
Abstract
This case report describes an adolescent with pancreatic insufficient cystic fibrosis, malnutrition, and cystic fibrosis–related diabetes found to have a loss in height at a routine outpatient clinic visit. He was subsequently admitted to the hospital for treatment of a pulmonary exacerbation and was found to have multiple, nontraumatic vertebral compression fractures. This report emphasizes the importance of routine review of growth charts and aggressive treatment of vitamin deficiencies and malnutrition in people with cystic fibrosis.
Keywords
Case Report
A 19-year-old young man with cystic fibrosis (CF; F508del/F508del), exocrine pancreatic insufficiency, CF-related diabetes (CFRD), chronic sinusitis, moderate malnutrition requiring gastrostomy tube feeds, fat-soluble vitamin deficiency, and osteopenia was hospitalized for inpatient treatment of a CF pulmonary exacerbation and a weight loss of 15 pounds since starting college 3 months prior. His forced expiratory volume in 1 second (FEV1) on admission had declined from a baseline of 90% predicted to 65% predicted. His weight had declined to 134 pounds (body mass index [BMI] = 22.2 kg/m2), and his hemoglobin A1C was 7.8% on admission. Of note, he had been taking lumacaftor/ivacaftor, a medication approved by the Federal Drug Administration in 2015, for approximately 18 months. Lumacaftor/ivacaftor is the first medication approved to treat the genetic defect in people with CF who carry 2 copies of the CF transmembrane conductance regulator (CFTR) mutation F508del. On admission, a review of his growth chart revealed a height loss of 8.5 cm over the previous 5 months (Figure 1). This had previously been identified during an outpatient CF clinic visit, at which time he did not endorse symptoms of back pain and was largely thought to be secondary to variability in height measurement by clinic staff. A dual energy X-ray absorption (DEXA) scan 1 month prior to admission was significant for osteopenia (lumbar spine Z-score = −2.1, total body Z-score = −1.4) but did not show evidence of a vertebral compression fracture. The patient reported no limitation in activity or movement.
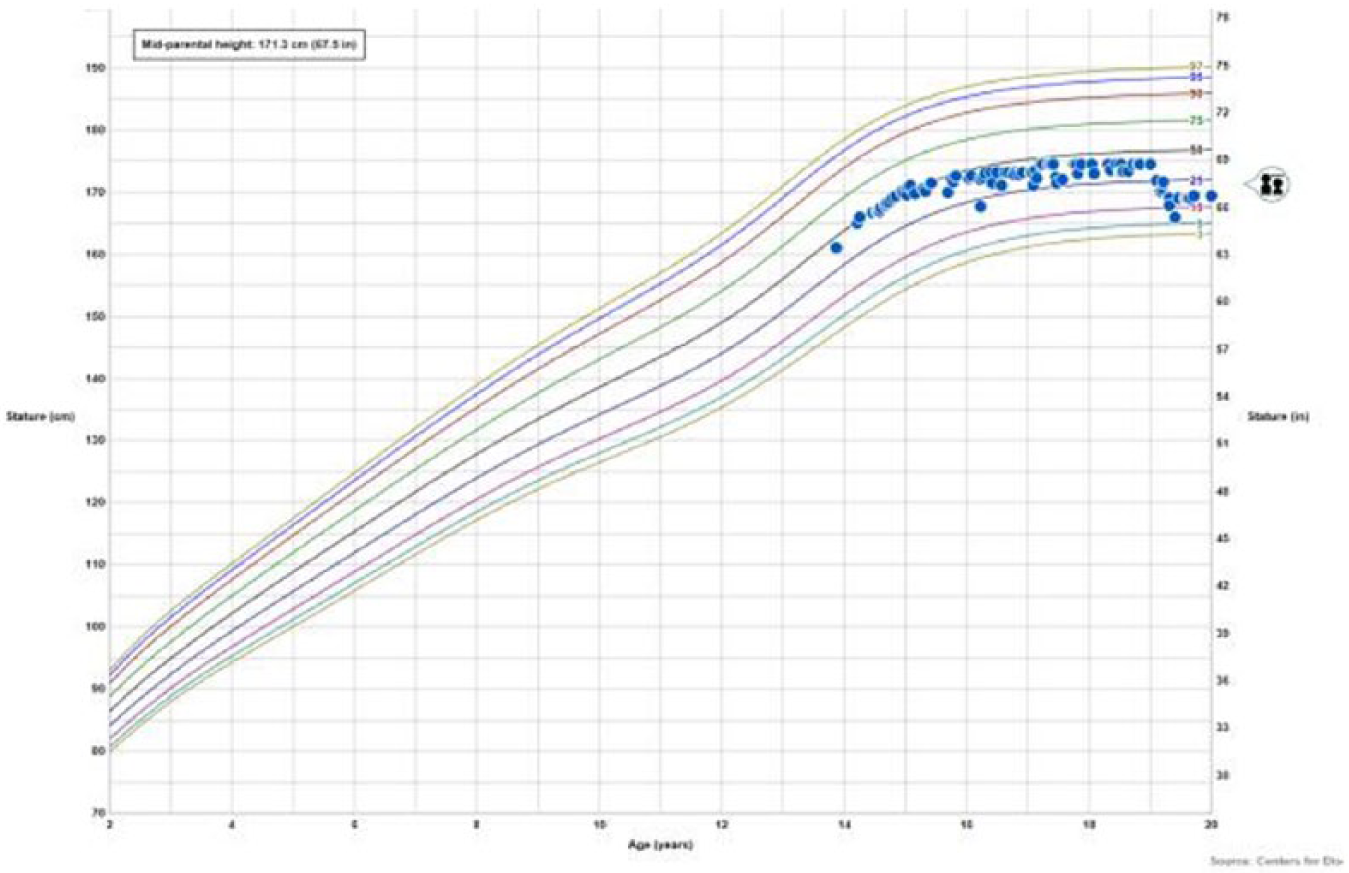
Growth chart showing abrupt, significant loss in height.
Hospital Course
The patient was admitted to the hospital and started on treatment for a CF pulmonary exacerbation, which included nebulized mucolytic therapy with high-frequency chest wall oscillation therapy 4 times daily, intravenous antibiotics, pancreatic enzyme replacement therapy, fat-soluble vitamin supplementation, and insulin therapy for his CFRD. His nightly gastrostomy tube feeds for supplemental nutrition were continued. He was continued on his lumacaftor/ivacaftor CFTR modulating therapy. On further questioning, the patient did endorse mild intermittent back pain over the previous 6 months, which he had attributed to sleeping on a couch. He had no history of trauma. His musculoskeletal physical examination remained normal, aside from the loss in height, with no neurologic signs or focal spinal tenderness. Given the observed loss in height of unclear etiology, imaging studies were performed to better assess his spine. A lumbar spine X-ray demonstrated a superior endplate fracture of L1 and a chest computed tomography scan obtained for primary pulmonary concerns revealed the incidental finding of significant height loss of multiple mid-thoracic vertebrae. A follow-up total spine magnetic resonance image was obtained and showed evidence of chronic compression fractures at the level of T5 through L1 (Figure 2). None of the fractures were displaced and there was no evidence of compression of neurologic structures.

Magnetic resonance image demonstrating chronic T5-L1 compression fractures.
Given the unexpected finding of multiple spinal compression fractures, pediatric neurosurgical consultation was requested. They recommended monitoring with serial spine X-rays. No bracing or surgical correction was indicated. Laboratory studies showed low levels of fat-soluble vitamins (vitamin A level of 0.34 mmol/L, 25-OH vitamin D3 level of 26 µg/L, vitamin E level 3.7 µg/mL, and international normalized ratio of 1.23) and normal calcium, ionized calcium, alkaline phosphatase, and parathyroid hormone levels. In consultation with Pediatric Endocrinology, the pediatric CF dietitian, and the pediatric CF pharmacist, aggressive treatment for the patient’s osteopenia was recommended and initiated. Given previous concerns of adherence to chronic therapies, he was given a single, oral high-dose stoss vitamin D3 replacement therapy (500 000 IU) followed by the initiation of a 1-year course of intravenous pamidronate. 1
Final Diagnoses
(1) Nontraumatic compression fractures of T5 through L1, (2) fat-soluble vitamin deficiency, (3) CF pulmonary exacerbation, and (4) cystic fibrosis.
Discussion
Osteopenia and osteoporosis are well-known complications of CF, particularly in older patients with end-stage disease. The etiology of osteopenia in CF is complex and incompletely understood. 2 Several studies have correlated poor nutrition, malabsorption, vitamin deficiencies, systemic glucocorticoid use, male gender, presence of CFRD and chronic infection, and inflammation with decreased bone mineral density (BMD).2-5 A study of adolescents and adults with CF found that low BMD Z-scores were also predicted by poor lung function, or low FEV1. 4
Due to the progressive nature of bone loss, fractures resulting from osteopenia are less common in pediatric patients and are often due to at least minimal trauma. Fracture rates of 34% to 53% in adolescent and young adult CF populations are reported, with only one report of a spontaneous fracture. 6 Few studies report the age at which fractures occur, but a recent German study of 43 adolescent and young adult CF patients found that 20.9% of these patients had at least one fracture occurring before the age of 10 years and 13.9% before the age of 5 years. 6 Although fractures do occur in young CF populations, it is especially unusual to see nontraumatic fractures in pediatric patients. In the study previously mentioned, only 1 of 43 patients had a spontaneous fracture and it was of a non-axial bone. 6 No spontaneous vertebral fractures were reported. 6 This patient’s presentation with multiple nontraumatic vertebral compression fractures is both concerning and unique. To our knowledge, the only other reported case of spontaneous vertebral compression fractures in a pediatric CF patient occurred at the time of systemic glucocorticoid therapy. 7 Our patient has many risk factors for osteopenia, including malnutrition, malabsorption, vitamin D deficiency, male gender, poorly controlled CFRD, chronic infection and inflammation, and a low FEV1 (65% predicted on admission). However, he was young and had not received treatment with systemic glucocorticoids for the past year. With no reported pain or known trauma and a recent DEXA showing no evidence of fracture, multiple vertebral compression fractures were an unexpected and perplexing finding.
Although this patient had numerous risk factors for fractures, given the infrequent nature of fractures in pediatric CF patients in the absence of trauma, we searched for additional potential contributing factors. Lumacaftor/ivacaftor therapy was initiated in our patient approximately 18 months prior to his presentation. With the relatively recent widespread clinical use of lumacaftor/ivacaftor given its Federal Drug Administration approval in 2015, it is important to consider the possibility of this medication having an impact on bone health. There is a growing body of evidence suggesting a role of CFTR in bone metabolism, possibly by way of osteoblast function. 3 Although lumacaftor/ivacaftor improves the functionality of the CFTR, it is possible that bone metabolism could be adversely affected by altering CFTR function. Although there is no published mechanistic link between lumacaftor/ivacaftor use and fractures, this warrants further investigation and vigilance, as we gain more experience in the long-term use of this medication in both the pediatric and adult CF population.
The early identification of bone loss leading to fractures is of great importance in the care of CF patients, as fractures can limit quality of life and even lead to pain that limits cough and sputum clearance. The current standard of care for monitoring bone loss in pediatric CF patients includes surveillance with DEXA scans measuring BMD of the total body and lumbar spine starting at age 8 to 10 years, with scans repeated every 1 to 5 years based on the patient’s BMD Z-scores. 3 However, low Z-scores alone have poor positive predictive value for patients who will go on to have multiple fractures. 6 Rather, DEXA scans may be more useful in identifying a group of CF patients with low fracture risk. 6 Additionally, DEXA scan 1 month prior to our patient’s admission did show osteopenia, but failed to show any fractures. Based on these findings, it may be prudent to reevaluate optimal screening methods for fractures in pediatric CF patients with risk factors for osteopenia. Pediatricians involved in primary or hospital care of CF patients should be knowledgeable about the risk factors for osteopenia and vigilant in monitoring not only standard DEXA screens but also growth curves and subtle symptoms of fracture. Unexpected height loss in a pediatric CF patient is especially concerning and warrants early escalation to further imaging beyond the DEXA scan.
Conclusion
We present the case of a 19-year-old adolescent with CF who was found to have multiple, relatively asymptomatic, nontraumatic vertebral compression fractures. This case highlights the importance of considering the possibility of occult fractures in pediatric patients and the need for vigilant height monitoring, as well as the consideration of early imaging in patients with multiple risk factors for osteopenia.
Footnotes
Acknowledgements
The authors wish to thank this CF patient and family.
Author Contributions
AS: Contributed to conception and design; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JM: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RE: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CTT: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TAL: Contributed to conception and design; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.