should be scheduled promptly, and a MCU should be performed. Besides the presence of the urethral valve, a few other classic findings were demonstrated on the MCU prior to the PUV valve ablation in our study, including bladder trabeculations (3 cases), diverticula (2 cases), and VUR (bilateral grade 1 in 1 case; bilateral grade 5 in 2 cases). The serum creatinine level of 3 patients diagnosed with delayed PUV decreased following the PUV ablation. An elevated bladder neck was observed during PUV ablation in 3 patients. The improved BUN and creatinine in such a short period of time after PUV ablation may be attributed to catheter placement for bladder drainage several days prior to the ablation. Patients may experience underdevelopment of the lungs due to oligohydramnios. After the patient was stable from a respiratory standpoint, the valve ablation was performed. The ultrasound and MAG3 scans were performed shortly after valve ablation as these tests were requested by the nephrology team treating the patients.
Limitations of this case series include its retrospective nature and small number of cases. As both delayed posterior and anterior urethral valves are exceedingly rare conditions, the size of our case series is larger than others reported in the literature which are primarily single case reports. Further investigation will include a larger number of patients with a longer follow-up. Another limitation is that only 3 of 5 patients underwent urodynamic studies.
Conclusion
A high index of suspicion is warranted in cases of delayed presentation of urethral valves despite a history of a normal prenatal US. Delayed diagnosis of urethral valves often has overlapping features with other diseases. Pediatricians should consider delayed urethral valves in the differential diagnosis when an infant or child presents with symptoms of recurrent urinary tract infections and voiding difficulties such as poor urinary stream, urgency, and incontinence. Diligent long-term surveillance with MCU, serial renal sonograms, and routine serum creatinine following valve ablation is necessary to ensure proper renal and bladder function.
Footnotes
Acknowledgements
We acknowledge Norton Healthcare for their continued support.
Author Contributions
LBES made substantial contributions to the conception and design, analyzed and interpreted the data, performed the literature search, and was the major contributor in the writing of the manuscript. JTW, AZM, DSP, and ER made substantial contributions to the conception and design, analyzed and interpreted the data, and revised the draft critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
As the patients in this study were less than 10 years of age, the patients’ mother and/or guardian provided written consent.