
Abstract
Objective. To understand the perspectives of clinical providers and caregivers regarding early childhood development (ECD) in children born to HIV-infected mothers in Kenya. Methods. This was a qualitative study of provider and caregiver perspectives on ECD at 5 Kenyan HIV clinics, using semistructured interviews and focus group discussions. Constant comparison and triangulation methods were employed to elucidate the concepts of ECD. Results. Twenty-five providers and 67 caregivers participated. While providers understood ECD in terms of milestones, caregivers strongly equated ECD with physical growth. Factors affecting ECD, such as nutrition, perinatal effects, and illness, were perceived differently by providers and caregivers. Both groups generally believed that HIV-infected children would have typical ECD if adherent to their HIV treatment. Conclusions. Important considerations regarding ECD in this population were uncovered. Understanding provider and caregiver perspectives’ on ECD in HIV-exposed children is critical for promoting ECD in this community.
Keywords
Introduction
Despite increasing attention to early childhood development (ECD) in international settings, it is estimated that 43% (250 million) of children <5 years living in low- and middle-income countries may not reach their full developmental potential. 1 This loss of human potential is associated with an approximate 20% deficit in adult income, which has significant implications for individual and national economic development. 2 The United Nations Sustainable Development Goals, as well as international organizations and governments, are focused on addressing this loss through strategic frameworks to ensure that young children are reaching their full potential.3,4
Children living in the Republic of Kenya have multiple risk factors for poor developmental outcomes. Forty-two percent of Kenya’s population live below the poverty line. 5 Stunting, or a height-for-age Z-score more than 2 standard deviations below the median, is a known proxy for development delays and is present in 35% of Kenyan children. 5 Chronic and recurrent infectious diseases, including diarrhea, malaria, tuberculosis, and human immunodeficiency virus (HIV), also have a significant role in Kenyan children’s overall health and development. 5 In particular, every year, approximately 70 000 to 100 000 Kenyan children are born to mothers who are HIV-infected (8% of all births), which often comes with multiple risk factors for worse developmental outcomes, such as malnutrition and maternal depression.6-9 Across studies, children born to HIV-infected mothers are more likely to have cognitive and motor delays compared with their unexposed peers, making this population particularly vulnerable.10-12
In an effort to address ECD, Kenya’s Ministry of Education created policy and guidelines outlining the implementation of ECD programs within the country, including special needs services.4,13 Yet while policy and guidelines for ECD exist in Kenya, little is known about the experiences and knowledge of ECD from clinical providers and caregivers of children born to HIV-infected mothers in this setting. Awareness of these perspectives is an important first step in understanding how ECD services are integrated within the communities needing them the most. Therefore, the primary objective of this study is to understand perspectives of ECD and development delays from clinical providers and caregivers of children born to HIV-infected mothers to help guide ECD promotion in this population.
Methods
Study Setting
This qualitative study was conducted at 5 HIV clinics within the Academic Model Providing Access to Healthcare (AMPATH) program in western Kenya. AMPATH is a long-standing collaboration between Moi University School of Medicine, Moi Teaching and Referral Hospital, and a consortium of North American academic medical centers led by the Indiana University School of Medicine. 14 Through AMPATH, comprehensive HIV care services are provided at 25 semirural and urban clinics and 40 satellite clinics in western Kenya. The 5 clinics included in this study were selected to strengthen the representativeness of providers and caregivers within AMPATH settings with varying levels of pediatric population sizes, levels of urbanization, and ethnic diversity. At the conclusion of this study, the urban site (site 1) had nearly 15 000 individuals actively in care; site 2 with nearly 8000 individuals; site 3 with approximately 3700 individuals; and site 4 and site 5 each with <3000 individuals actively in care (Figure 1). 15

Clinical sites of research study: site 1 represented with “20”; site 2 represented with “18”; site 3 represented with “34”; site 4 represented with “26”; and site 5 represented with “32.”
Study Participants, Recruitment, and Sampling
We performed semistructured interviews with clinical providers caring for HIV-exposed and HIV-infected children and focus group discussions with caregivers of HIV-infected children. We chose semistructured interviews for providers to address topics specific to their individual training and experiences, while allowing for further pursuit of an idea or response. 16 Focus group discussions were chosen for caregivers to generate collective views of development and the implications behind those views. 16 Private interviews were offered to caregivers of a child with a known developmental delay. Each focus group discussion had 8 to 12 participants. Convenience sampling was used, with the guidance of clinic leadership. In following cultural norms, we requested that the clinic manager at each site choose up to 5 clinical providers who met the inclusion criteria. Each clinical site was limited to 5 interviews due to prior knowledge of the number of pediatric providers at each clinic, as well as time constraints while visiting each clinic. All clinical providers identified by the clinic manager as potential participants agreed to enroll in this study. Inclusion criteria for providers included providing clinical care at the AMPATH clinic and working with children <5 years old and their families. Caregivers were recruited by a study liaison, who was identified by the clinic manager at each study site. The study liaison was often a social worker or someone familiar with the families attending clinic. The eligible participants were informed about the study when they were coming in for a clinic visit. Inclusion criteria for caregivers included being a primary caregiver for a young (<8 years) HIV-infected child attending an AMPATH clinic. The study liaison organized a group of potential caregiver study participants, with whom our research team met with and discussed the details of the study. All caregivers identified by the liaison as potential participants agreed to enroll in this study.
Discussion Guides
We created interview guides using input from local pediatric health care providers, literature on developmental assessments, and the Health Belief Model to help determine perspectives of ECDs. 17 The Health Belief Model contains concepts that predict why people may take action to prevent, screen for, or treat a medical condition. 17 These qualitative methods are particularly useful in cross-cultural settings to understand perspectives regarding medical conditions, as they allow for a more complete description of the topic of interest. 18 Separate interview guides were used for providers’ semistructured interviews and caregivers’ focus group discussions; however, both covered similar themes related to ECD, including the following: general understanding of ECD; factors affecting development; additional considerations for children born to HIV-infected mothers; and identification and treatment of development delays (interview guides available on request). Providers were additionally asked about developmental assessments and referrals.
Data Collection and Management
Twenty-five semistructured interviews and 7 focus group discussions (3 at the urban site and 1 at each semirural clinic) took place between March and June 2016. Prior to data collection, the study protocol and interview guides were extensively reviewed with the 3 interviewers during training. Data collection for the semistructured interviews and focus group discussions was conducted in a private, quiet room within the AMPATH clinics. Semistructured interviews lasted 30 to 60 minutes, and focus group discussions lasted 60 to 120 minutes. Participants received refreshments and US$2 to compensate for travel. Semistructured interviews and focus group discussions were audio-recorded, transcribed verbatim, and then translated from Swahili into English, if necessary.
Data Analysis
All interview transcripts were analyzed for themes within the participants’ understanding of ECD and factors influencing development delays (transcripts are available on request). First, we created a priori codes emanated from the interview guide as a starting point for analysis. We then employed constant comparison and triangulation to identify central concepts.19,20 The initial stage of constant comparative analysis was done through coding by investigators (MSM and CIM). Line-by-line coding was individually performed by the investigators (MSM, CIM, and ARO) using the qualitative analysis software Dedoose. 21 Kappa scores on a random sample of codes showed >0.90 agreement between MSM and CIM. Relevant themes and concepts were developed inductively from these data. After analysis, authors agreed that the themes were saturated and no further semistructured interviews or focus group discussions were necessary to elucidate new ideas. We used basic descriptive analyses to describe the study sample. Quotes, edited minimally for clarity, are provided to add descriptive detail and highlight major themes.
Ethical Approvals
Written informed consent was obtained from all study participants, both caregivers and clinical providers, on enrollment to this study. This study was approved by the Institutional Review Board of Indiana University School of Medicine in Indianapolis, Indiana, and by the Institutional Research and Ethics Committee of Moi University School of Medicine and Moi Teaching and Referral Hospital in Eldoret, Kenya. The ethics committee at Moi University is registered with the US Office of Human Research Protections with its own Federalwide Assurances (FWA00003128).
Results
Twenty-five clinical providers and 67 caregivers of HIV-infected children participated in this study. Most providers were clinical officers (a mid-level provider) and female. A quarter of providers (7/25) indicated having training in child development, and over half of these (4/7) noted that this training was within the context of their general clinical education. Nearly 90% of caregivers were biological mothers of the HIV-infected children. Approximately 40% of caregivers did not work outside the home and fewer than half received education beyond primary school (Table 1).
Participant Demographics.
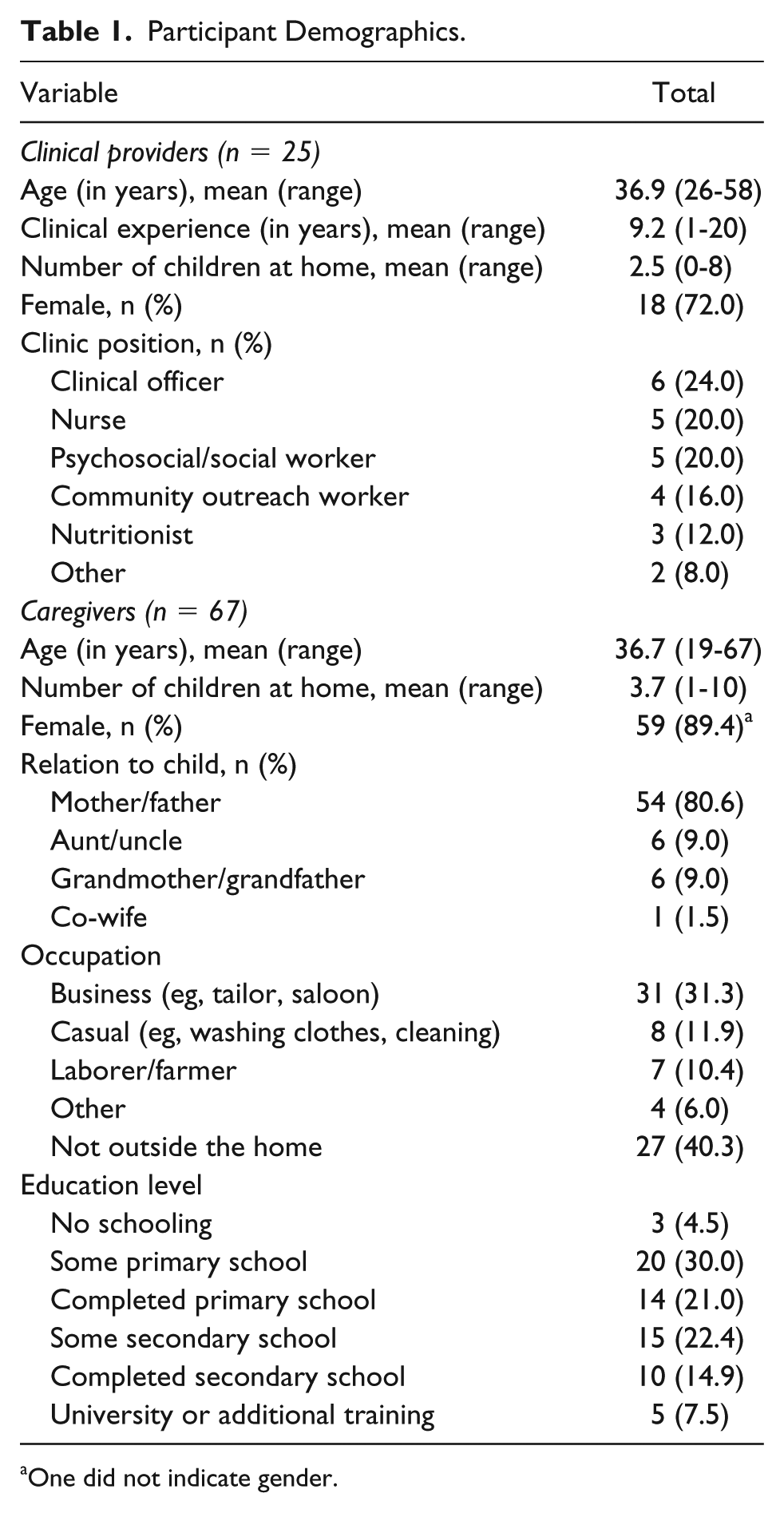
One did not indicate gender.
Within the framework of our interview guides, we highlighted general understanding of ECD, factors affecting development, additional considerations for children born to HIV-infected mothers, and identification and treatment of development delays. Themes within these categories are described.
General Understanding of Child Development
The general understanding of ECD differed between providers and caregivers. Most providers understood that ECD consists of physical, mental, and physiological development across age ranges. Providers often stated that a child is expected to do certain tasks at certain ages, some using the term “milestones” and others describing examples of milestones (eg, a child should be able to sit at 6 months).
In contrast, caregivers generally did not have rigid or concrete definitions of ECD. When asked what the term “development” meant to them, most focused on their child’s birth, as well as their physical growth and feeding practices, especially within the first 6 months of life.
Local Concepts of Development
Participants of this study represented 6 Kenyan tribes: Luhya, Kalenjin, Luo, Kikuyu, Bantu, and Kisii. Each of these ethnic groups has a local language, which is often the first language that they learn in life. When asked to describe the concept of “delays in development” in their local language, participants identified 37 different words or phrases. Approximately 46% (17/37) of these words literally translated to terms indicating physical growth (5/12 of providers’ words and 12/25 of caregivers’ words). The Luhya tribe was most represented, and 59% (11/19) of the words provided directly translated to physical growth. Other words provided by caregivers translated directly to either childbirth or witchcraft.
Determining Developmental Status
Age-specific milestones were the primary focus of nearly all providers when asked for indications of typical development. If a child achieved specific tasks, such as walking and talking, at the same time as their peers, providers perceived their development as normal. The providers described age ranges to convey when a milestone might be achieved. These age ranges were largely consistent with Western norms, although some small differences were noted. For example, many providers would be concerned if a child was not walking independently by 12 months. Less often, providers indicated the ability of a child to socialize at school and perform specific gender roles was an indication that a child was developing typically.
A few caregivers also compared a child’s skill with that of other same-aged children, but this was rarely described in comparison to that of the providers. Instead, caregivers often referred to crying at birth, the timing of tooth eruption, as well as a child’s weight, general size, energy level, and school performance as indications of typical development.
The ability to perform expected gender-specific chores was also commonly described by caregivers as a way to know a child is developing typically. As one caregiver noted: If it is a girl, she will wash the utensils. A boy will graze the cows, sheep, and goats. With that you will know that this child has grown to a certain level. But if you have gone somewhere else and you return to find beddings outside rained on, the chicken are still outside late in the evening, then you will know that this child is not developing or there is a problem somewhere.
Factors Affecting Development
The major factors affecting children’s development that emerged from both caregivers and providers were nutrition, home environment, illness, maternal factors and prenatal care, and poverty. Illustrative quotes are seen in Table 2.
Factors Affecting Development: Illustrative Quotes From Caregivers and Clinical Providers.

Nutrition
Both groups highlighted the importance of a balanced diet, not only ensuring that a child was getting enough food but also getting a variety of nutrients. Discussions with both groups revealed a clear connection between the nutrition a child received and their growth and development. Providers clearly described this connection, while caregivers tended to focus on the physical growth. Both groups discussed nutrition throughout childhood; however, caregivers more often focused on the first few months of a child’s life. Both groups frequently outlined the duration of time that mothers should exclusively breastfeed and when the child should be weaned.
Home Environment
Both caregivers and providers noted that neglected children had worse development than those children living in a loving home. Most caregivers stressed the importance of showing love for the child. Additionally, caregivers noted the impact that family dynamics had on a child’s development (eg, the negative impact of familial discord on children’s development).
Providers and caregivers also noted that neglect was a risk factor for delays, which generally occurred when children were left for hours without adult supervision. Both groups shared examples in their community when caregivers would leave their children at home by themselves. Some were “locked up” because they had delays and the caregivers did not want to take them into the community. Other children were left behind because the caregivers were laborers and the children were no longer small enough to take with them. One caregiver described a case where a mother would leave her toddler alone at home while she went out drinking alcohol. These examples were common cases highlighted during the discussions, with both providers and caregivers deeming them as instances of neglect, which may negatively affect child development.
Both groups also felt that discipline was a factor that affected child development. Some focused on the importance of being strict to ensure that their children behaved well. However, more often the degree of physical discipline was described. Both providers and caregivers noted that children’s development is negatively affected when they are beaten too often and too harshly. Rarely, violent sexual abuse, such as rape and its implications to physical development, were discussed.
Illness
Both groups discussed infectious diseases as affecting development. Providers generally described the illness itself (eg, tuberculosis, malaria, HIV, diarrhea, or pneumonia), especially when chronic in nature. Caregivers primarily focused on the prevention of infectious diseases, for example, by noting the importance of children receiving immunizations. They also described how a clean environment, including the “cleanliness of the body,” affects children’s development.
A focus on cleanliness also had the potential to negatively affect the developmental status of children. Caregivers frequently mentioned that individuals who worked as laborers often had to bring their infants with them to work. In these cases, they would be carrying them on their backs in order to keep them clean. In doing this for long hours during the day, it prevented the children from “being free,” and some caregivers indicated that this could be an additional cause of development delays.
Maternal Factors and Prenatal Care
Both providers and caregivers believed the earliest moments of a child’s life could determine their long-term development. Providers focused on maternal factors during pregnancy, citing impacts of nutrition, illness, stress, and drug abuse (typically alcohol). Providers also noted how higher maternal education could help improve children’s development, while stressors experienced during pregnancy could worsen children’s development. The importance of a mother delivering in a medical facility was a common discussion point among providers, and they noted the association of unattended delivery complications with poor developmental outcomes.
Caregivers also addressed the issue of prenatal care. However, their approach was generally more indirect. A child’s birthweight was of great importance when discussing their development. Additionally, caregivers noted the absence of crying at birth to be associated with poor developmental outcomes. A few caregivers identified maternal health conditions and prenatal exposures that could affect developing fetuses, including exposure to rubella and alcohol.
Gender
Almost all caregivers and providers indicated that young girls develop faster than boys. The majority of participants were unable to provide an explanation for this perception. A few providers cited their training as the source of this knowledge, while most others were confident of this fact but admitted they were unsure why this was the case.
Additionally, caregivers described that within particular Kenyan tribes, sons are preferred over daughters. The sons received more attention and resources than the daughters, which they indicated could negatively affect the development of young girls.
Poverty
Underlying much of the discussion of factors affecting child development was poverty. Both providers and caregivers cited examples of how poverty made it difficult for families to provide enough nutrition for their children. Poverty also led caregivers to work as laborers, spending long hours away from their children and often depriving them of a stimulating environment. For those laborers with children too young to walk, the children were often taken and carried on their caregiver’s back throughout the day. Poverty also made it more difficult to prevent illnesses and obtain timely treatment for children.
Cultural Beliefs and Developmental Delays
Both groups also indicated certain cultural beliefs, such as curses or the “evil eye,” as other potential reasons for development delays. However, providers mostly indicated that these ideas existed within the community and did not necessarily contribute to development. Providers described stories of children with severe delays being locked in the house, and one added, “It goes even as far as others being thrown away.”
Caregivers did not frequently describe witchcraft as a source of delays, although some caregivers stated that it was “God’s will” when a child would not develop typically. These caregivers often sought treatment for their children at the church and forwent seeking medical care. Caregivers also described cultural practices within their tribe that would be attempted when a child was not developing typically.
Additional Considerations for Children Born to HIV-Infected Mothers
Adherence to antiretroviral treatment was the overarching factor affecting development in children born to HIV-infected mothers. Both providers and caregivers believed if HIV-infected mothers were adherent to their antiretroviral treatment during pregnancy, and if an HIV-infected child was adherent with their antiretroviral treatment, that the child’s development would be similar to his/her peers. Additionally, those children who were HIV-exposed but uninfected were thought to be the same developmentally as their nonexposed peers. However, if HIV-infected children came into care late or were not taking antiretroviral treatment, then their development was believed to be worse than their peers.
Providers focused on the importance of prenatal care for HIV-infected mothers, while caregivers stressed that HIV-infected children should be treated equally to those who are uninfected. Some caregivers noted that HIV-infected children should receive additional care and consideration, such as more nutritious food. Additionally, one caregiver noted that for her HIV-infected child, she asked the teacher to not beat him to the point of bloodshed, to avoid putting the other children at risk of HIV exposure (Table 3).
Additional Illustrative Quotes From Caregivers and Clinical Providers.

Identification and Treatment of Children With Development Delays
Providers noted that caregivers’ reluctance to seek care was a critical barrier to identifying children with delays. Both caregivers and providers described the stigma that families feel for having a child with delays. Additionally, providers believed that some families do not seek care, because the delays did not seem to make the child uncomfortable (Table 3).
Half (12/24) of providers were unable to identify a location where developmental screening takes place. Some (5/24) indicated that Maternal-Child Health clinics, where young children receive weight checks and immunizations, performed developmental screening. Five providers indicated that they screened at their clinic, either by asking general questions if they believed a child was delayed or by monitoring physical growth only. Only one provider noted the existence of developmental screening questions on intake forms for patients attending the clinic.
Half (13/24) of providers were aware of physical and/or occupational therapy options within their communities. Some (6/24) indicated that children requiring intervention should be referred to the local hospital. Two providers identified a local school with the capabilities to care for children with development delays. The remainder knew of no treatment options for delays in their communities.
Most (19/23) indicated that they would be willing to screen for delays within their clinics. Two indicated that another individual within their clinic was more appropriate to perform the screening, and two others noted that it would be a challenge to add screening to their current workload.
Discussion
Among this sample of clinical providers and caregivers of HIV-infected children in Kenya, we found differences in perspectives of ECD and understanding of factors related to development delays. Most notably, providers understood child development within the context of milestones and described the factors affecting development in concrete terms, while caregivers generally gave more indirect descriptions of the factors described. Physical growth was almost inseparable from child development for caregivers. Both providers and caregivers generally believed when HIV-infected pregnant mothers and children were adherent to their antiretroviral treatment, the ECD of those children were similar to HIV-exposed, uninfected and unexposed children. While half of providers were unable to identify if and where developmental screening took place, the majority were willing to screen for it within their clinical role.
The clinical providers’ conceptualization of ECD as developmental milestones is consistent with most Western theories of ECD development. The first formalization of developmental milestones is often attributed to Arnold Gesell’s work studying child development and his classification by age of when certain abilities and skills would emerge. 22 This created the foundation for the construct of formal developmental milestones, which subsequently enabled clinicians and psychometric assessment developers to determine when a child had developmental delays. The issue with Gesell’s study population, as well as the populations used to norm most standardized developmental assessments, is that they consist of children living in Western, industrialized countries. 22 This may complicate the comparison of those milestone standards when used cross-culturally. In our study, many providers believed that children should be walking before 12 months of age. This is in contrast with the American Academy of Pediatrics’ position that the average age of walking is 12 months, with many neurologically typical children walking between 12 and 15 months. 23 The data supporting this position were from a study that reported the mean age of walking for Caucasian infants at 12.0 months, while the mean age was 10.9 months for African American infants. 24 In fact, this article concluded that African American infants tended to attain all gross motor milestones at an earlier age than Caucasian infants. 24 It is plausible that Kenyan children may develop at a rate that is similar to that of African Americans. Additionally, it was been shown that when a culture highly values certain skills or abilities, caregivers’ interactions with their children help promote those activities, such as stretches and postural manipulations for the promotion of walking. 25 When determining appropriate developmental milestones in Kenya, it is important to understand the typical trajectory of children living in this setting. Developmental assessments, such as the Kilifi Developmental Inventory 26 in Kenya and Malawi Developmental Assessment Tool, 27 have used local populations to develop and norm assessments for the cultural context in which they are used. While this is a resource- and time-intensive process, it is critically important in helping us understand how ECD milestones might differ cross-culturally.
While the providers were able to describe the full range of development within young children, caregivers’ conceptualization of ECD heavily focused on physical growth, with motor development, behavior, and occasionally language also being discussed. Most conceptual models within Western context include cognition, language, social-emotional, and sensorimotor development. 28 The caregivers’ focus on more concrete, external developmental domains may be the result of their limited education on ECD. Additionally, while this study did not include a robust linguistic analysis, it was noted that many local languages used terms for physical growth to describe child development. This could potentially indicate that other domains of development may not be as easily expressed and conceptualized within their local language and culture as physical growth is, although this hypothesis would require further analysis. For interventions addressing development delays to be effective, it is important for caregivers to understand the full spectrum of domains involved with ECD and the impact that delays have on their children’s long-term growth. While more exploration is needed to determine the developmental domains of interest when promoting ECD in this context, having physical growth and ECD linked in the minds of caregivers may be beneficial. In fact, the World Health Organization has described the connection between physical health and psychosocial development as a “critical link.” 29 Many of the factors that cause poor health and growth also affect development, such a stunting or low height-for-age Z-scores due to malnutrition. 30 Conversely, factors that cause poor development (eg, unstimulating environment) also cause poor health. By expanding education on the importance of nutrition, infection control, and immunizations, we are not only promoting optimal growth for children, but we can also educate families on the importance of ECD and risk reduction of development delays.
Caregivers highlighted the importance of providing children with loving homes. However, they also discussed physical abuse with distinct normalcy, which inferred that physical abuse and love for a child are not mutually exclusive in Kenyan culture. Despite a 2001 Kenyan law protecting children from physical and psychological abuse, corporal punishment is still commonly used on children, even within schools.31,32 Caregivers were either unaware of this law or understood that it was not enforced whenever they discussed teachers beating children at school. In a study of African countries in 2005-2006, 43% of children experienced severe physical abuse in the prior month, while 83% experienced psychological abuse. 33 In our study, caregivers noted that the severity and frequency of “beatings” should be monitored, as this was perceived to affect child development. Physical punishment is associated with a range of mental health problems in children, as well as slower cognitive development and lower academic achievement.20,34 Early childhood programs in these settings would benefit from educating caregivers, parents, and teachers on the importance of reducing or eliminating physical punishment and psychological abuse for children in order to maximize their children’s development.
Children born to HIV-infected mothers experience multiple social risk factors that may negatively affect their behavior and development. The social stigma of HIV can create additional stressors in both caregivers and their children.9,35 Children living with HIV-infected parents are more likely to experience mental health difficulties and abuse that persists over time.36-38 Depression in HIV-infected caregivers is also associated with increased internalizing and externalizing behaviors in the children living in their households. 39 Efforts for promoting ECD and reducing child abuse should provide support and education to help caregivers address children’s externalizing behaviors and reduce HIV stigma in these settings.
The degree of social stimulation is also a factor affecting child development. Providers and caregivers described cases of young children being left at home for long periods of time without supervision. Within Kenyan culture, children are preferably left under the care of a neighbor, house help, or family member; however, siblings are commonly the ones responsible for caring for each other at home. The phenomenon of children being left at home without supervision is not uncommon in low-resourced settings, and it is often necessary due to economic restraints and lack of close family support. A survey performed in low-resourced settings found that 33% of single-parent homes and 22% of dual-parent homes had left their children alone at home.40,41 In 66% of these households, the children had suffered accidents or emergencies; in 35% of the cases, the children were reported to have suffered from developmental or behavioral problems.40,41 While this may be unavoidable in certain settings, programs looking to support families in a holistic manner should consider appropriate options for child care while adults are performing economic activities.
While historically there is no clear evidence of significant differences in ECD between the genders,42,43 nearly all study participants believed that females developed more quickly than males. Given the perception of both caregivers and clinical providers that certain tribes continue to prefer boys over girls, one would assume that boys are provided with more resources and opportunities for stimulation during the early periods of child development. However, this assumption is at odds with their belief that females develop more quickly than males. None of the participants were able to give an etiology to the difference, but this perception may warrant consideration by public health officials and epidemiologists. Some studies have found associations between low cognitive, motor, and social-emotional scores and the male gender in low- and middle-income countries.30,44 Future research is needed to measure the strength of this association and, if true, determine possible etiologies for this finding and how perceptions of a preferred gender might affect these results.
The study participants were specifically recruited as individuals closely involved with the care of HIV-infected infants and children. In general, both providers and caregivers believed that if an HIV-infected mother received appropriate antiretroviral treatment during pregnancy or if an HIV-infected child was adherent to antiretroviral treatment, then ECD would be unaffected. Studies have shown that even when young HIV-infected children are on antiretroviral treatment, they have worse developmental outcomes compared with their uninfected peers.11,45,46 The evidence is less clear for HIV-exposed but uninfected children; however, a recent meta-analysis found that these children had lower cognitive and motor scores compared with unexposed children. 11 In each of these studies, the developmental status was measured by neuropsychological testing. Therefore, the presentation of these delays may not be overtly observable by family and community members in otherwise healthy HIV-infected and HIV-exposed children. It could be hypothesized that HIV-infected children who are not adherent to antiretroviral treatment have significantly more risk factors for development delays, such as malnutrition and recurrent illness, and their presentation of delays may be more severe and thus observable. More research is needed to more clearly delineate these findings.
Differences between providers’ and caregivers’ knowledge of ECD were likely due to educational achievement. While most of the providers did not have specific training in ECD, nearly all of them received training after secondary school. Less than 10% of caregivers had received any training beyond secondary school. This may have influenced the providers’ increased understanding of milestones and the impact of prenatal factors and recurrent illness on development, whereas caregivers primarily focused on physical growth, cleanliness, and events within a baby’s first few months of life. Future efforts at improving ECD in this setting must focus on educating caregivers about ECD, to help raise awareness of this issue and enable caregivers to advocate for their children.
Within this setting, screening for development delays appeared limited to those with obvious delays on exam. Only one provider knew about the developmental screening questions on the required forms completed on every new patient. Due to numerous developmental risk factors for children in this setting, routine screening for all children is critical for detecting development delays. Providers in Western settings who did not perform routine developmental screening also fail to identify children with delays. 47 Furthermore, although many providers were aware of physical and occupational therapists in their village, few knew of other ECD resources (eg, schools accepting children with special needs). This lack of awareness is in discordance with the Kenyan guidelines for ECD. 4 Kenya’s government increased grants to help subsidize the cost of ECD programs for those with the greatest financial need.48,49 Theoretically, this action should have increased access to these services. However, if providers are unaware of these resources and no one is routinely screening and diagnosing children with delays, these children are at risk for not benefiting from these policy and funding changes.
A potential limitation of this study design is its western Kenyan setting, which has a prominence of specific tribes, and it may not be applicable to all of Kenya or to HIV-exposed children. Efforts were made to draw on perspectives from clinics with varying pediatric population sizes, levels of urbanization, and ethnic diversity. However, cultural views will likely differ across different cultures and settings.
By looking at provider and caregiver perspectives on ECD, we are taking the first step in understanding the constructs of ECD held by communities in Kenya, especially those affected by HIV. Few studies have looked at sub-Saharan African caregiver and health provider perspectives on ECD, and they primarily focused on creating developmental assessment tools or exploring developmental outcome measures.50,51 Our study adds further insights by allowing participants to describe their own understanding of development, factors affecting development, differences with HIV-infected populations, and perceptions of screening and intervention services within their community. These perspectives help guide us in educating and engaging the village elders and community members to promote ECD, reduce development delays, and implement a screening and referral system in the future.
Footnotes
Acknowledgements
The authors would like to thank the study participants for their time and invaluable insights.
Author Contributions
MSM: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EO: Contributed to conception and design; contributed to acquisition and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CIM: Contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ARO: Contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ERC: Contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SOA: Contributed to conception; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RCV: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Indiana Center for AIDS Research (Principal Investigator: Megan S. McHenry). Dr McHenry was also supported by the Morris Green Physician Scientist Development Program at Indiana University.