
Abstract
Objective. To evaluate the impact of an obesity didactic session for pediatric physicians on confidence in counseling and identified overweight/obesity and follow-up recommendations. Methods. Pediatric residents underwent training and completed pre/post online surveys evaluating confidence in obesity prevention and identification. A booster training occurred 1 year later. Pre-/post-training scores were compared using χ2 or Fisher’s exact tests. Electronic medical records data for patients ≥3 years with BMI-for-age percentile ≥85 during 3 months prior/following the training/booster compared frequency of overweight/obesity identification and follow-up recommendations (≤3 months recommended vs longer) using logistic regression adjusting for age and overweight/obese status. Results. Post trainings, improvements in confidence to define/screen for obesity were observed, with a decline between trainings. Overweight/obese identification and follow-up time recommendations improved post-training (identification: 14.2% to 27.4%, adjusted odds ratio [aOR] = 3.16, 95% confidence interval [CI] = 1.54-6.51; follow-up: 48.9% to 58.9%, aOR = 1.63, 95% CI = 1.01-2.64), aOR = 1.77, 95% CI = 1.10-2.85, and identification remained stable/above pre-training rates both pre-/post-booster (25.8%, aOR = 3.14, 95% CI = 1.53-6.45; and 22.1%, aOR = 2.57, 95% CI = 1.25-5.30, respectively). Recommended follow-up time rates continued to rise when measured pre-booster (60.6%, aOR = 1.77, 95% CI = 1.10-2.85), then declined (46.0%, aOR = 0.95, 95% CI = 0.60-1.52). Conclusion. This didactic session improved resident confidence in defining/screening, identification of overweight/obesity and follow-up recommendations; however, rates of identification remained low. The successes of this intervention support similar didactic sessions in residency programs and identifies opportunities for improved resident/attending education.
Introduction
Childhood obesity has increased 10-fold over the past 40 years, with nearly 1 in 5 children currently classified as either overweight or obese and approximately 17% of children classified as obese. 1 Furthermore, there is clear evidence that obesity prevalence is higher in low-income children. 2 Children who are overweight on kindergarten entry are likely to maintain their overweight status throughout childhood/adolescence, 3 and new evidence demonstrates worsening prevalence of obesity in children aged 2 to 5 years, 4 demonstrating a need to understand and identify overweight/obesity early in life. Given the frequency with which children receive care in a clinical setting in the first 5 years of life, as well as the long-term health consequences of these diagnoses, pediatricians are ideal individuals to target for training to improve comfort and skills in strategies for early prevention/detection/management of overweight or obesity. 5
Prevention and management strategies should ideally be implemented in the primary care setting,6,7 yet there is minimal standardization of curriculum for pediatric residents on the prevention, identification, or management of obesity in pediatric patients, with evidence that less than a quarter of all accredited pediatric programs offer a structured teaching curriculum on the evaluation, management, and counseling of obese or overweight patients. 8 This is in spite of evidence of growing perceived deficiencies and interest in further training in these skills by experienced pediatricians.
Prior studies have demonstrated that by training pediatric residents in childhood obesity prevention and identification techniques, there is an increase in confidence in their counseling, in resident satisfaction of these visits, in body mass index (BMI) recognition, in resident knowledge about obesity (specifically healthy eating, activity, and weight status), and in the frequency of these weight and lifestyle-related conversations.8-10 In an evaluation of methods for these curricula, studies have demonstrated that direct, simple training tools are more useful for resident education and comfort in obesity-related counseling in comparison to longer tutorial sessions.11,12 Brief training programs are also associated with positive behavior changes in patients. 13 Few studies have evaluated if training programs have affected physician identification of overweight/obesity in their visits, or the changes to their follow-up patterns with these patients if identified. Furthermore, few studies have focused on the use of electronic medical records (EMRs) to label and identify weight status or trended these results over time after the implementation of a repeat training session.
To address these gaps, we implemented a training program for pediatric residents and attending physicians to provide a brief review of strategies aimed at educating about obesity identification and management techniques. The training was inclusive of education on nutrition and physical activity recommendations as prevention strategies, as well as classification of overweight and obesity and recommendations if identified. EMR was utilized to identify the impact of the training session on rates of obesity detection and prescribed follow-up timing among overweight/obese patients, and physician surveys were used to assess perceived confidence in conducting weight and lifestyle counseling, with the expectation that, if the curriculum reached the objectives, there would be a trend toward increased identification and closer follow-up for patients with obesity/overweight as a chronic disease.
Methods
Physician Training
During the first year of the study, 35 pediatric residents and 6 attending physicians participated in a 15-minute obesity prevention/treatment training adapted from Nebraska’s Child Obesity Prevention Project’s Foster Healthy Weight in Youth provider toolkit. 14 The obesity prevention curriculum was delivered by a small team of residents (n = 2) and attending physicians (n = 1). It included calculating BMI, defining overweight versus obese, case discussions, as well as learning about the Youth Physical Activity & Nutrition Assessment Form, 14 which requires quantifying daily physical activity and screen time, breaking down diet history to quantify days of the week in which breakfast and meals out of home are eaten, and quantifying consumption of fruits, vegetables, milk products, whole grains, high fat or sugary foods, and sugar-sweetened drinks. The curriculum further detailed strategies for healthy eating/exercise related to the questions asked of patients and methods to sensitively approach these topics with patients and families.
A booster session was completed as additional training during the second year with 37 pediatric residents and 7 attending physicians, including first year residents for whom the material was introduced for the first time, and delivered by the same resident and attending curriculum team. It included the same obesity prevention curriculum. All sessions were conducted over the 15-minute didactic time allotted at the start of resident continuity clinic, located at a primary care site in a large, urban academic primary care practice. The sessions included interactive question and answer case-based scenarios and concluded with a tutorial of the EMR interventions as well as a reminder of the need to identify these diagnoses on the problem list and to schedule close follow-up once identified. The overall project timeline is described in Figure 1.

Timeline.
Data Collection
Ethical Approval and Informed Consent
This study was approved by the University Institutional Review Board (HP-00059163). EMR data were requested and delivered in de-identified batches through the generation of Epic EMR-based reports. Physicians provided written informed consent prior to completing surveys. Training was offered to all, regardless of participation in the study.
Impact of Training on Practice Outcomes
In order to assess the impact of the training on overweight/obesity detection and whether physicians implemented a more intensive treatment follow-up time (determined as ≤3 months, as per general policy of the clinic for follow-up of treatment of chronic illness) for patients with overweight/obesity, we extracted data from the EMR for all patients aged 3 years or older, with a BMI-for-age percentile ≥85th, and who had been seen for a well-child visit during the 3 months prior and 3 months following the training and booster. Extracted data included the following: patient demographics (gender, age), patient BMI-for-age percentile, diagnosis of overweight/obesity (inclusion on problem/diagnosis list within the Epic EMR), and specified time for follow-up.
Impact of Training on Physician Confidence in Prevention and Treatment of Overweight and Obesity
In order to assess the impact of the training on confidence related to topics in obesity treatment and prevention, a repeated cross-sectional design with a nested longitudinal subsample was used for this study. A 10-item survey 10 was adapted for brevity and inclusion of items within the training module and administered pre-post training and pre-post booster using e-mail survey software (SurveyMonkey, San Mateo, CA). Participants completed a pre- (1 week prior to training) and delayed post- (9 months following training) online survey evaluating their confidence in 8 areas of obesity prevention, identification, and counseling. This was repeated pre/post the booster session. Identifiers were not included in the physician questionnaires, thereby not allowing the research team to track individual trends in order to maintain anonymity of responses.
Data Analysis
For the EMR data, we compared demographic information among the 4 assessments, with χ2 tests or Fisher’s exact tests. Logistic regression models examined the odds ratios of identification of overweight/obesity on problem list and recommending follow-up time within 0 to 3 months, comparing each follow-up assessment to pre-training among patients who were overweight/obese. Age and obesity were examined as moderators of the above relations by including interaction terms in the models.
For the physician survey data, Fisher’s exact tests or χ2 tests were used to compare confidence in 8 areas of obesity prevention, identification, and counseling among the 4 assessments. Comparisons across each pair of assessments were conducted by restricting the analyses to 2 assessments per comparison.
Results
Impact of Training on Practice Outcomes
The EMR sample of overweight/obese patients from 3 months prior to/post training is described in Table 1. There were no differences in pooled patient demographics across time points (P > .05), n = 605. Overall, 54% (n = 327) of the patients were male, 52% (n = 315) were ages 3 to 5 years, with 6% (n = 45) of adolescent patients represented. Sixty-three percent (n = 380) were patients with overweight classification and 27% (n = 225) were patients with obesity classification out of those with BMI at or greater than 85th percentile.
Demographics of Overweight/Obese Patients Ages 3 to 19 Years From 3-Month Periods of Electronic Medical Record Data Pre/Post Training(s).

Ps are based on χ2 tests or Fisher exact tests, whichever are appropriate.
Overweight/Obesity Detection
Prior to training, 14.2% (n = 20) of patients with a BMI at or greater than 85th percentile were correctly identified as overweight or obese on the problem list within the EMR, which increased to 27.4% (n = 40) in the 3 months following training (see Table 1). At Follow-up #2 (3 months prior to the booster), 25.8% (n = 40) were correctly identified; and at Follow-up #3 (3 months post booster), 22.1% (n = 36) were correctly identified. In a logistic regression model (Table 2), adjusting for patient age and overweight versus obese status, patients were more likely to be identified as overweight/obese at each follow-up compared with the pre-training period (adjusted odds ratio [aOR] = 3.16, 95% confidence interval [CI] = 1.54-6.51, P < .05; aOR = 3.14, 95% CI = 1.53-6.45, P < .05; aOR = 2.57, 95% CI = 1.25-5.30, P < .05, respectively). No significant differences were found between the aORs among the follow-ups.
Logistic Regression Model to Examine the Odds Ratio of Overweight/Obesity Identification (Noting Overweight/Obesity on Problem List; 1 = Yes, 0 = No) Comparing the Follow-ups to Pre-Training Among Pediatric Patients Who Were Overweight/Obese.
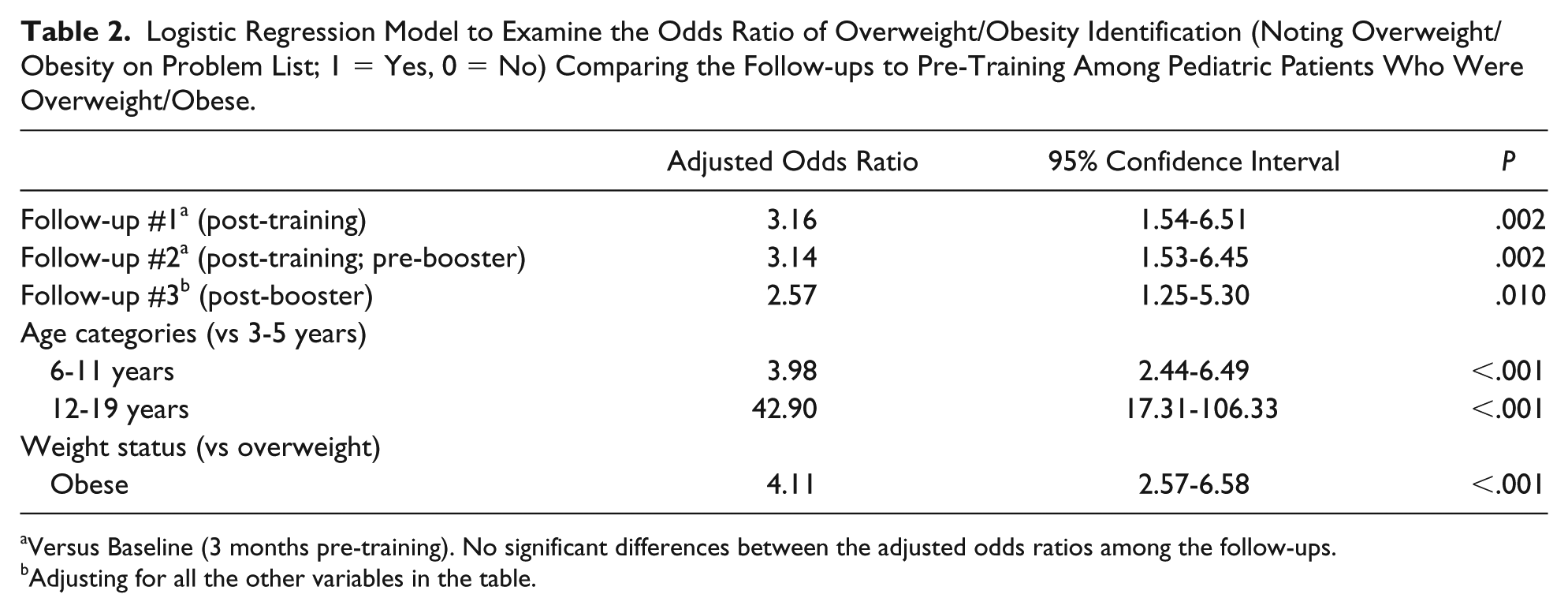
Versus Baseline (3 months pre-training). No significant differences between the adjusted odds ratios among the follow-ups.
Adjusting for all the other variables in the table.
Patients with overweight/obesity classification were more likely to be identified as such as they grew older, as shown in Table 2. Age was significantly related to obesity identification, with 6 to 11 year olds about 4 times and 12 to 19 years about 43 times more likely to be identified compared with 3 to 5 year olds (aOR = 3.98, 95% CI = 2.44-6.49, P < .001; aOR = 42.90, 95% CI = 17.31-106.33, P < .001, respectively). Patients with obesity (compared with overweight) were also more likely to be identified as overweight/obese in unadjusted models (aOR = 4.11, 95% CI = 2.57-6.58, P < .001). Age and obesity (vs overweight) were not significant moderators in the relation between the intervention and identification of overweight/obesity as a problem.
Follow-up Time
At pre-assessment, 48.9% of overweight/obese patients were suggested to follow-up within 3 months, which increased to 58.9% in the 3 months following training (see Table 1). A total of 60.6% of patients at Follow-up #2 and 46.0% of patients at Follow-up #3 were suggested to follow-up within 3 months. In a logistic regression model in Table 3, adjusting for patient age and overweight versus obese status, patients were significantly more likely to be suggested to follow-up within 3 months at Follow-up #1 (aOR = 1.63, 95% CI = 1.01-2.45, P = .047), and significantly more likely at Follow-up #2 (aOR = 1.77, 95% CI = 1.10-2.85, P = .018), compared with the pre-training period. No significance was seen at Follow-up #3 (P > .10). Significant differences in the odds between Follow-ups #1 and #3 (P < .05) and Follow-ups #2 and #3 (P < .05) were observed.
Logistic Regression Model to Examine the Odds Ratio of Recommendation of 3-Month or Less Follow-up Comparing the Follow-ups to Baseline Among Pediatric Patients Who Were Overweight/Obese.

Versus 3 months pre-training. There is significant difference in the odds between first and third follow-ups and second and third follow-ups (Ps < .05).
The adjusted odds ratios adjusted for all other variables in the table.
Age was also related to follow-up time outcomes, with 6 to 11 year olds less likely to receive a noted 3-month follow-up recommendation at any time (aOR = 0.61, 95% CI = 0.43-0.86, P = .005), but 12 to 19 year olds were more likely to receive such recommendation (aOR = 2.56, 95% CI = 1.16-5.66, P = .020). Patients with obesity were also more likely to have a 3-month follow-up recommendation compared with patients with overweight classification (aOR = 1.64, 95% CI = 1.16-2.33, P = .042). Neither age nor obese status were moderators in the relation between the intervention and a 3-month follow-up recommendation (Ps > .10).
Impact of Training on Physician Confidence in Obesity-Related Practice
The baseline survey was completed by the 41 physicians who attended the training session in August 2016 (100%) and more than half (58.5%, n = 24) of these completed the Follow-up #1 survey. A total of 24 physicians completed the pre-booster session survey (Follow-up #2), which is 54.5% of those who attended the booster training (n = 44). Of those who completed Follow-up #2, 66.7% (n = 16) completed Follow-up #3 (post-booster).
Overall, significant group differences were observed pre- versus post-training/booster in the percentage of (1) confidence in ability to define obesity in patients and to identify if a patient is overweight, (2) confidence in ability to screen patients for obesity and obesity risk factors, and (3) confidence in ability to manage a pediatric patient with established obesity (Ps < .05, Table 4).
Physician Confidence in 8 Areas of Obesity Prevention, Identification, and Counseling (% Agree/Strongly Agree) Across the 4 Assessments.

P value of follow-up versus baseline.
P values are based on Fisher exact test or χ2 tests, whichever is appropriate.
Boldface indicates statistical significance.
Following the initial training, improvements were observed in confidence in the ability to define obesity in patients and to identify if patients were overweight (70% pre to 96% post, P = .022), and ability to screen patients for obesity and obesity-related risk factors (60% pre to 87.5% post, P = .025).
A decline from Follow-up #1 was observed for each item (96% to 54% in ability to define obesity, P < .05; and 87% to 58% for ability to screen, P < .05). There were no significant differences between pre-training and Follow-up #2 in the prevalence for the 2 items. There were significant or marginally significant improvements from Follow-ups #2 to #3 after the booster training in the prevalence of the 2 items (54% to 88% for ability to define obesity, P = .040; and 58% to 88% for ability to screen patients, P = .079). For the confidence in ability to manage a pediatric patient with established obesity, there was increase from pre-training (39%) to Follow-up #1 (46%), but the increase was not statistically significant. There was a decline in the confidence in ability to manage overweight/obesity for Follow-up #2 to a prevalence significantly below pre-training (25%). For Follow-up #3, a significant increase was noted in the confidence of the ability to manage a pediatric patient with established obesity when compared with pre-training (39% to 75%, P = .02) and pre-booster (25% to 75%, P = .003).
Discussion
The results of our study demonstrated that a low-cost, minimally intensive educational intervention for pediatric residents was effective at improving the identification and closer follow-up for patients with overweight/obesity and improving confidence regarding obesity prevention and treatment in physician participants. This program could be widely implemented in continuity clinic education sessions in pediatric residencies given the brevity of the trainings, making it a unique intervention in comparison to much of the current literature. Many skills improved and were maintained for a 10-month follow-up period. While a continued trend toward improvement in identification and closer follow-up for patients with overweight and obesity status was not detected following the booster session, physicians’ perception of self-efficacy improved in several areas after the initial training, and it further improved after the booster session.
The prevalence of overweight/obesity identification on the EMR problem list was significantly increased after the first training and remained increased over a 10-month interval prior to the booster session. There was a slight drop off after the booster session, leading to a return that was not significantly above baseline rates. Importantly, even at the highest levels of identification, only 27.4% of patients within our selected age range with a BMI at or greater than 85th percentile were successfully identified on the problem list. Follow-up time recommendations for patients who met criteria for overweight/obesity were included as a primary outcome because evidence indicates that increased frequency of follow-up discussions with a medical professional may improve BMI in overweight/obese pediatric patients. 15 We observed a similar trend for follow-up time as presented for overweight/obesity identification, with a significant difference in recommendations toward a 3-month or less follow-up appointment for patients who were identified as overweight/obese, maintained and increased after 10 months following the initial training, but again returning to baseline rates after the booster session. These findings suggest that a different approach to the booster training, perhaps a variation of the original didactic session, more frequent boosters, or less distance between trainings may be needed to further improve on the findings from the initial training.
Overall, older patients and those who were obese (vs overweight) were more likely to be identified as overweight/obese by the physicians, which supports the current literature.16,17 Recent national data suggest an increase in the prevalence of overweight/obesity in the younger pediatric age ranges, 4 suggesting that more needs to be done to train physicians in both obesity prevention and detection among younger children. Opposite of the hypothesis, neither age nor weight status moderated the impact of the intervention on study outcomes, suggesting that the intervention was effective for all patients, regardless of age or weight status.
The intervention improved self-confidence in physicians’ ability to define, discuss the prevalence of, and screen for obesity in pediatric patients, which was further enhanced after the booster session. Physicians perceived improved ability to manage pediatric patients with established obesity, but not in their ability to provide information to parents or patients regarding the management of established moderate to severe obesity. Overall, these data suggest that the didactic session may have improved physician identification of illness without improvement in preventative strategies, which was a goal of the training sessions. Future didactics should further stress the importance of prevention efforts in a clinical setting.
An additional improvement in most study outcomes was not observed following the booster training. In other clinical skills trainings, booster sessions have been found to be a useful supplement, but this pattern was not demonstrated in the booster training sessions. 18 This may in part be a result of the fact that, while some members of the study group received both trainings, due to the cyclical pattern of residency initiation and graduation and the fact that the didactic sessions took place over 2 separate academic years, many participants only received 1 of the 2 trainings. Therefore, repeated training sessions within the same cohort of physicians should be further studied for ongoing value, as well as stratifying by year of training to account for variations in training experiences. It is also notable that prior booster trainings have demonstrated improvement in a simulation-based training, which may have benefit that extends beyond the ability of a didactic-only curriculum.
Limitations include an inability to trend individual patient patterns to demonstrate differences in their diet and lifestyle before and after the training sessions, since only EMR aggregate data were examined. Similarly, no identifiers were included in the physician questionnaires; therefore, individual improvements as a result of attending both training sessions could not be followed or trended across years of training. We were therefore also unable to determine their age or prior experiences with obesity medicine training or certifications. Future studies are needed to understand if improved self-efficacy by physicians will improve direct counseling for patients and in turn affect patient outcomes. Furthermore, overall low rates of identification within the EMR, even after improvements following the trainings, demonstrate that there is much to be gained from continued research in curriculum development and education of overweight/obesity. It is also likely that some discussion may have occurred outside of the documentation regarding weight and lifestyle changes that was not captured as an update on the problem list.
In conclusion, this brief didactic intervention demonstrated improvements in identification of overweight/obesity in pediatric patients, improved recommendation for follow-up times, particularly among pediatric patients who are older and with obesity, as well as improvements in self-efficacy among physicians for counseling and management of overweight/obesity, but did not demonstrate trends toward improvement in prevention strategies. Given that obesity continues to be a dominant concern in the pediatric population, it is important to examine the ways in which the next generation of pediatricians are being trained in the understanding, identification, and management of overweight/obesity issues, and educated in strategies for overweight/obesity prevention.
Footnotes
Author Contributions
Drs. Carter, Silber, and Weiss designed this study and carried out the intervention trainings. Drs. Wang and Hager and Ms. Sharaf oversaw the data analysis. All authors contributed to the primary composition of the article and participated in critical revision of the manuscript for intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported with funding by the Maryland State Community Health Resources Commission (grant #14-018). This funding agency played no role in the study design, data collection, analysis, interpretation of data, or the preparation of this manuscript.