
Abstract
Diabetic ketoacidosis (DKA) is an important diagnosis in the pediatric intensive care unit (PICU) and is associated with significant morbidity. We hypothesized children with DKA living in poorer communities would have unfavorable outcomes while critically ill. This single-center retrospective study included children with DKA admitted to a PICU over a 27-month period. Patients were classified as low-income if they lived in a ZIP code where the median household income was estimated to be less than 200% of the federal poverty threshold, or $48 016 for a family of 4. In this study, living in a low-income ZIP code was not associated with increased severity of illness, longer PICU length of stay (LOS), or readmission.
There are well established associations between adverse health outcomes and poverty in children, but little is specifically known about the effects of poverty on pediatric critical illness.
To our knowledge, this is the first study to specifically address associations between estimated income level and PICU outcomes in children admitted with DKA, an important condition in the PICU.
Acute care physicians must understand the social challenges faced by low income families, recognize the toll a critical care admission likely places on a deprived family, and begin to address them upon hospital admission through social work referrals, partnerships with community resources, and robust communication with primary care providers.
Background
Type I diabetes (T1D) is a substantial public health burden, and the incidence is increasing worldwide.1-3 In the United States, there are approximately 21.7 new diagnoses of T1D per 100 000 children each year. 4 Diabetic ketoacidosis (DKA) is a common and expensive complication of T1D, with each DKA-related admission costing an estimated $7000. 5 There is evidence suggesting community-level, hospital-level, and patient-level variability exists in healthcare utilization among children hospitalized with DKA, likely in part due to variability in risk factors.5-7 Because of the high social burden of DKA, identifying potentially modifiable factors may lead to improved patient outcomes and decreased healthcare resource utilization.
Poor glycemic control, psychiatric disorders, younger age, and low socioeconomic status have been associated with increased risk of developing DKA, but little is known if these risk factors influence patient outcomes while in the pediatric intensive care unit (PICU).8-11 Because many hospitalized children with DKA require PICU admission, understanding how modifiable patient risk factors influence short-term outcomes may ultimately decrease hospital utilization.12,13
Approximately half of all children living in the United States live in low-income households. 14 It is known that socioeconomic factors are associated with poor glycemic control and higher incidence of DKA, but it is unclear if a patient’s socioeconomic status influences short-term outcomes in the PICU. Therefore, this study aimed to describe the association between estimated household income and clinical outcomes of children admitted to the PICU for DKA. We hypothesized that children living in low-income communities would have unfavorable consequences, including a longer length of stay (LOS).
Methods
This was a retrospective study of children admitted to one mixed medical-surgical PICU in a tertiary academic medical center. With institutional review board approval, children <19 years of age with a primary diagnosis of DKA admitted between October 1, 2013 and December 31, 2015 were identified using local Virtual PICU (Virtual PICU Systems, Los Angeles, CA) data. Only the first admission during the study period was included in our analyses. The database was queried for demographics, PICU LOS, and laboratory values at admission. Additional demographics, PICU readmissions during the study period, diagnostic studies and administered therapeutics including duration of insulin infusion were obtained from the electronic medical record. DKA severity was categorized based on the serum pH at admission: children with admission pH of 7.2 to 7.3 were classified as mild, those with pH between 7.1 and 7.19 were classified as moderate, and children with admission pH <7.1 were classified as having severe DKA. 15 This severity classification system is consistent with previously published consensus statements on DKA in the pediatric population. 15 At our center, children with DKA with admission serum pH <7.3 and/or bicarbonate ≤15 mmol/L are admitted to PICU; those with serum pH >7.3 and bicarbonate >15 mmol/L may be admitted to a regular inpatient hospital unit. All children who require excessive fluid administration prior to admission, have mental status changes, or have serum glucose levels >800 mg/dL require PICU admission, regardless of admission serum pH and bicarbonate values. Children with DKA requiring hospitalization at our institution are managed with an insulin, fluid and laboratory schedule protocol that begins at emergency department presentation. All children with DKA are admitted to the PICU, where the protocolized care is continued. This protocol was in place during the entire duration of the study period.
Collected demographics included age, race, gender, and residential ZIP code. Median household income for each patient was estimated by matching ZIP code to publicly available 2014 US Census Bureau data. In 2014, the federal poverty threshold (FPT) for a family of 4 was $24 008. 16 In this study, we designated children living in a ZIP code with a median household income less than the FPT as “poor,” and those with an income less than 200% of the FPT as “low-income.”
The primary outcome measure was PICU LOS. Other outcome measures included duration of insulin infusion, severity of illness, and readmission risk. We defined morbidity as requiring central venous line placement (indicating a severe course of illness), requiring computed tomography (CT) of the brain due to clinical concerns for cerebral edema, and/or having documented episodes of cardiac arrhythmias. Analyses were conducted using SigmaPlot 12.5 (Systat Software, Inc, San Jose, CA). Descriptive statistics were used to interpret demographic data and presented as proportions. Continuous data are presented as median values and interquartile ranges. Categorical data are presented as numbers and percentages. The chi square test was used to compare the severity of DKA and readmission risk between children who were and were not low-income. The Mann-Whitney U test was used to compare LOS. A 2-sided P value of <.05 was considered statistically significant.
Ethical Approval and Informed Consent
This study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board (UHCMC IRB number 04-16-05) with a waiver of informed consent. Waiver of informed consent was granted as this research involved medical records that were collected solely for non-research purposes, and that the rights and welfare of included subjects were not at enough risk to require informed consent.
Results
During the 27-month study period, 171 patients were admitted to the PICU with a primary diagnosis of DKA. These patients accounted for 5.3% of the 3242 children requiring PICU admission during the study period. Patient demographics are shown in Table 1. Most patients were Caucasian (64%), with a median age of 13.3 [10.2-15.2] years. Nearly one-half (n = 80) of children were living in a low-income neighborhood.
Demographics of Children Admitted to One PICU with DKA.
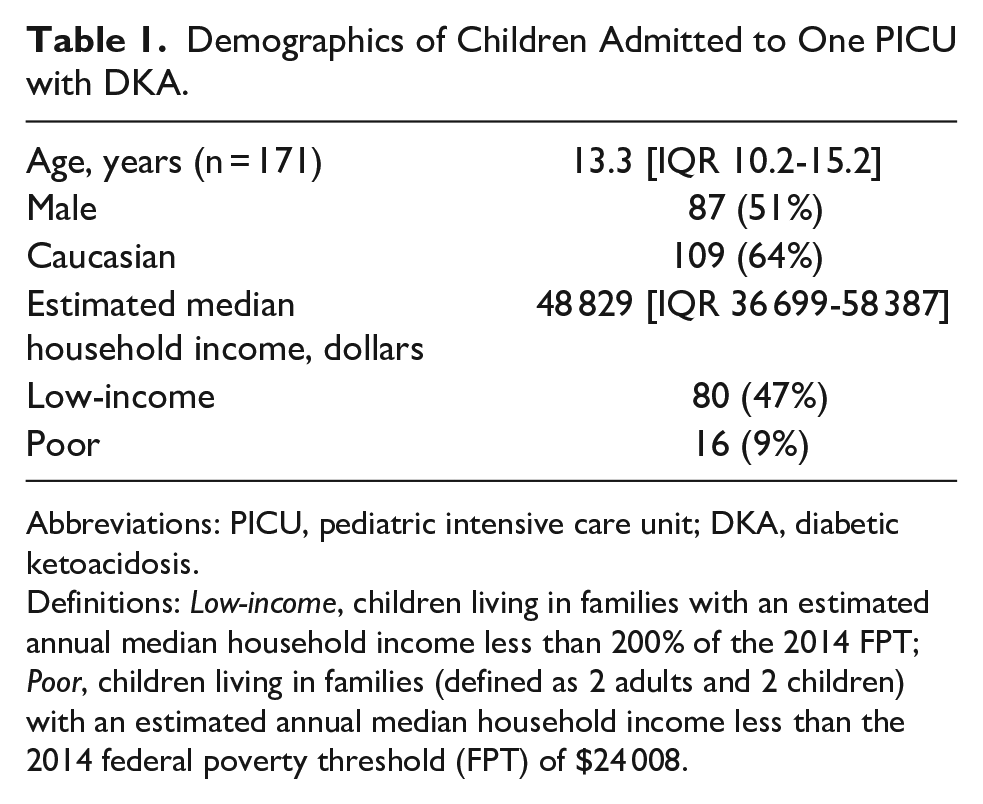
Abbreviations: PICU, pediatric intensive care unit; DKA, diabetic ketoacidosis.
Definitions: Low-income, children living in families with an estimated annual median household income less than 200% of the 2014 FPT; Poor, children living in families (defined as 2 adults and 2 children) with an estimated annual median household income less than the 2014 federal poverty threshold (FPT) of $24 008.
Most children met criteria for mild DKA at the time of PICU admission (Table 2). There were no deaths, and morbidity was low (Table 3). Only 3 (1.8%) children required central venous access, 2 (1.2%) underwent computed tomography of the head, and none had documented episodes of cardiac arrhythmias. The median PICU and hospital LOS were 0.9 days [0.7-1.1] and 2.6 days [1.8-3.17], respectively. Children admitted with severe DKA had a longer PICU LOS (1.2 days [0.97-1.73] vs 0.83 [0.67-0.99], P < .001) than those admitted in mild or moderate DKA.
Clinical Characteristics on PICU Admission.
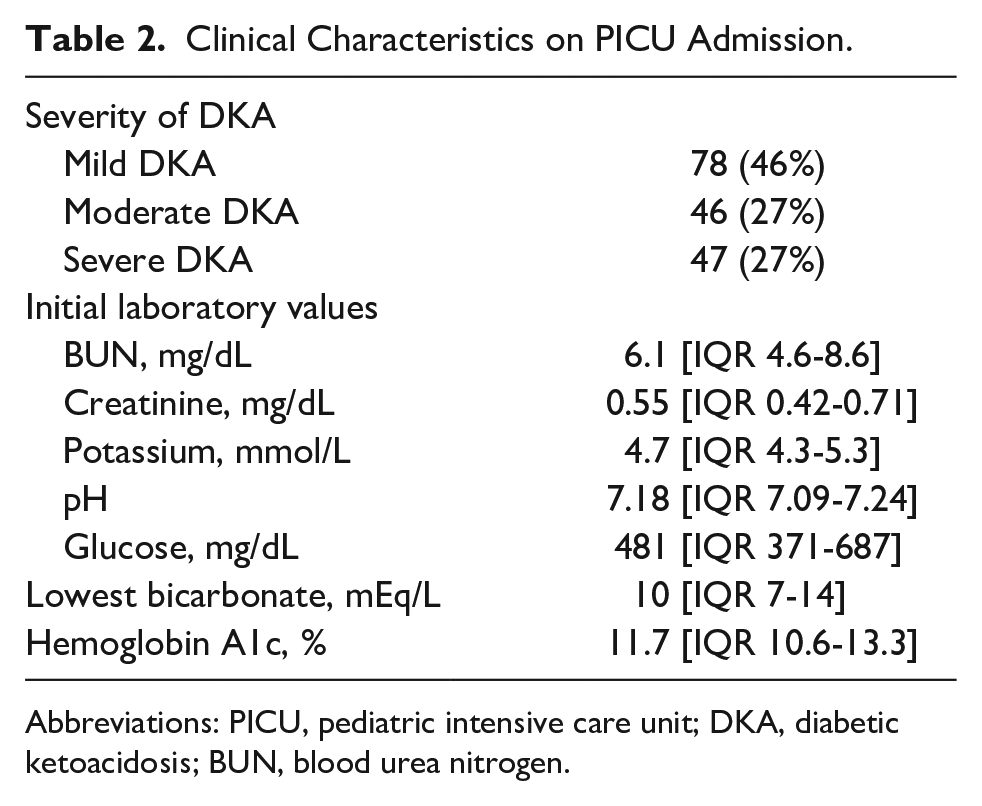
Abbreviations: PICU, pediatric intensive care unit; DKA, diabetic ketoacidosis; BUN, blood urea nitrogen.
PICU Outcomes of Study Cohort (n = 171).

Abbreviations: PICU, pediatric intensive care unit; LOS, length of stay; CT, computed tomography.
Outcomes were similar regardless of estimated patient income (Table 4). There were no differences in the number of patients with mild, moderate, or severe DKA (P = .867), initial pH, glucose, lactate, or potassium values between patients who were and were not low-income. Resolution of DKA followed a similar clinical course regardless of estimated household income. The duration of insulin infusion and PICU LOS were similar between those children living below and above 200% of the FPT.
Comparison of Clinical Characteristics.
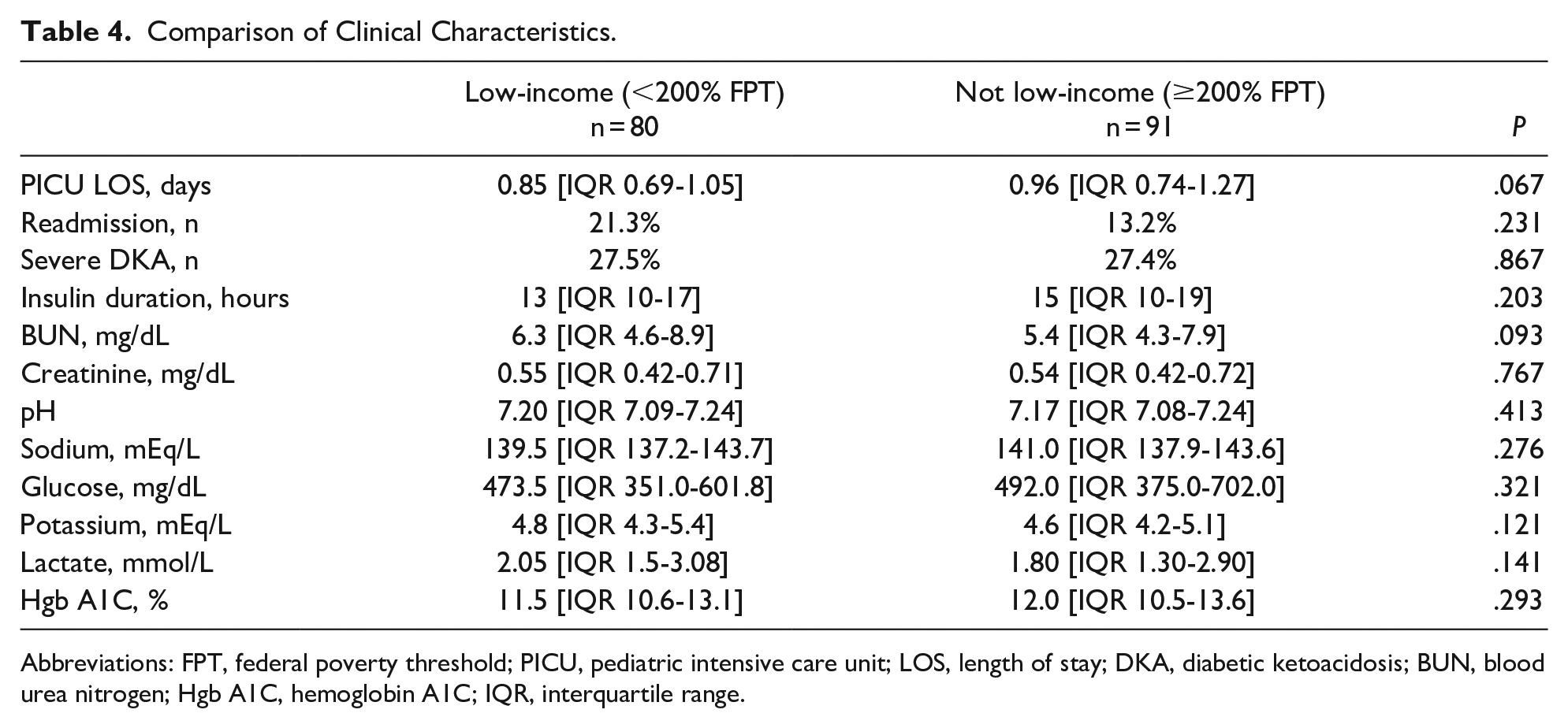
Abbreviations: FPT, federal poverty threshold; PICU, pediatric intensive care unit; LOS, length of stay; DKA, diabetic ketoacidosis; BUN, blood urea nitrogen; Hgb A1C, hemoglobin A1C; IQR, interquartile range.
Of the 171 included patients, 29 (17%) were readmitted to the PICU for DKA during the study period. There was no difference in readmission rate between patients from the poorer communities versus those living in neighborhoods with higher median household income. Additionally, both groups had similar glycemic control, based on hemoglobin A1c at admission.
Discussion
The socioeconomic status of children with T1D has generally been described as affluent, with a higher incidence of T1D among children from higher income communities.17,18 While children in living in affluent ZIP codes are at increased risk for developing T1D, low-income, low parental educational attainment, and public insurance are associated with development of DKA, a preventable complication of T1D.9,11,19 To our knowledge, this is the first study to explore associations between estimated household income and PICU outcomes for children with DKA. Nearly half of the children included in this cohort were living in low-income families, a proportion that mirrors the percentage of low-income children nationally. 14 We found no differences in outcomes including LOS or readmission rate between children who were and were not living in low-income households. This was an unexpected finding, considering multiple previous studies with similar patient populations showed an association between lower socioeconomic status and unfavorable hospital outcomes.7,11,20
In a multicenter retrospective cohort study using the publicly available National Inpatient Sample database, Keenan et al described an association between poverty (estimated from ZIP code) and a hospital stay ≥ 7 days in children with DKA. 7 This study did not differentiate between the PICU and total hospital stay, but a more recent multicenter study including data from 38 children’s hospitals found that the non-PICU portion of the hospitalization was the predominant driver of hospital resource use variability. 5 In our own study there was little variability in the PICU LOS, with the duration ranging from 0.1 to 3.2 days in this cohort of 171 children. DKA treatment is protocolized in many institutions, including ours. This has led to improved outcomes including shorter length of stay.21,22 Our hospital employs a standardized intravenous fluid, medication and laboratory schedule order set for patients admitted to the PICU with DKA. There is little variability in treatment of these patients in our facility, which may account for the similar LOS and duration of insulin observed in this study. Additionally, patients living above and below the 200% of the FPT in this cohort presented with similar DKA severity and metabolic derangements at time of admission, which likely contributes to the similarity of outcomes between the 2 groups.
In adult diabetic patients, low-income is associated with an increased risk of extremity amputations, coronary artery disease, and renal disease, suggesting poorer glycemic control.23,24 In our study, there was no difference in hemoglobin A1c at admission between patients from lower income and higher income communities. The median hemoglobin A1c of 11.7% suggests poor glycemic control in both study groups, consistent with previous literature showing an association between DKA and elevated hemoglobin A1c. 25 Identifying patients from socially fragile families upon PICU admission is important, despite there not being a difference in DKA severity, metabolic derangements or outcomes between different income groups in this study. In the outpatient setting, an association between low socioeconomic status and poor glycemic control has been described in pediatric patients. 11 Diabetic management requires frequent glucose monitoring and insulin dosing. Insulin is an expensive medication and not always accessible to poor families, and social disadvantage contributes to missed appointments necessary for optimal management of a chronic medical condition.26,27 Acute care physicians must understand these challenges, recognize the toll a critical care admission likely places on a deprived family, and begin to address them upon hospital admission through social work referrals, partnerships with community resources, and robust communication with primary care providers. 28
There are limitations to this study. Inclusion of children from only 1 institution serving a large underserved population, the modest sample size, and retrospective design limits generalizability. There are 2 other PICUs in our city, and although our demographics are comparable to national percentages, this may skew our results, as children from higher income homes may prefer 1 hospital over the others. Based on initial pH, only 27% of children in this cohort presented in severe DKA. The relative lack of illness severity may falsely shorten the PICU LOS and skew results in this study. The use of ZIP code as a proxy for socioeconomic status can be problematic as a ZIP code may be assigned to an area with income heterogeneity, potentially leading to incorrect inferences of familial income of individual study subjects. 29 Future retrospective studies could use census tract data, which are more homogenous communities with respect to the economic status and population characteristics of its inhabitants. 30 An accurate understanding of the social conditions of each PICU family will ultimately require a prospective, interview study design.
Conclusion
To our knowledge, this is the first study to specifically investigate differences in illness severity, treatment requirements and LOS based on estimated family household income level in children admitted to the PICU with DKA. We hypothesize that our center’s consistent use of a standardized DKA management protocol contributed to similarities in observed outcomes. Although there were no differences in hospital outcomes between income groups in this single center study, understanding the socioeconomic stressors that families of critically ill children face remains imperative for hospital-based physicians. T1D is a chronic disease requiring careful outpatient management, which may be particularly challenging for low-income families. A systematic process to transition children with DKA from the acute to outpatient care setting is necessary for optimal disease control, and this process should begin at admission to the PICU. Adherence to standardized, evidence-based management protocols for children requiring PICU admission for DKA—as well as other critical disease processes—may be helpful in mitigating differences in hospital outcomes that may result from socioeconomic disparities.
Footnotes
Author Contributions
Broberg and Slain conceputualized and designed the study, and contributed to the acquisition, analysis and interpretation of the data. Broberg drafted the manuscript. Broberg, Rose and Slain critically revised and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.