
Abstract
There is a disproportionate burden of pediatric disease in low- and middle-income countries (LMICs); however, the proportion and relation of published articles to childhood disease burden in LMICs have not been assessed previously. This study aimed to determine whether published articles and disease topics from research conducted in LMICs in the most widely cited pediatric journals reflected the global burden of childhood disease. We reviewed all articles published from 2006 to 2015 in the 3 pediatric journals with the highest Eigenfactor scores to identify studies conducted in the World Bank–designated LMICs. We abstracted study topic, design, purpose, country, and funding sources. We derived descriptive statistics, Fisher’s exact χ2 test, Monte Carlo estimates, and Spearman’s rank order coefficients. Of the 19 676 articles reviewed, 10 494 were original research articles. Of those, 965 (9.2%) were conducted in LMICs. Over the study period, the proportion of published articles originating from LMICs increased (r2 = 0.77). Disease topics did not reflect the underlying burden of disease as measured in disability-adjusted life years (Spearman’s rank order coefficient = 0.25). Despite bearing the majority of the world’s burden of disease, articles from LMICs made up a small proportion of all published articles in the 3 pediatric journals with the highest Eigenfactor scores. The number of published articles from LMICs increased over the study period; nevertheless, the topics did not coincide with the burden of disease in LMICs. These discrepancies highlight the need for development of a research agenda to address the diseases that are the greatest threat to the majority of children worldwide.
Introduction
There is a disproportionate burden of pediatric diseases in low- and middle-income countries (LMICs) when compared with high-income countries (HICs).1-3 In 2015, sub-Saharan Africa contributed 50% and south Asia contributed 31% of under-5 deaths worldwide, according to a United Nations systematic analysis of childhood mortality. 2 Moreover, 98% of under-5 mortality worldwide occurs in LMICs. 2
Previous studies in the adult literature have demonstrated that there is underrepresentation of articles published on studies conducted in the parts of the world with the highest disease burden. 4 As little as 0.4% to 13.7% of articles published in internal medicine, surgery, tropical medicine, and psychiatry journals reported on studies conducted in LMICs.5-9 In pediatrics, studies comparing the number of clinical trials and the pediatric global burden of disease have shown only moderate correlation.10-13 However, studies assessing this relationship in the published literature are lacking. Published literature ultimately influences distribution of funding and other resources for clinical and public health work.
To date, no studies have assessed the proportion of pediatric published articles from LMICs compared with the pediatric global burden of disease. A more complete understanding of the representation of the global burden of disease in published articles has the potential to focus attention on the development of a research agenda to address the diseases and conditions that are the greatest threat to the world’s children. The objective of this study was to assess the proportion of articles from LMICs in pediatric journals with the highest Eigenfactor scores, and to determine whether published articles and disease topics from research conducted in LMICs reflected the pediatric burden of disease.
Method
This was a retrospective review of all articles published between January 1, 2006, and December 31, 2015, in the 3 pediatric journals with the highest Eigenfactor scores in 2015 (Pediatrics, Journal of Pediatrics, and Pediatric Infectious Disease Journal). Eigenfactor scoring includes several metrics to assess how widely read and cited a journal is at a given time.14,15 The 10-year study period was selected to assess contemporary trends over time.
All articles published during the study period were reviewed by 3 authors (EMK, HL, and CAR) to identify articles reporting on studies conducted in countries defined by the World Bank as LMIC, or those in which a LMIC was one of the study sites for research conducted in multiple countries. 16 To capture primary research that was conducted in LMICs, the following were excluded: editorials, historical articles, case reports, case series, commentaries, guidelines, biographies, conference summaries, interviews, review articles, meta-analyses, systematic reviews, and letters to editors. Supplements were excluded as they often contain invited articles and conference abstracts.
The reviewers assessed the published articles’ abstract and article text in their entirety. Data were compiled into a Microsoft Excel spreadsheet. Variables extracted from each article included journal name, year of publication, country or countries in which the research was conducted, topic studied, study purpose, study design, and funding source. Where study funding information was available, it was classified as originating from a HIC, LMIC, or, in cases where funding was obtained from both HIC and LMIC sources, as mixed HIC and LMIC. Study type was defined based on commonly recognized study designs. To capture the goal of each article, the authors used existing literature to define 8 categories of study purpose.17,18 Diseases studied were classified by research topics in global pediatrics, adapted from a list from the World Health Organization’s Global Health Estimates Summary Tables. 19 To represent global disease burden, summary disability-adjusted life year (DALY) estimates in children aged 0 to 14 years from 2012 from the World Health Organization’s Global Health Estimates Summary Tables were used.19,20 To ensure data acquisition quality, 15% of reviewed articles were randomly selected for review by other reviewers and interrater reliability was determined. Articles in which there were discrepancies in data collection were reviewed by all authors and discussed until consensus was achieved. Data were analyzed using Stata Special Edition 14.1 (Statacorp, College Station, TX). Descriptive statistics, Fisher’s exact χ2 test, Monte Carlo estimates, and Spearman’s rank order coefficients were calculated.
Ethical Approval and Informed Consent
Institutional review board approval was not required for this retrospective review as this study did not involve human subjects.
Results
There were 19 676 total articles published during the study period, 10 494 of which met inclusion criteria, and of those, 965 (9.2%) were articles conducted in LMICs (Figure 1). The vast majority of articles were single-country studies (n = 826, 85.6%) with only 139 (14.4%) conducted in more than 1 country. Using standardized calculations, 21 the interrater reliability for the classification of 3 article characteristics (study topic, design, and purpose) was high (κ = .82), but given that it was not one, there was not an exact match in every instance for all 3 characteristics. All differences in classification were discussed iteratively until consensus was achieved.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for article inclusion and exclusion from the 3 journals in pediatrics with the highest Eigenfactor scores* from 2006 to 2015.
Of the articles conducted in LMICs, 573 (59.4%) were from upper-middle-income countries, 262 (27.2%) were from lower-middle-income countries, and 130 (13.5%) were from low-income countries (Pearson χ2 = 0.008; Table 1). Forty-five percent of the articles (n = 435) reported on studies from 5 countries: Brazil (n = 123, 12.7%), China (n = 102, 10.6%), South Africa (n = 91, 9.4%), India (n = 62, 6.4%), and Thailand (n = 57, 5.9%). Over the 10-year study period, the proportion of publications in the 3 pediatric journals with the highest Eigenfactor scores conducted in LMICs increased. There was a significant positive correlation in the proportion of published global health articles and time during the 10-year study period (r2 = 0.77, P = .009; Figure 2).
Proportion of Articles From Low- and Middle-Income Countries in the 3 Journals in Pediatrics With the Highest Eigenfactor Scores From 2006 to 2015.

Pearson χ2 P value: .008.

Proportion of articles from low- and middle-income countries over all articles meeting inclusion criteria in the 3 journals in pediatrics with the highest Eigenfactor scores* from 2006 to 2015.
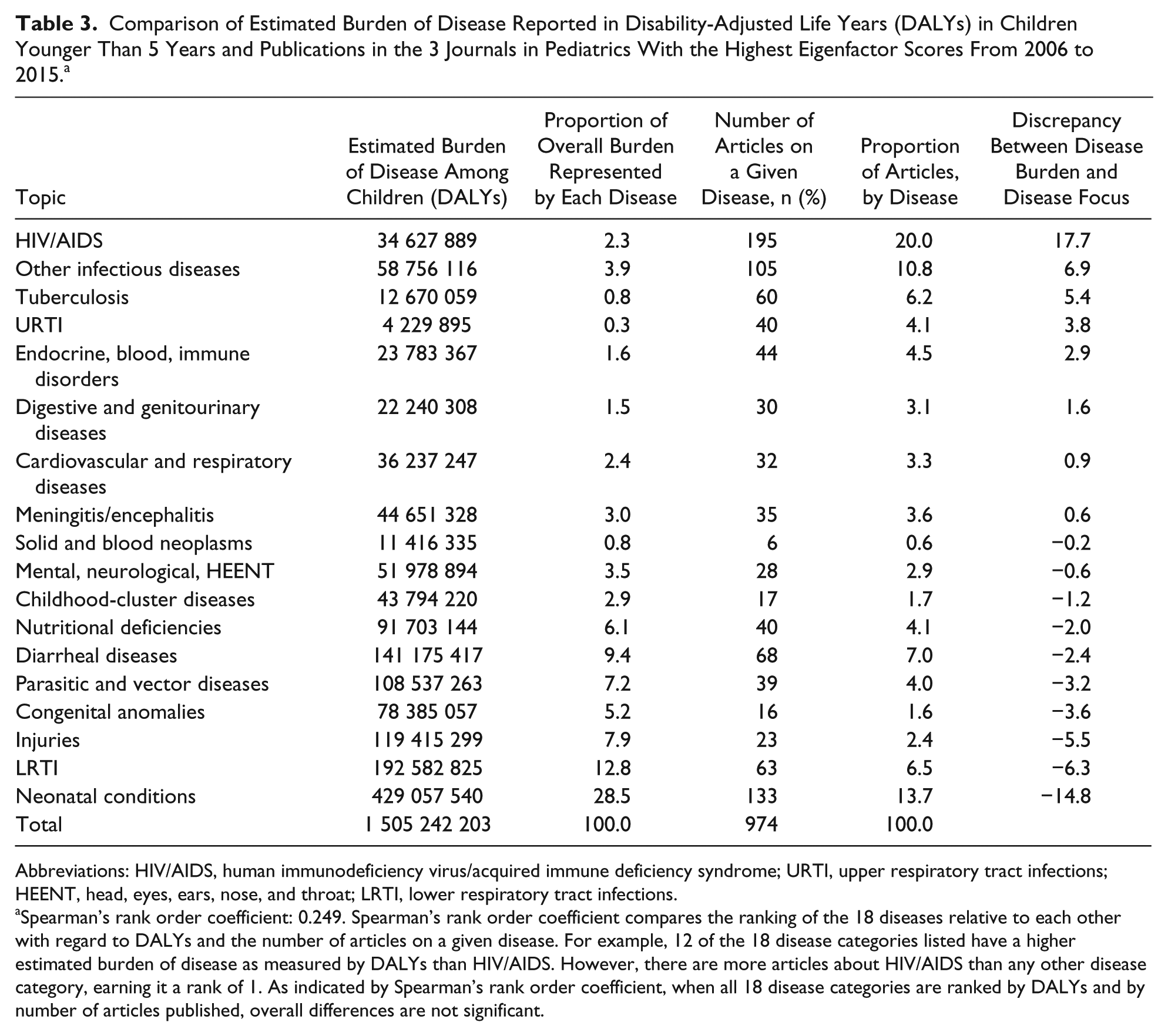
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), neonatal conditions, infectious diseases classified by the World Health Organization’s Global Health Estimates Summary Tables as “other infectious diseases,” and vaccines were the most common disease topics found in articles reporting on studies conducted in LMICs (Table 2). When we compared disease topics by countries’ income category, we found significant differences across approximately one third of the comparisons among upper-middle-income countries, lower-middle-income countries, and low-income countries (Table 2). Published study topics from articles included in this study did not reflect the underlying burden of disease as measured in DALYs (Table 3). The disease topic that most outstripped the underlying global burden of disease was HIV/AIDS (discrepancy of +17.7), while the topic most underrepresented disease topic relative to the underlying burden of disease was neonatal conditions (discrepancy of −14.8). There was a weak correlation between disease burden and number of articles on a particular disease topic (Spearman’s rank order coefficient = 0.25, P = .32).
Number of Articles From Low- and Middle-Income Countries in the 3 Pediatric Journals With the Highest Eigenfactor Scores From 2006 to 2015 by Disease Topic.

Abbreviations: HIV/AIDS, human immunodeficiency virus/acquired immune deficiency syndrome; LRTI, lower respiratory tract infections; URTI, upper respiratory tract infections; HEENT, head, eyes, ears, nose, and throat.
Comparison of Estimated Burden of Disease Reported in Disability-Adjusted Life Years (DALYs) in Children Younger Than 5 Years and Publications in the 3 Journals in Pediatrics With the Highest Eigenfactor Scores From 2006 to 2015. a
Abbreviations: HIV/AIDS, human immunodeficiency virus/acquired immune deficiency syndrome; URTI, upper respiratory tract infections; HEENT, head, eyes, ears, nose, and throat; LRTI, lower respiratory tract infections.
Spearman’s rank order coefficient: 0.249. Spearman’s rank order coefficient compares the ranking of the 18 diseases relative to each other with regard to DALYs and the number of articles on a given disease. For example, 12 of the 18 disease categories listed have a higher estimated burden of disease as measured by DALYs than HIV/AIDS. However, there are more articles about HIV/AIDS than any other disease category, earning it a rank of 1. As indicated by Spearman’s rank order coefficient, when all 18 disease categories are ranked by DALYs and by number of articles published, overall differences are not significant.
The most common study designs were prospective cohort studies (n = 335, 34.7%), cross-sectional studies (n = 243, 25.2%), randomized controlled trials (n = 179, 18.5%), and retrospective cohort studies (n = 104, 10.8%). Articles employing case control, program descriptions, qualitative, or other study designs collectively comprised 10% (n = 104) of articles meeting inclusion criteria. There were statistically significant differences in study designs by the World Bank income designations (contingency coefficient Monte Carlo test [10 000 samples, P < .001]; Table 4). Comparing study design by the World Bank region, prospective cohort and cross-sectional study designs dominated in all regions. Randomized controlled trials were least represented in sub-Saharan Africa, where they accounted for just 13.2% (n = 38) of articles published.
Comparison of Study Type by Study Country Income Bracket in the 3 Pediatric Journals With the Highest Eigenfactor Scores From 2006 to 2015. a
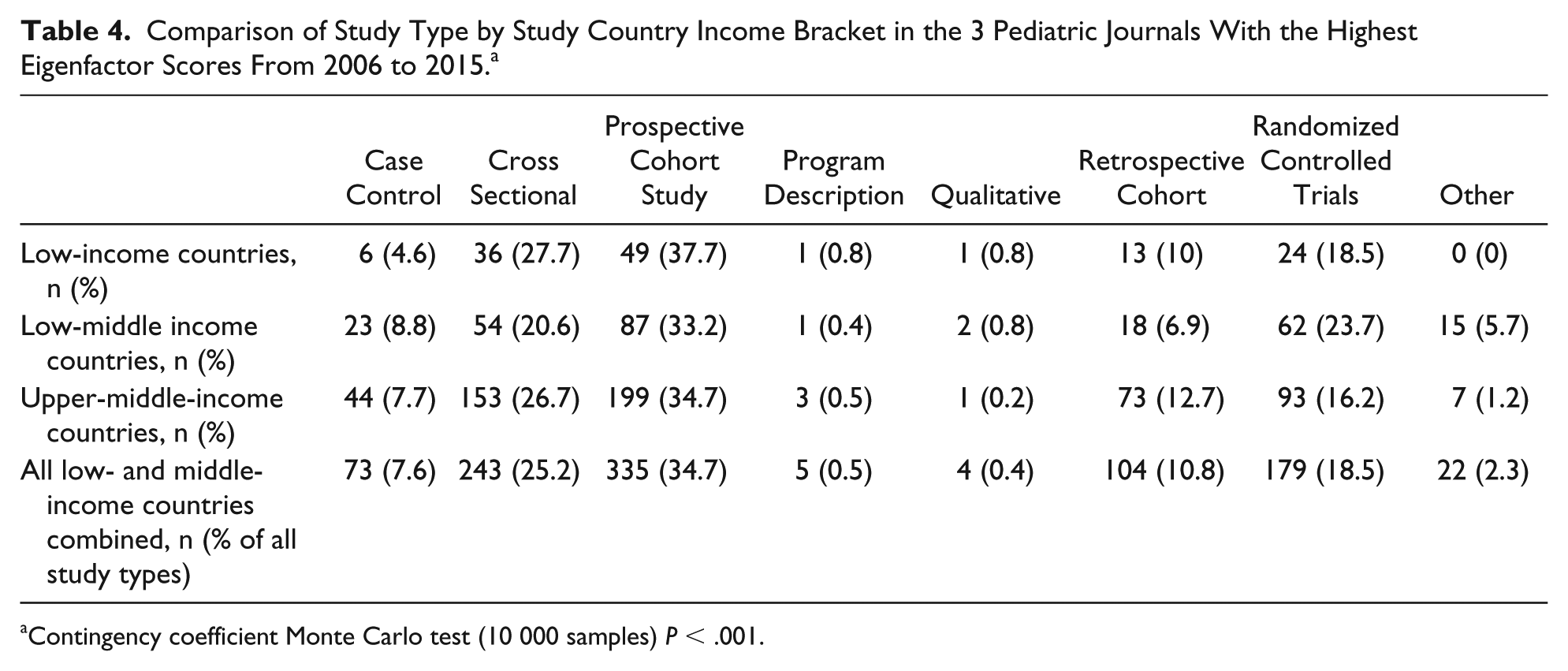
Contingency coefficient Monte Carlo test (10 000 samples) P < .001.
The most common study purposes found in the included articles were epidemiologic investigations (n = 289, 30.0%), diagnosis (n = 211, 21.9%), and therapy (n = 180, 18.7%). Less common study purposes included prevention (n = 99, 10.3%), prognosis (n = 92, 9.5%), harm (n = 56, 5.8%), and health services (n = 36, 3.7%).
Of the 745 articles for which funding information was listed, only 20.0% (n = 149) were funded exclusively by LMIC sources, while 66.7% (n = 497) were funded exclusively by HIC sources and 13.3% (n = 99) by mixed HIC and LMIC sources. Of the 179 articles reporting on randomized controlled trials, 24.8% were funded by HIC sources compared with 12.1% that were funded by LMIC sources and 11.1% that were funded by mixed HIC and LMIC sources. Among studies that were exclusively funded by LMIC sources, cross-sectional (n = 42, 28.2%) and prospective cohort (n = 51, 34.2%) study designs were most common.
Discussion
Published articles reporting on studies conducted in countries accounting for most of the world’s childhood morbidity and mortality made up a small proportion of articles in the 3 pediatric journals with the highest Eigenfactor scores over the 10 years. In addition, articles from upper-middle-income countries were much more common than articles from low-income countries. Most studies employed prospective cohort or cross-sectional study designs, and most of the studies conducted in LMICs that we evaluated were funded exclusively by HIC sources.
Although the correlation between pediatric clinical trials and disease burden has been studied,10-13 our study adds to the literature as this is the first study that we know of that evaluates disparities between pediatric disease burden and the actual focus of pediatric publications from LMICs. The low proportion of articles from LMICs in the pediatric literature mirrors what has been shown in other fields and in clinical trials.10,12,22 There are several possible explanations for the disparity between disease burden and published research in LMICs. Most research funding agencies are in HICs and researchers conducting studies in LMICs may find it difficult to access such funds. 23 In addition, limited research training programs and fewer trained researchers may hamper investigations in LMICs. 22 The international emigration of highly skilled researchers from lower to higher resourced areas further widens the gap between LMICs and HICs. 24 Furthermore, for many LMIC authors, English is a second language, and these authors may struggle to publish research when they are not entirely fluent in English. Some studies show that researchers from LMICs are underrepresented on editorial boards of journals, thus further biasing the focus of studies carried out in LMICs.25,26 Finally, lack of support for research from local governments, local institutions, and international agencies has also been cited as a reason for fewer publications in LMICs. 25 Authors from LMICs may not have the finances to fund expensive publishing fees and thus seek out local journals without fees that may not have as wide of a readership base. In response to this issue, many journals in HICs are starting to develop programs that have decreased publishing fees for authors from LMICs. 27
This study showed an increase in the proportion of articles from LMICs over the study period. This is similar to trends seen in the psychiatry literature where an increased proportion of articles from LMICs was observed from 2001 to 2011. 28 Other studies have shown a significant increase in health research in the World Health Organization–designated Africa Region from 2000 to 2015. 29 In addition, in recent years, there has been greater effort to increase research productivity from LMICs. Moreover, the World Health Organization Strategy on Research for Health outlines a roadmap to improve global health research standards and national capacity for research. 30 It is important to note that an increase in published articles from studies conducted in LMICs over time does not imply that these studies address local priorities or build local research capacity.31,32 Thus, researchers from HICs who are working in LMICs should seek to establish local partnerships to ensure that local disease burden is prioritized.
Articles published in the 3 pediatric journals with the highest Eigenfactor scores did not reflect the underlying burden of disease. This finding is supported by other studies, including several adult-focused reviews that have documented a weak association between burden of disease and published articles.13,33 In addition, 2 reviews of all clinical trials, one in global pediatrics clinical trials and one exclusively focused on clinical trials in Latin America, found discrepancies between studied disease topics and global disease burden.10,34 A study assessing 8 years of publications in the New England Journal of Medicine found that only 3.0% of articles addressed health issues in LMICs with the majority of those focusing on HIV and communicable diseases. 35 The current study is consistent with these findings, as the largest study topic was HIV/AIDS even though HIV/AIDS is not among the top 3 causes of child mortality. 36 In order to improve child health, topics that address the global burden of disease must be prioritized. One group that has made major contributions to the understanding of the leading causes of child death globally is the Child Health Epidemiology Reference Group, which is working toward identifying research gap areas and prioritizing child health in research agendas. 37
This study showed that randomized controlled trials, which are widely considered the gold standard of clinical research, were less common in published articles from low- and lower-middle-income countries compared with upper-middle-income countries. This supports the findings of other studies on pediatric clinical trials, which found that only a small minority of registered clinical trials took place in low-income countries.10,12 Additionally, a recent analysis of pediatric clinical trials found that only 7.1% of trials had study sites in Africa. 38 However, more than one third of pediatric clinical investigational trials conducted under the Pediatric Exclusivity Provision were carried out in LMICs.39,40 This may suggest a shift in clinical trial location toward LMIC settings in some regions. However, since the trials in LMIC settings in the Pediatric Exclusivity Provision were largely funded by non-LMIC sources, it is likely that LMIC governments may not be able to afford clinical research when there are many other demands on health care budgets. Furthermore, this study showed a lower percentage of qualitative and program description studies in LMICs, perhaps reflecting a lack of training in these particular areas of research.
Most of the articles on studies conducted in LMICs in this study investigated epidemiologic patterns, therapies, and diagnostics, while a minority considered prevention or health systems issues. The trend toward therapy and diagnostic studies may be partially explained by pharmaceutical industries’ support of research in LMICs, where pharmaceutical and device companies may find it less expensive to conduct research.41,42 The strict regulatory environments in many HICs have also played a role in where trials are conducted. 41 However, this globalization of clinical research raises important questions around the ethical standards of these trials, as well as whether their results are generalizable to HIC settings where pharmaceutical companies may have their biggest markets. 41
Our research has several limitations. First, this study only included articles published in the 3 pediatrics journals with the highest Eigenfactor scores and thus was unable to provide an assessment of all pediatric research. Furthermore, all 3 journals are based in HICs (Pediatrics and Journal of Pediatrics in the United States and Pediatric Infectious Disease Journal in the United Kingdom), which may contribute to a publishing bias in favor of articles from these countries. Also, these journals are published in English, which may hinder submission from authors from LMICs who speak English as a second language. In addition, 1 of the 3 journals, Pediatric Infectious Disease Journal, is topically focused and thus inherently publishes more articles on infectious diseases. Despite these limitations, these journals represent the most widely read pediatric literature. Since most articles did not include a breakdown of funding, in those cases where multiple funding sources were listed, it was not possible to identify if certain sources contributed more than others. Furthermore, DALYs were used to compare disease burden and research topic, which may underestimate or overestimate disease burden, even though they are a widely accepted metric for estimating morbidity.
Conclusions
With regard to LMICs, there are multiple disparities in the pediatric literature. These include overall representation of published articles, as well as the global burden of pediatric disease relative to study focus, funding source, and the country in which the study was conducted. While published articles from LMICs increased over the study period, the published topics did not coincide with the pediatric global burden of disease in LMICs. By recognizing these disparities, donors and researchers may develop a research agenda that better reflects the diseases and conditions that are the greatest threat to a majority of the world’s children.
Footnotes
Author Contributions
EMK, HH, MHS, and CAR: made substantial contributions to the concept and design of the work; acquisition, analysis, and interpretation of the data; drafting of the article; approved the version to be published; and take public responsibility for the content.
KAD: made substantial contributions to the design of the work and analysis of the data; revised the article critically for important intellectual content; approved the version to be published; and takes public responsibility for the content.
SAL, GES, and PNK: made substantial contributions to the design of the work and interpretation of the data; revised the article critically for important intellectual content; approved the version to be published; and takes public responsibility for the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.