
Abstract
Over a decade after its debut, human papillomavirus (HPV) vaccine coverage remains suboptimal. The inpatient setting presents a largely unexplored opportunity to increase vaccination rates. This study aims to describe pediatric resident attitudes toward inpatient immunization and compare differences by vaccine, in particular HPV. An anonymous survey of beliefs and practices regarding inpatient vaccines was distributed to pediatric resident physicians at a single freestanding urban children’s hospital in September 2017. A total of 58 surveys were collected (64% response rate). We found that pediatric residents were more likely to report that they never or rarely discuss the HPV vaccine during hospitalization compared with the primary childhood series (P = .001), Tdap (P = .02), and the influenza vaccine (P < .001), and rarely offer the HPV vaccine during hospitalization compared with childhood vaccines (P = .003) and influenza (P = .001). This suggests that provider hesitancy still exists for the HPV vaccine, presenting opportunities for further education and inpatient interventions.
Introduction
The American Academy of Pediatrics recommends using every health care visit as an opportunity to review and update vaccine status, especially in adolescents.1-3 This practice, known as opportunistic immunization, is advocated for in the United States and internationally to help increase vaccine uptake.4,5 While literature exists about opportunistic immunization in pediatric and adult populations for both the primary series and influenza vaccines, studies evaluating the human papillomavirus (HPV) vaccine in the inpatient setting are limited. Immunization rates for HPV are lower than any other Advisory Committee on Immunization Practices (ACIP) recommended vaccine, excluding the influenza vaccine, which continues to have the lowest rates. The HPV vaccine was first recommended for females only in 2006, with guidance later expanding to include routine immunization of males in 2011. 6 However, despite a decade of data on the safety and efficacy of the HPV vaccine, immunization rates remain low in both males and females. The 2017 National Immunization Survey Teen found that although rates of HPV vaccination have been rising, only 68.6% of females and 62.6% of males aged 13 to17 years had received at least one dose of the vaccine. Meanwhile, only 48.6% of adolescents aged 13 to 17 years have completed the HPV vaccine series. 7
Previous studies have identified significant gaps in immunization status for hospitalized patients. A study at a tertiary children’s hospital in England showed that 20.5% of inpatients were either due or past due for an immunization while hospitalized. 8 A children’s hospital in the United States found that 27% of hospitalized children were behind on vaccines; HPV was the most common vaccine needed, and adolescents were the group least likely to be up to date. 9 Other studies have also confirmed this disproportionate impact on teens, finding that 94% of adolescents required catch-up vaccines at the time of hospital admission. 10 Unfortunately, these studies also highlighted the difficulty in obtaining accurate vaccine records in the inpatient setting. In a recent retrospective cohort study looking at hospitalized children with a respiratory illness, 94% of charts had “up to date” on vaccines documented by the physician while in reality, only 42% of these patients were truly “up to date” when compared with the public vaccine records. 11
The inpatient encounter is a promising opportunity to augment the low rates of HPV vaccination, especially given adolescents’ infrequent visits to primary care providers.12,13
A systematic review identified provider attitudes toward HPV vaccine as key drivers for vaccine uptake in the outpatient setting. 14 Provider hesitancy regarding the HPV vaccine has been well documented in outpatient practice, where pediatric health care providers have noted that they prefer to offer the vaccine as optional or avoid discussing the vaccine due to anticipation of parental refusal. 15 This is the first study to date examining whether these same attitudes apply in the inpatient setting, and how they may affect provider behaviors.
Methods
An anonymous survey regarding provider attitudes and practices surrounding administration of vaccines during hospital admission was distributed to first-, second-, and third-year pediatric residents at an urban tertiary care children’s hospital (Supplementary Figure 1; available online). Demographic questions included level of training (postgraduate years [PGY] 1 through 3) and gender. Four vaccine-related questions were asked regarding whether residents had discussed a vaccine type when admitting a patient to the hospital, offered a vaccine type when admitting a patient to the hospital, believed a vaccine type should be offered in the hospital, and believed a vaccine type should only be offered in the outpatient setting by the primary care provider, each with a 4-point Likert-type scale. Vaccine types included the following: primary childhood vaccine series (diphtheria, tetanus, and acellular pertussis [DTaP], Haemophilus influenzae type B, hepatitis B, pneumococcal conjugate, inactivated poliovirus, measles, mumps, and rubella, varicella, and hepatitis A vaccines); tetanus, diphtheria, and acellular pertussis (Tdap); meningococcal; HPV; and influenza vaccines. A free-text section for additional comments was also included in the survey.
Surveys were administered on paper during a residency-wide educational conference, as well as via a web-based survey tool (www.qualtrics.com) disseminated by email for residents not present at the educational conference. Residents were asked in the email to complete the survey only one time.
Contingency tables were constructed to evaluate agreement between opinions for each vaccine type within each question. The 4-point scales were combined to create a dichotomous outcome. Chi-square tests and binary logistic regressions were conducted to examine overall differences in discussion and offering of HPV vaccination compared with the other vaccines. Differences in responses by resident gender and level of training were also examined using χ2 tests and binary logistic regression.
Ethical Approval and Informed Consent
The study was determined to be exempt by the Children’s Hospital Los Angeles Institutional Review Board, Study ID: CHLA-17-00287. Participants were provided with a study information sheet prior to completing the survey but no written consent was required. Participants were not reimbursed for participation.
Results
A total of 58 surveys were collected (64% response rate), with similar numbers of residents from each level of training. Of the respondents, 46 were female (79%) and 11 were male (19%); 1 declined to state gender (Table 1). The demographics were similar between respondents and nonrespondents. For all vaccine types queried, most residents reported that they sometimes or usually discussed vaccines at the time of admission. However, fewer report having offered vaccines during admission, particularly for adolescent vaccines; more than 70% of residents responded that they never or rarely offer the adolescent vaccines, including the HPV vaccine, during hospital stay (Table 2). The vast majority of residents agreed or strongly agreed that patients should be offered all types of vaccines in the hospital, and few believe they should only be offered by the primary care physician as outpatient; this did not vary by vaccine type (Table 2).
Demographics of Survey Respondents.

Abbreviation: PGY, postgraduate year level.
Total number of respondents was 58 (64%).
Resident Survey Responses by Vaccine Type (n = 58).

Abbreviations: PCP, pharmacist-provided vaccination; Tdap, tetanus, diphtheria, and acellular pertussis; HPV, human papillomavirus.
Out of 57 responses for this item.
Out of 56 responses for this item.
Comparisons were made between the HPV vaccine and other childhood vaccines overall. Residents were much less likely to report discussing the HPV vaccine during inpatient admission, when compared with primary childhood vaccines (odds ratio [OR] = 6.02, 95% confidence interval [CI] = 2.08-17.40), Tdap (OR = 2.72, 95% CI = 1.15-6.48), and influenza (OR = 10.03, 95% CI = 2.79-36.08; Table 3 and Figure 1). Residents were also much less likely to report offering HPV vaccine compared with childhood series (OR = 3.18, 95% CI = 1.48-6.86) and influenza (OR = 3.57, 95% CI = 1.64-7.73). There was no significant difference between offering HPV and the other adolescent vaccines. In addition, there were no significant differences between HPV and other vaccines in the proportion of residents reporting that vaccines should be offered when a patient is admitted to the hospital, or should only be given as an outpatient (Table 3).
Resident Attitudes Toward Inpatient Vaccines, Compared With HPV Vaccine.

Abbreviations: HPV, human papillomavirus; OR, odds ratio; CI, confidence interval; Tdap, tetanus, diphtheria, and acellular pertussis.

Odds ratio for discussing and offering vaccines at admission, compared with human papillomavirus (HPV) vaccine.
Next, differences in responses for each vaccine type were compared by provider gender. Male residents were less likely to discuss the meningococcal vaccine (OR = 0.19, 95% CI = 0.04-0.79) when compared with their female counterparts. There were no statistically significant differences between male and female providers in offering any of the vaccines. No differences were found when comparing the level of training of residents and discussion or offering of vaccines (Table 4).
Resident-Reported Discussion and Offering of Vaccines During Admission, by Gender and Level of Training.
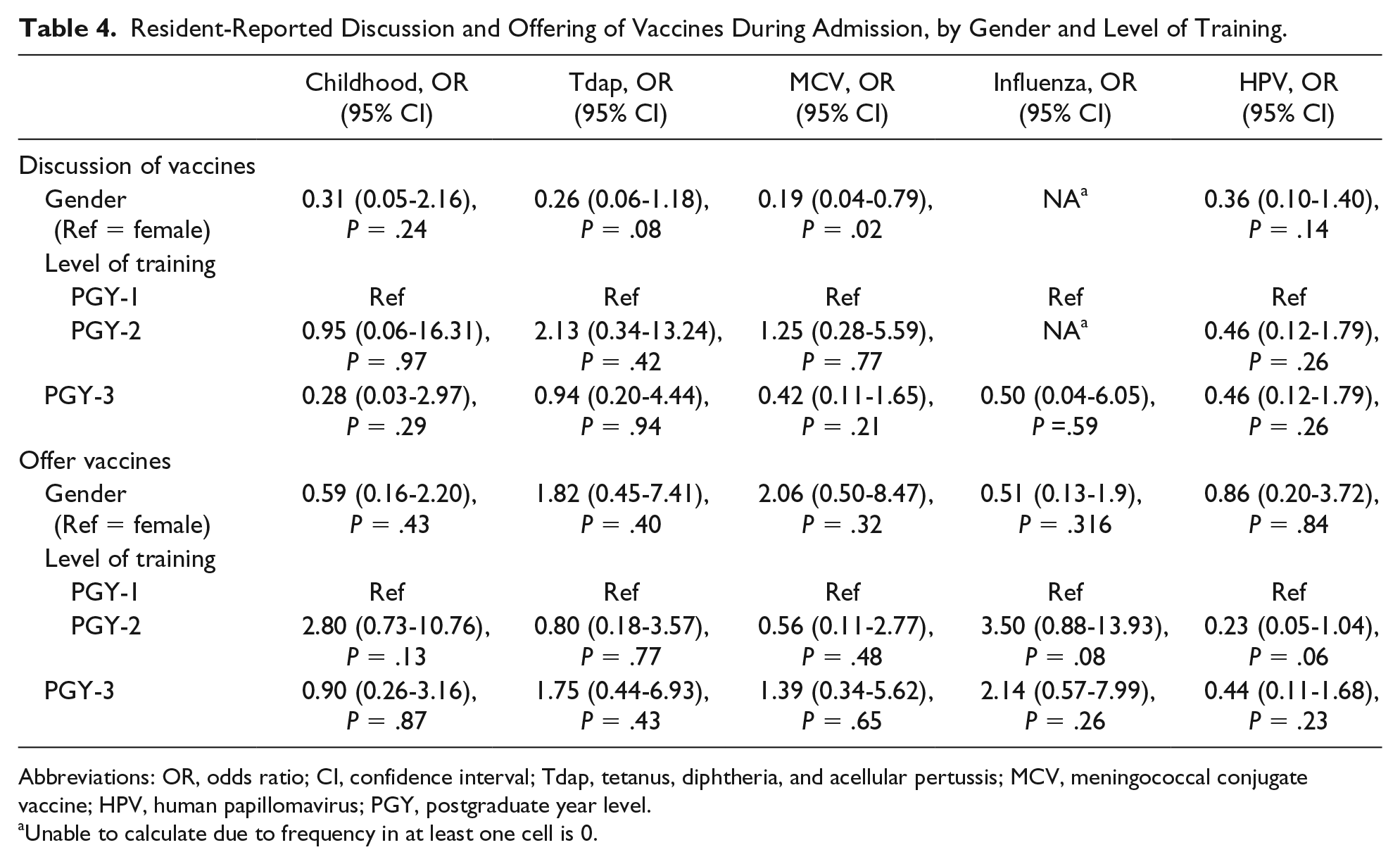
Abbreviations: OR, odds ratio; CI, confidence interval; Tdap, tetanus, diphtheria, and acellular pertussis; MCV, meningococcal conjugate vaccine; HPV, human papillomavirus; PGY, postgraduate year level.
Unable to calculate due to frequency in at least one cell is 0.
Discussion
This study evaluates the opinions and self-reported practices of pediatric residents regarding inpatient administration of vaccines, including the HPV vaccine. While both the American Academy of Pediatrics and the ACIP recommend using every health care visit as an opportunity to review and update vaccine status, 2 our study found that providers are less likely to discuss and offer the HPV vaccine in the hospital setting compared with other vaccines.
Pediatric resident physicians were chosen as the survey population, because in our hospital, and in the majority of large academic children’s hospitals, residents are often a patient’s primary provider, from placing orders to serving as the primary point of contact for counseling to answering any questions patients or their families may have. In the residency program at our hospital, residents are expected to obtain a vaccination history for every patient admitted to the hospital. Pediatric residents have also served as a primary stakeholder group in prior studies evaluating increased inpatient delivery of the childhood and influenza vaccines.16,17
Our survey demonstrated that despite most residents reporting they believe that all vaccines should be offered in the inpatient setting, the HPV vaccine was not routinely discussed or offered during hospitalization, was discussed less than the primary childhood vaccine series, Tdap, and the influenza vaccine, and was offered less than the primary series and influenza vaccines. These findings are consistent with aforementioned studies of outpatient primary care providers, indicating that despite agreement on the theoretical importance of HPV vaccination, there is a lack of emphasis on routine HPV vaccination in practice in both the inpatient and outpatient setting. In particular, it is consistent with a recent study of family medicine residents and faculty, which showed that although residents received adequate training on the clinical importance and aspects of the HPV vaccine, their communication with families did not align with best practices for recommending the HPV vaccine. 18
A number of factors may explain inpatient provider hesitancy to discuss and offer the HPV vaccine, which may mirror reasons for limited vaccine uptake in the outpatient setting. Resident inpatient providers may be concerned about parental refusal of the vaccine, which has been cited in previous literature as a common barrier held by outpatient providers. 15 This misconception has a direct impact on parents’ decision to vaccinate—a recent systematic review found that “parents consistently cited health care professional recommendations as one of the most important factors in their decision to vaccinate their children.” 14 Additionally, residents may be unfamiliar with vaccine recommendations or inexperienced in counseling patients and families about the details of the vaccine. Some studies have revealed low knowledge among health care providers about medical sequelae of HPV infection,19,20 as well as lack of adherence to guidelines regarding target populations. For example, several qualitative studies showed that some health care professionals use a risk-based rather than universal approach, or preferentially vaccinate older instead of younger adolescents and girls instead of boys.20-22 This highlights the need for education directed at improving provider knowledge of HPV and comfort with addressing parental vaccine hesitancy. In fact, a study conducted at the Mayo Clinic found that increased clinician knowledge and decreased perception of parental barriers were associated with higher rates of vaccination. 23
Another major barrier specific to the inpatient setting may be the assumption that the primary care provider is managing vaccine counseling and administration during outpatient visits. However, research demonstrates that primary care physicians often have financial and logistical barriers to providing the HPV vaccine in the outpatient setting. 24 Furthermore, relying on outpatient vaccination is particularly problematic in the adolescent population because of their infrequent visits to primary care providers. Analysis of national Medical Expenditure Panel Survey (MEPS) data found that only half of adolescent patients see a primary care physician each year, and only one third have a preventative care visit. 12 Another longitudinal study of a large health plan in Minnesota found more dismal results—over a 4-year period, only 1% of commercially insured and 2% of government-insured adolescents had at least one preventative care visit annually over the 4 consecutive years studied. 13
It is also important to note that adolescent patients with chronic illnesses, who may be hospitalized frequently, are less likely to have routine preventative health care visits and are more likely to see a specialist, who may not regularly order vaccines, including the HPV vaccine.25,26 In addition, multiple studies have dispelled myths that chronically ill or disabled adolescents are not at risk for contracting sexually transmitted infections. 27 We now know that these patients are just as likely as their healthy counterparts to be sexually active, and are at higher risk for sexual abuse, placing them at risk for contracting sexually transmitted infections, including HPV. 28 However, studies have also shown that parents of children with special health care needs are less likely to perceive that their child may need the HPV vaccine than parents of healthy children. As a result, these children are more likely to have a parent refuse the HPV vaccine even if their outpatient provider has recommended it. 29 Thus, opportunistic immunization presents a particularly crucial intervention for this subset of patients who often have lengthy stays in the hospital, allowing time to counsel parents about the importance of HPV vaccination for their special health needs child.
Additional barriers may include systems-based concerns such as time constraints in the setting of a busy patient census, worries that the patient may be “too ill” to receive the vaccine, concerns regarding vaccine series completion once discharged from the hospital, policies and process barriers, or financial issues leading to difficulty in ordering, obtaining, or administering vaccines. There may be perceived pressures to forgo outpatient treatments such as vaccines due to diagnosis-related group-based reimbursement models. One barrier is simply a lack of resident education on opportunis-tic immunization—including inpatient admissions—to catch patients up on immunizations. Our study showed that greater than 90% of surveyed residents responded that they “usually/sometimes discussed” the primary childhood series or influenza vaccine with patients and families, but 60% or less actually “usually/sometimes offered” either of these. Past studies done in the outpatient setting have shown quality improvement (QI) methods to be effective in increasing HPV vaccination rates—specifically targeting education of providers and giving feedback. 30 Further research on the applicability of these methods in the inpatient setting could present a potential solution to this issue.
Limitations of our study include a small sample size in a specialized population—pediatric residents at a single large, tertiary, academic center serving a patient population that is largely Medicaid insured (72%)—and therefore may not be generalizable to all pediatric providers in every inpatient setting. In addition, the surveys were conducted as the first step in a larger QI initiative to increase resident HPV vaccine status documentation and vaccine administration in the inpatient setting. The survey was administered after the QI initiative had been introduced and resident education surrounding the importance of opportunistic immunization had taken place the prior year, thus senior residents (PGY-2 and PGY-3) may have been biased in their survey responses. However, we would expect this to overestimate resident discussion and offering of HPV vaccines, and we did not find any differences by training year. Additionally, our survey inquired about discussion and offering of vaccines at time of admission, but did not specifically inquire about vaccine practices during hospitalization or on discharge. While this may have led to an overall underestimation of residents’ discussion and offering of vaccines during hospitalization, it does not diminish the significant differences found between the HPV vaccine and other vaccines. Our survey was administered anonymously by paper and electronically; although both versions were identical in format and content, it is possible that there are differences by response modality. Also, although instructed not to, there is a chance that residents responded more than once. Finally, our study only evaluates self-reported behaviors and does not assess completeness of vaccine histories or vaccines ordered.
This study demonstrates a discrepancy between provider attitudes and self-reported practices regarding inpatient administration of the HPV vaccine compared with other inpatient immunizations; however, it does not explain why this discrepancy exists. Further studies are indicated to evaluate the reasons behind this variation. In addition, surveyed residents reported lower rates of discussion and offering of any of the 3 adolescent vaccines (Tdap, HPV, and meningococcal vaccines) compared with the influenza vaccine or primary series vaccines. Although our study showed statistical significance for a difference in how the HPV vaccine is discussed and offered in the inpatient setting, more studies are needed to further explore the differences in how adolescent vaccines, as a whole, are viewed in the hospital setting. Our study also found that females were more likely to discuss meningococcal vaccines; this difference was not accounted for by differences in level of training and has not been described in the literature. Further studies are needed to investigate this finding.
Given the large proportion of hospitalized adolescents that are underimmunized, understanding these differences may help in designing future educational programs and interventions to increase uptake of the HPV vaccine—and all other ACIP recommended adolescent vaccines—in the inpatient setting.
Conclusions
Pediatric residents were more likely to report that they never or rarely discuss or offer the HPV vaccine during hospitalization compared with Tdap, the primary childhood vaccine series, and influenza vaccines. While the majority of residents believed that patients should be offered adolescent vaccines during inpatient admissions, most residents do not routinely offer them to eligible patients during hospital stays. Further research is needed to evaluate interventions that may shift provider attitudes toward increased acceptance and practice of inpatient opportunistic immunization for the HPV and other adolescent vaccines.
Supplemental Material
Supplemental_Figure_1_JPEG – Supplemental material for Pediatric Resident Attitudes Toward Inpatient Immunization of Children and Adolescents: Highlighting Differences in Human Papillomavirus Vaccination
Supplemental material, Supplemental_Figure_1_JPEG for Pediatric Resident Attitudes Toward Inpatient Immunization of Children and Adolescents: Highlighting Differences in Human Papillomavirus Vaccination by Nora Pfaff, Chelsea Garnett, Alexandra J. Mihalek, Mary Rose Mamey and Susan Wu in Global Pediatric Health
Footnotes
Authors’ Note
Prior poster presentation of this work: Mihalek A, Pfaff N, Garnett C, Keefer M, Tanaka D, Arora G, Wu S. Opportunistic immunization of adolescents: increasing discussion and assessing provider attitudes about HPV vaccination in the inpatient setting. American Academy of Pediatrics (AAP) National Conference & Exhibition Section on Hospital Medicine, Chicago, IL (2017).
Author Contributions
NP: Contributed to conception and design; contributed to analysis; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CG: Contributed to conception and design; contributed to analysis; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AJM: Contributed to conception and design; contributed to analysis; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MRM: Contributed to analysis; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SW: Contributed to conception and design; contributed to analysis; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Susan Wu has stock in Eli Lilly and Company. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was done without a funding source.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.