
Abstract
Background. Education should support the gradual development of students’ necessary abilities to empower them in participating in decision-making together with health care professionals. Aim. The aim of this study was (1) to evaluate baseline knowledge regarding medication and medication wastage among primary school children and (2) to determine the short- and long-term effects of an educational intervention. Methods. Ten primary state schools around Malta were invited to participate; 5 accepted participation (3 control and 2 intervention). Children aged 9 to 12 years attending the sixth grade completed a self-reported questionnaire containing 20 questions, with total scores ranging from 0 to 20. Students from the intervention classes filled in a questionnaire pre and post an educational seminar. All students answered the questionnaire again after 8 months. ANOVA (analysis of variance) with repeated measures was used to compare difference between preintervention and postintervention mean scores. Results. Overall, 40.8% (160/392) of children participated. Mean ± SD age was 10 ± 0.4years; 52.5% (n = 84) were boys. Average preintervention knowledge score for all 5 schools was 11.5 ± 3.6, with 43.1% (n = 69) obtaining responses ≥13 (median). A repeated-measures ANOVA with a Greenhouse-Geisser correction determined that mean knowledge scores differed significantly between preintervention and postintervention (F[1, 81.000] = 75.190, P < .0005). Intervention students retained a significant increase in knowledge scores at 8 months (P = .026). Discussion and Conclusion. The significantly improved knowledge score following the educational intervention both in the short- and long-term demonstrated the success of the intervention. These findings provide a basis for the introduction of education about medication and medication wastage in schools.
Introduction
Knowledge About Medication Among School Children
The educational system, together with professionals, has been summoned to promote social well-being and health education. 1 Health education should provide students with the ability to become responsible individuals who are capable of making the right decisions in health rather than having others decide for them. 1 Individuals are exposed to medication from the time that they are born, mainly through personal use requirement, such as vaccinations, and also, at times, easy accessibility within households. 2 Therefore, educating students about medication as part of health education is imperative. 3 The US Pharmacopeia and the American School Health Association published a “Guide to Developing and Evaluating Medicine Education Programs and Materials for Children and Adolescents” almost 2 decades ago. 4 Studies have shown that while children and adolescents were knowledgeable about some aspects in relation to medication, such as what medications actually are, 5 in other areas knowledge was lacking, such as the effect of dose on efficacy of medication.5,6
Educational Interventions to Increase Health and Medication Knowledge Among School Children
Studies have dealt with educational interventions to improve knowledge of different health issues among school-aged children. Health awareness studies have shown that educational interventions increase knowledge scores. An intervention to improve knowledge in relation to HIV/AIDS enhanced students’ knowledge about sexual transmission from 50.0% to 95.0% and about mosquito bite transmission from 24.0% to 76.0%. Moreover, while only 34.0% of students were aware that there is no curative medication for HIV/AIDS, awareness was increased among 92.0% of students after the intervention. 7 A study that applied the Cancer Awareness Measure among 422 adolescents found that adolescents significantly identified 9 frequent cancer signs 2 weeks and 6 months following the intervention, with maintenance of awareness at a 6-month follow-up. 8 In the study by Ray et al, 9 cardiovascular health awareness increased from a score of 41.1 ± 10.5 to 48.1 ± 16.9. Knowledge about healthy lifestyles was also the target of some educational intervention studies. One study assessing breakfast eating habits by applying a questionnaire and an educational intervention, based on the theory of planned behavior, found an improvement in behavior of students’ intentions in eating breakfast and the actual breakfast-eating behavior after the intervention. 10
School-based educational interventions have also been carried out in relation to medication. Research to gauge short- and long-term effects of an educational intervention to encourage rational drug use and self-medication among 367 female students aged 10 to 13 years found a significant increase in knowledge both in the short- and long-term. 11 Yamada et al 12 conducted an educational lecture by school pharmacists to encourage rational medication use and self-medication in junior high school students. While 42.7% of students reported lack of confidence in buying medication alone without anyone’s guidance, this was decreased to 11.7% following the intervention. Lack of confidence in using medication by themselves was manifested in 25.2% of students before the intervention, which decreased to 12.6% after the intervention.
A survey study on medication wastage among the Maltese population revealed that age and awareness of medication wastage were significantly related, with younger respondents being much less likely to self-report awareness of issues of medication wastage. 13 Therefore, targeting the younger age group is a crucial step toward increasing awareness of medication wastage. Education should support the gradual development of students’ necessary abilities to empower them in participating in decision-making together with health care professionals when they require medication as adults. 14 Medication education programs in Malta are encouraged from the elementary years, and apart from the set syllabus within the “National Curriculum Framework” with the emphasis being on substance abuse, effective medication educational interventions from outside visitors are also accepted. 3 No published evidence was identified by the authors in relation to medication wastage education among school children. Thus, the aim of this study was (1) to evaluate baseline knowledge regarding medication and medication wastage among primary school children and (2) to determine the short- and long-term effects of an educational intervention.
Methods
Design
The study follows a positivist stance applying longitudinal survey methodology pre- and post-educational intervention.
Setting
The study was conducted in primary (elementary) state schools around Malta, a small island in the Mediterranean Sea. The study was approved by the Maltese Research and Policy Development Directorate and by the University of Malta Research Ethics Committee (UREC Reference Number: 21/2017). Heads of schools and parents had to give their written informed consent and children their written assent to participate.
Inclusion Criteria, Sampling, and Sample Size
Children of any gender aged 9 to 12 years attending sixth grade of a consenting primary state school in Malta were included. Schools were chosen by pairing all schools that had 4 or more classes in the sixth grade according to the Maltese region they are located in. Two schools from every region of Malta were chosen randomly to act as sampling sites, with the aim of including students from all the different geographical regions of Malta. First, a school was randomly selected per region to be part of the intervention group; then a school from each region of Malta was chosen randomly to form part of the control group. All selected schools were provided with an information letter and meetings were held with Heads of schools to discuss study logistics. Parents were handed an information letter containing details about the study and were given an email address to contact the research team if further information was required.
A minimum sample size of 385 students was required to give 95% confidence interval (CI) and 80% power assuming 50% response rate among students completing the preintervention questionnaire and 40% response rate among students completing the postintervention short-term questionnaire. Therefore, based on the study’s inclusion criteria, to obtain a sample size of 385 students, 5 schools had to be recruited. Assuming 50% response rate among schools consenting participation, 10 schools were recruited. To calculate the sample size of students receiving the intervention and to determine whether the educational intervention produced a significantly enhanced knowledge score, a minimum of 32 students receiving the intervention and completing both preintervention and short-term and long-term postintervention questionnaires was required. A 95% CI and an 80% power were used to detect a mean difference of 5 points on knowledge score and assuming a standard deviation (SD) in the mean difference scores of 10 points on knowledge score. 15
Questionnaire
On the day of the study, in October 2017, students accepting participation were asked to remain in their respective classrooms and completed a baseline anonymous, self-reported questionnaire without the teacher’s support. The main outcome of the questionnaire was knowledge about medication and medication wastage based on 20 questions. Questions were formatted in line with benchmark examinations paper styles. These examinations are mandatory for all sixth-grade state-school students across Malta. The questionnaire layout was designed by a teacher with a master’s degree in pedagogy and a professional graphic design house to enhance children’s readability and understanding of statements.
The first section of the questionnaire contained demographic questions. The knowledge section contained 3 parts. In the first part, students were provided with statements and for each statement, there were 3 optional answers to choose form. Students had to underline the correct answer. In the second part, students were provided with statements and they had to mark “yes,” “no,” or “sometimes” for each statement. In the third part, statements were provided with a blank space for students to fill it in with one word. Each correct answer was given a score of 1, while incorrect answers were given a score of 0. Scores of each item were summed up, with total scores ranging from 0 to 20. All 3 sections included knowledge statements about medication and medication wastage that children between the ages of 8 to 12 years should know.
Students were also asked whether they would like to know more about medication and whether teachers should teach them how to prevent medication wastage. One hour was allocated to complete the questionnaire. The questionnaire was assessed for face and content validity by 2 teachers who also commented on the design of the questionnaire. The content of the questionnaire was also reviewed by the Maltese Research and Policy Development Directorate and was amended following their feedback. Following amendment and formal submission to the Maltese Research and Policy Development Directorate, the study was approved by the Directorate.
Educational Intervention: Seminar About Medication and Medication Wastage
Following completion of the questionnaire, students from the intervention classes received a 45-minute seminar by the principal researcher, who is a clinical pharmacist, about medication and medication wastage, which was delivered in November 2017. The seminar took the form of an information-based speech supported by visual aids whereby students were allowed to interact by sharing comments or queries that they had. Toward the end of the session, the seminar evolved into an interactive quiz whereby students were provided with a series of images in relation to medication wastage, medication storage, and disposal and they had to state whether the images showed correct or incorrect practices. Content of the seminar and questionnaire about medication was based on the US Pharmacopeia and the American School Health Association 4 published “Guide to Developing and Evaluating Medicine Education Programs and Materials for Children and Adolescents.” Content about medication wastage was based on a Delphi study, which highlighted possible factors that lead to medication wastage. 16 Content on medication disposal was based on “Medicine Disposal: Questions and Answers” issued by the US Food and Drug Administration 17 and website of WasteServ Malta Limited. 18 Information was adapted for children between the ages of 8 and 12 years. The seminar content was constructed and discussed with a panel of pharmacists while the information and visual aids were appraised by a teacher with a master’s degree in pedagogy.
The seminar was carried out on a day and time chosen by the head of school. From the 2 consenting intervention schools, School A divided the consenting children into 2 groups and each group received the seminar in a classroom. School B gathered all consenting children in the school hall and received the seminar all together. The students’ questionnaire was repeated with all the participating classes receiving the seminar up to 1 month after termination of the seminar. The principal researcher was present when the students were completing the postintervention questionnaire to ensure that students fill in the questionnaire on their own and not with the support of teaching staff. The questionnaire was then repeated with the intervention schools 8 months postintervention to determine long-term knowledge. Schools that acted as control also completed the questionnaire at 8-month interval to ensure that impact on knowledge was not due to other external factors.
Data Analysis
Data were inputted into IBM SPSS Version 24 (IBM Corp, Armonk, NY; Released 2016, IBM SPSS Statistics for Windows, Version 24.0) and analyzed using descriptive statistics. Knowledge scores were dichotomized at the median, which was 13. Desire to know more about medication and medication wastage answers were converted to binomial data by combining the “No” and “I am not sure” options together. Chi-square test was used to determine any association between the desire to know more about medication/medication wastage and knowledge score above the median. One-way analysis of variance (ANOVA) was used to assess the differences in preintervention knowledge scores between the 5 schools and postintervention scores between the 2 schools receiving the intervention. ANOVA with repeated measures was used to compare difference between preintervention and postintervention mean scores. Post hoc tests using the Bonferroni correction were performed. 19
Results
Response Rate
From the 10 primary state schools that were chosen randomly, 5 schools accepted participation (2 from the intervention group and 3 from the control group).
Figure 1 indicates sample sizes per group and response rates.

Randomization of schools pre- and postintervention and respective response rates.
Demographics
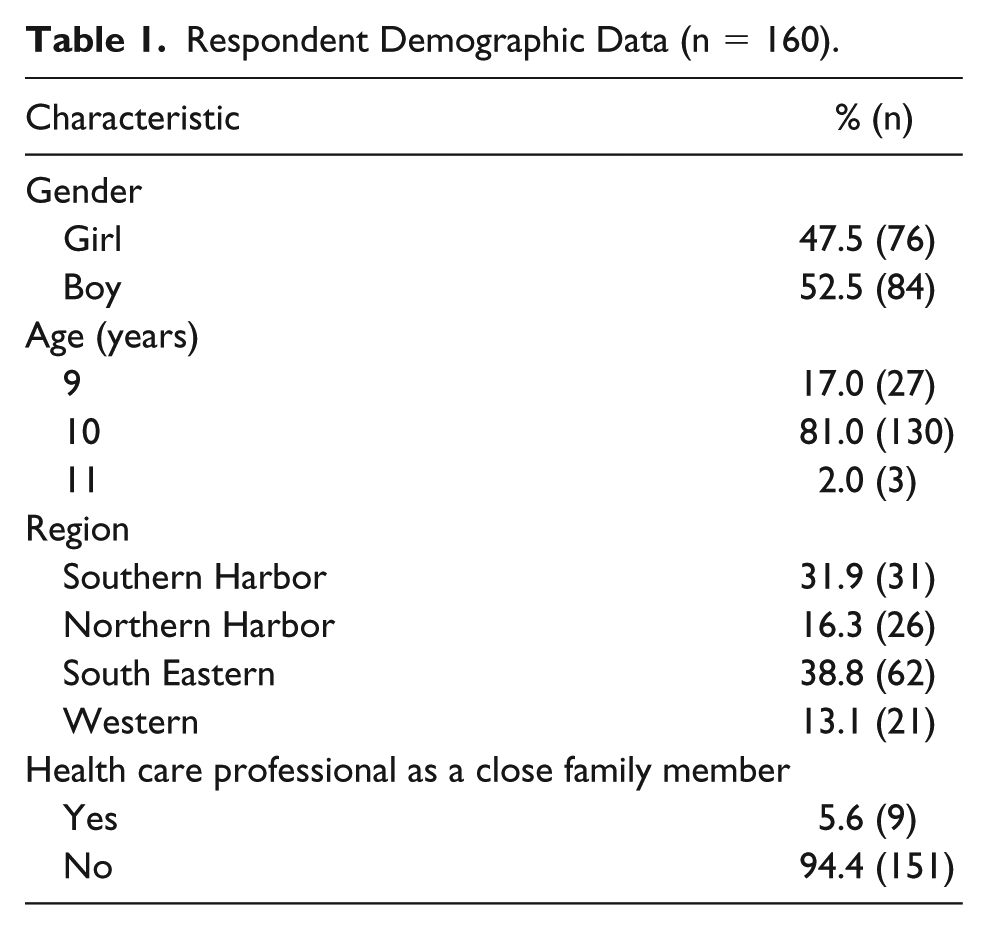
Table 1 demonstrates students’ demographics. Overall, 40.8% of children (160/392) participated in the study. The mean ± SD age was 10 ± 0.4years.
Respondent Demographic Data (n = 160).
Knowledge About Medication and Medication Wastage Preintervention
When asked if they knew any medication, 82.5% (n = 132) claimed that they knew at least one type of medication. Figure 2 indicates the different types of medication children claimed to know about.
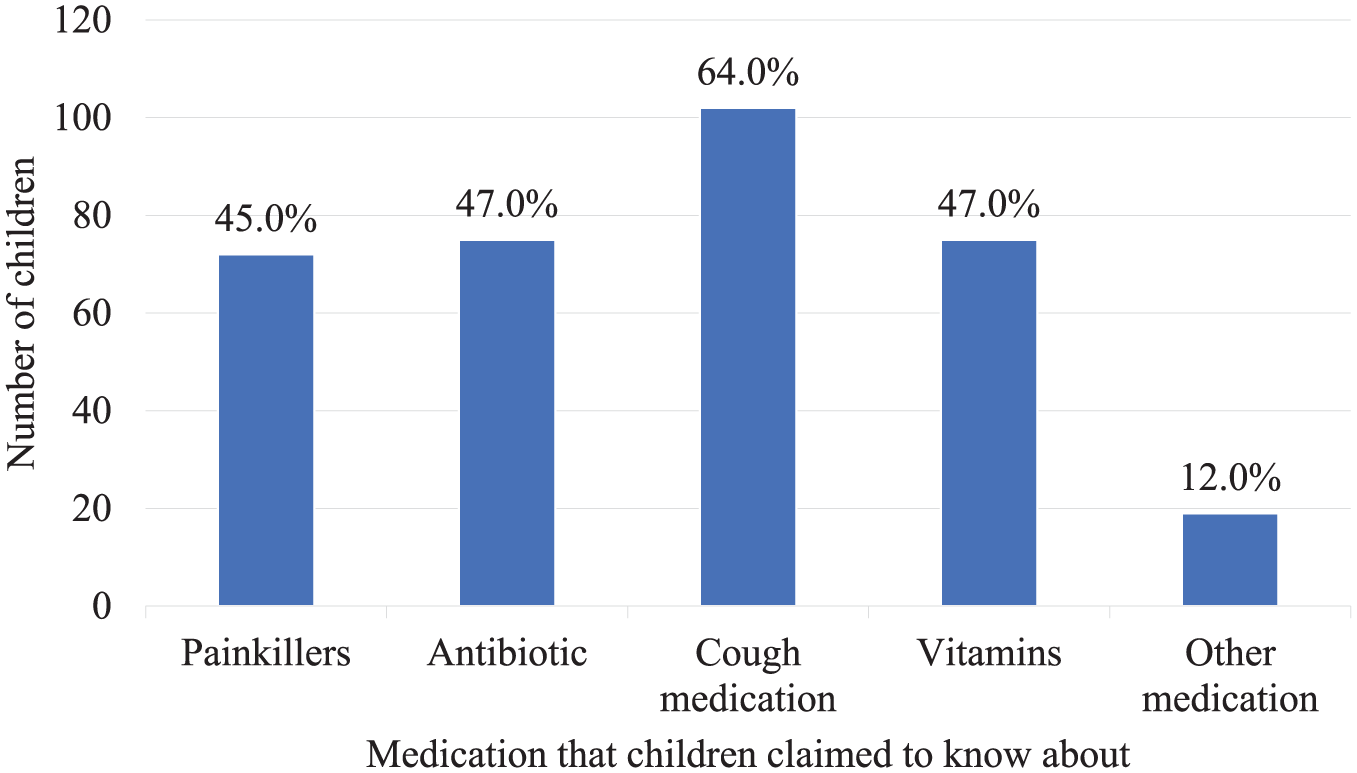
The different types of medication children claimed to know about.
Table 2 demonstrates the average preintervention knowledge score for each school separately and in total.
Average Preintervention Knowledge Score for Each Individual School.

There was a significant difference in knowledge in relation to medication/medication wastage between the 5 schools (P < .0005). Knowledge by “School C” was significantly higher than knowledge by “School B” (P < .0005, 95% CI = 1.37-6.51). Knowledge by “School E” was significantly higher than knowledge by “School B” (P = .015, 95% CI = 0.37-5.51).
Table 3 demonstrates knowledge statements provided to students and the respective correct values.
Knowledge Statements Provided to Students and the Respective Correct Values at Baseline.

Knowledge About Medication and Medication Wastage Postintervention
A repeated-measures ANOVA with a Greenhouse-Geisser correction determined that mean knowledge scores differed statistically significantly between preintervention and postintervention at 1-month interval (F[1, 81.000] = 75.190, P < .0005). Post hoc tests using the Bonferroni correction showed that the seminar produced an increase in knowledge scores from preintervention to postintervention (10.5 ± 3.4 vs 14.8 ± 3.7, respectively), which was statistically significant (P < .0005).
Since School A only repeated the questionnaire at the 8-month interval following the seminar, a repeated-measures ANOVA with a Greenhouse-Geisser correction for School A only determined that mean knowledge scores differed statistically significantly between preintervention and at 8 months following the intervention (F[1, 27.000] = 5.555, P = .026). Post hoc tests using the Bonferroni correction showed that the students retained an increase in knowledge scores from preintervention to 8 months postintervention in School A (11.7 ± 2.9 vs 13.2 ± 2.8, respectively), which was statistically significant (P = .026). However, there was also a significant decrease in knowledge between 1 month and at 8 months postintervention (P = .007).
Table 4 demonstrates the difference in students’ knowledge scores before and after receiving the educational seminar.
Difference in Students’ Knowledge Scores Before and 1 Month and 8 Months After Receiving the Seminar.

School B participated only at preintervention and 1-month postintervention.
Knowledge scores were significantly higher for School A when compared with School B at 1-month postintervention (P = .002).
There was a decrease in knowledge scores in the 2 schools that acted as control that accepted to complete the questionnaire at 8 months: Schools C and E, n = 21 (13.1 ± 3.7 at baseline vs 12.7 ± 4.0 at 8 months).
Desire by Students to Know More About Medication and Medication Wastage
Table 5 demonstrates students’ desire to know more about medication/medication wastage.
Desire by Students to Know More About Medication and Medication Wastage.

Desire to be taught more by their teachers about medication wastage and knowledge score above the median were significantly related, χ2 = 9.651, P = .008, df (degrees of freedom) = 2. Students who showed a desire to be taught more about medication wastage had more correct answers.
Among the 2 schools that received the intervention, after the seminar was delivered, a total of 58.5% of students showed a desire to know more about medication and 58.5% reported a desire to be taught more by their teachers about medication wastage.
Discussion
This study identified that 43.1% primary school students who completed the questionnaire had a baseline knowledge regarding medication and medication wastage at or above the median knowledge score of students. This could be due to participation bias, that is, children who were already interested in the topic participated in the study. Following the seminar knowledge scores increased significantly. However, less than one half of parents consented for their child to participate in the study. A contributing factor to this could be that some parents felt that their children are still young to discuss medications, as demonstrated by emails received by the principal researcher. Children may have their own perceptions and experiences about medications, which need to be discussed and addressed. Moreover, studies have shown that nonadherence issues are also present among children and adolescents. 20 Therefore, participation in such educational interventions should be encouraged. A self-reporting questionnaire among 14- to 16-year-old Maltese students showed that 90.3% of respondents had taken at least one medication in the previous 3 months. 21 In the current study, 82.5% of students knew at least one type of medication. Therefore, starting to educate children about medication and medication wastage from a young age contributes to their education in making good choices in life once they enter adulthood. 22 Moreover, parental participation with educators is imperative to enhance children’s health education. 1
In line with other studies,11,12 this study found a significant improvement in knowledge in the short-term following the seminar. However, having information and awareness about a given issue may not automatically lead to behavioral change. In fact, evidence is conflicting in this regard. An oral health educational intervention was found to be useful to enhance knowledge in relation to oral health significantly among 150 children aged 9 to 12 years. Yet, there were no significant differences detected in tooth brushing or dietary behaviors. 23 Other studies showed a positive effect of education on participants’ behaviors. An educational intervention affected positively the eating lifestyles of public school adolescents aged 10 to 14 years in Brazil, whereby a significant reduction in consumption of high-calorie foods was noticed after the intervention. 24 Therefore, while the intervention in the current study affected knowledge significantly, the long-term impact of the intervention on behavior needs to be measured.
While knowledge was retained significantly at 8 months in this study, knowledge scores decreased in the long-term during the 8 months following the intervention. The decrease in some of the intervention’s long-term beneficial effects has been shown in other studies. A study that explored the long-term benefit of a physical activity program among school children found that aerobic fitness remained significantly higher among children receiving the intervention. However, other benefits, such as body mass index and physical as well as psychological quality of life, observed in the short-term were not maintained. 25 These findings indicate the possible need of reinforcing the message delivered during educational interventions. In the interim, educational interventions in children should not be undermined as they could contribute toward a sustainable society and are imperative in forming the basis for “active and responsible citizenship.” 26
This study found that students who disclosed a higher desire to learn about medication wastage obtained significantly more correct answers than their peers. Teachers can enhance intrinsic motivation in children, 27 also known as the “enjoyment of learning.” 28 Yet, while the education system as well as the family environment could be the driving force for enhancing children’s motivation to learn, other factors such as genetics play a role.28,29 This study showed that, following the seminar, while knowledge was enhanced, desire to learn more on the subject did not show a significant increase. Some authors suggested student-specific educational strategies when developing interventions for students.28,29 Therefore, while the seminar has proved to be fruitful in increasing knowledge, it should be refined further to additionally target students’ intrinsic motivation. This will help students to enjoy learning about the subject, rather than merely having another topic on their busy curriculum. Moreover, the significant difference in knowledge postintervention noted between the 2 schools may be due to the fact that the school with higher knowledge scores received the intervention as 2 smaller groups of students. Therefore, such seminars should be delivered to small groups rather than to a whole assembly of students.
Limitations
A number of limitations need to be highlighted with regard to this study. Since half of the schools did not accept participation meant that not all regions of Malta were covered. Less than one half of parents consented for their child to participate in the study. While teachers were asked not to support students when completing the questionnaires, the principal researcher was not present during compilation of preintervention questionnaires. Therefore, knowledge scores at baseline may be an overestimate. The aim of the seminar was to convey knowledge to students about medication and medication wastage; other aspects of pedagogy need to be taken into account if the seminar is to be adopted within the school curriculum. The outcome measuring knowledge on its own does not necessarily reflect a change in behavior, and this needs to be acknowledged as a result of the current study. Education systems differ between different countries; therefore, extrapolation of results should be exercised with caution.
Implications for Policy and Practice
The Commission of the European Communities 30 affirms the importance of reducing wastage to support the appropriate utilization of limited resources. A definition of medication wastage generated through a consensus-based approach among stakeholders accentuates the educational relevance to reduce medication wastage. 16 In view of the paucity of previous studies in the area of medication wastage, this research could assist multiple stakeholders at various levels, including policy makers and educators, to establish an appropriate program that could be part of the broader health education schedule.
The European Commission 31 acknowledges the significance of education for the attainment of a sustainable future and places education as one of its propositions to be targeted for 2020. The significantly improved knowledge score following the educational intervention demonstrated the success of the seminar. Thus, findings of this study can provide a basis for policy makers and professionals to support health education and information. Educating and motivating students from a young age with the aim of knowledge and skills development around medication and prevention of medication wastage supports future generations in making informed and responsible decisions in this area. Prevention of medication wastage may have an economic and societal impact if the enhanced knowledge is translated into appropriate behavior.
Footnotes
Author Contributions
All authors have contributed significantly to the origin and design of the study. Lorna Marie West collected the data, analysed it and interpreted it and Maria Cordina checked data analysis and interpretation of data. Lorna Marie West drafted the article and Maria Cordina critically revised the content. Both authors approved this publication, are aware of the submission and agree with it.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research work disclosed in this publication is partially funded by the REACH HIGH Scholars Programme – Post Doctoral Grants. The grant is part-financed by the European Union, Operational Programme II – Cohesion Policy 2014 – 2020 ‘Investing in human capital to create more opportunities and promote the well-being of society’ – European Social Fund.