
Abstract

Introduction
Knowledge on uterine anomalies is important as they have great impact on women’s quality of life. Prevalence of common uterine anomalies is reported to be 7% to 10% in the general female population. 1 However, complex urogenital malformations are often missed and incorrectly diagnosed and fail to get timely treatment. Herlyn-Werner-Wunderlich (HWW) syndrome is a rare and underdiagnosed developmental anomaly of female urogenital tract and includes finding of uterus didelphys and obstructed hemivagina and ipsilateral renal agenesis (OHVIRA).2,3 It is a unique entity resulting from embryological arrest of Müllerian and mesonephric ducts at 8 weeks of gestation. 4 The incidence reported in the general population is 0.1% to 3.8%, with two thirds of patients with duplication of uterus having complete vaginal septum. 5 However, only few variants of OHVIRA are known, which includes septate uterus and ipsilateral renal anomalies. 6 A patient generally presents after menarche with nonspecific symptoms and diagnosis is often delayed till acute complications develop. 2 It is often associated with infertility, recurrent pregnancy loss, and adverse pregnancy outcomes. 1 Diagnosis is challenging and critical and requires use of diagnostic imaging to guide treatment, alleviate acute complications, and restore fertility. 3 High level of clinical suspicion is the key to timely diagnose and avoid complications.
Case Report
A 16-year-old-girl presented in the emergency department with increasing right lower quadrant and lower pelvic pain for 2 days. The patient had menarche at the age of 14 years with regular menstrual cycles. However, for the past 2 months she was experiencing cyclical abdominal pain. General physical examination was unremarkable. Abdominal examination showed a tender mass in the right lower quadrant extending to pelvis, which persisted even after voiding. Abdominal radiograph showed superior displacement of bowel loops (Figure 1). A provisional diagnosis of an extremely full urinary bladder or an abdominopelvic mass was made. Further evaluation with ultrasound was recommended. Transabdominal pelvic ultrasound distended endometrial and endocervical cavities filled with complex fluid with low level internal echoes—a provisional diagnosis of hematometra with hematocolpos was made (Figure 2). Uterus didelphys could not be appreciated on ultrasound as left was not seen on ultrasound likely due to compression by enlarged right horn. Additionally, the right kidney was absent (Figure 2). Due to complexity of clinical situation a magnetic resonance imaging (MRI) pelvis was recommended. MRI pelvis demonstrated uterus didelphys, right cervical atresia resulting in distended right endometrial and right endocervical cavities, and a compressed left uterine horn (Figure 3). These findings support patient’s normal regular menstruation since menarche from communicating left uterine horn until 2 months back when she started having dysmenorrhea. The patient underwent utero-vaginal canalization with right hemi-hysterectomy and drainage of the hematometra. She had uneventful postoperative stay with resolution of symptoms and resumption of normal menstruation.

A 16-year-old-female presented with severe right lower quadrant and right lower pelvic pain. Supine abdominal radiograph showing paucity of bowel loops in the right lower quadrant, with associated displacement of the small and large bowel loops superiorly.
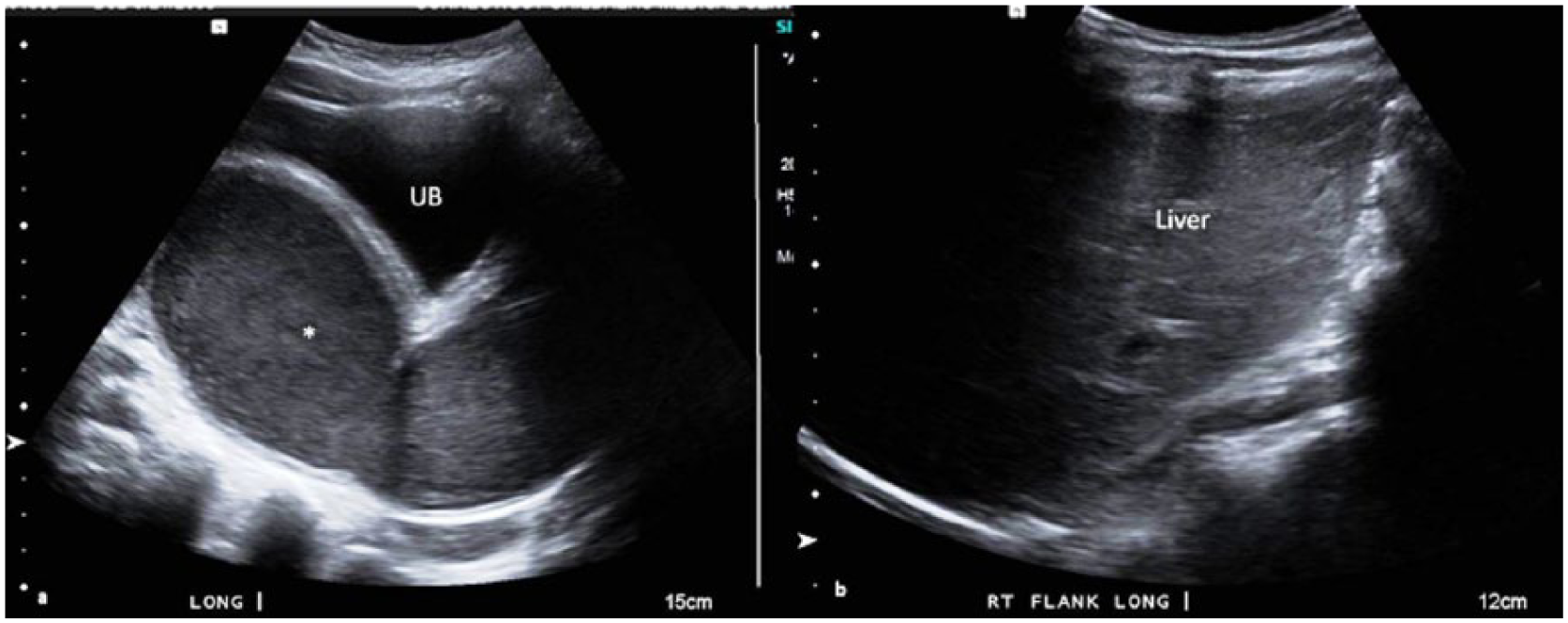
Transabdominal ultrasound. Midsagittal image of pelvis demonstrates (a) distended endometrial and endocervical cavities filled with complex fluid with low level internal echoes (*), compatible with hematometra and hematocolpos. Left horn of uterus was not appreciated on ultrasound, likely due to compression. Longitudinal image through the right flank (b) demonstrates nonvisualization of the right kidney.

Magnetic resonance imaging of pelvis demonstrates uterus didelphys with unilateral cervical atresia just above the external-os/noncommunicating cervix. Coronal T2WI with fat saturation (a) demonstrates unilateral (right) cervical atresia resulting in moderately distended cervix filled with T2 intermediate hyperintense fluid suggestive of blood (*). Axial fat sat T2WI (b) demonstrates blood filled distended lower uterine segment and cervix (*). The left horn of uterus didelphys is compressed by distended right horn (green arrows). UB, urinary bladder; FF, free fluid in cul-de-sac.
Discussion
The OHVIRA syndrome is included in class III of the American Fertility Society classification (Table 1) of congenital uterine anomalies and often consists of uterine duplication, though septate uterus (Class V American Fertility Society classification) has been rarely associated.6,7 Ipsilateral renal agenesis remains the most common associated urological anomaly though multicystic dysplastic kidney, renal duplication kidneys, rectovesical bands, or crossed fused ectopia have also been reported in the literature. 8
American Fertility Society Classification of Female Genital Anomalies. 7

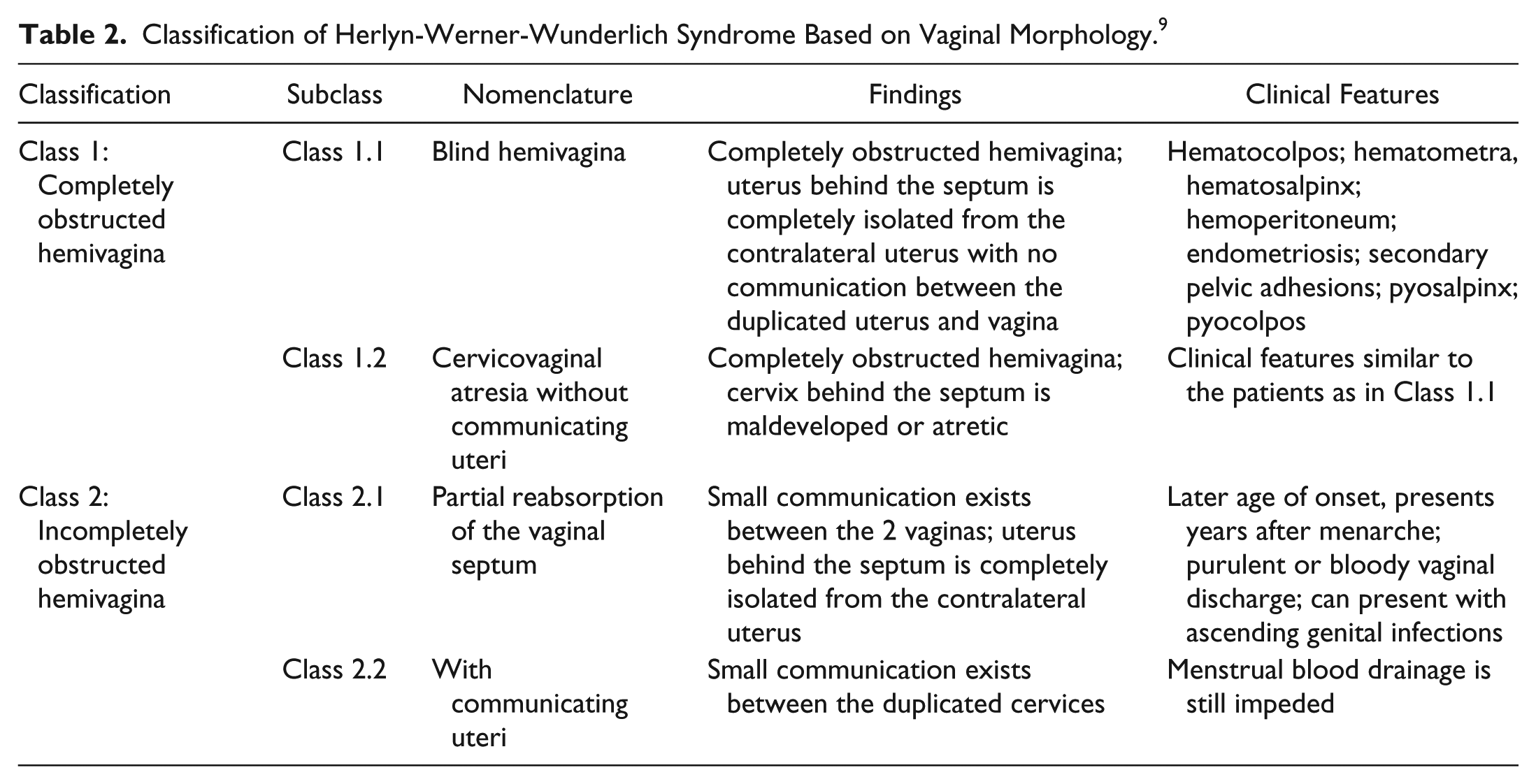
Recently, HWW syndrome has been classified on the basis of the morphology of vagina (Table 2). 9 Class 1 consists of completely obstructed hemivagina with Class 1.1 including blind hemivagina and Class 1.2 including cervicovaginal atresia without communicating uteri. Our case possibly can represent variant of Class 1.2 with didelphus uterus and unilateral cervical atresia.
Classification of Herlyn-Werner-Wunderlich Syndrome Based on Vaginal Morphology. 9
The etiopathogenesis of this spectrum of uterine anomalies remain unknown, though genetic and environmental factors are known to influence embryological development. Hox gene expression controlled by Wnt signaling pathway is known as regulators of uterine morphology have been implicated in genital organogenesis; however, no specific gene mutation responsible for defects is known so far. 10 According to the conventional theory of urogenital development, vagina develops partly from Müllerian duct and partly from urogenital sinus. 11 However, classical theory fails to explain complex female urogenital anomalies and accompanying renal anomalies. Recently, Acien theory has gained momentum and suggests that entire vagina is derived from mesonephric duct except vaginal cells, which are derived from Müllerian tubercle.1,12 Wolffian duct is located on both sides of the Müllerian duct and plays an important role in guiding fusion or resorption of wall between the Müllerian ducts. Ureteral bud arises from opening in urogenital sinus of Wolffian duct and any disruption in the development of these ducts can result in renal, uterine, and vaginal anomalies.
This syndrome may remain undiagnosed and asymptomatic during early childhood. Presence of a normal external genitalia can often mask internal urogenital anomalies. Rarely, in the neonatal period, patients can present with protruding vaginal mass due to distended hemivagina under the influence of maternal estrogen, which regresses after cessation of hormonal influence. 13 Often patients seek medical attention for menstrual disorders after the onset of menarche. The most common clinical presentation in postpubertal females is cyclical pelvic pain. However, presentation may vary and patients may present acutely with fever, pelvic abscess, pyohematocolpos, pyosalpinx, peritonitis, urinary tract obstruction, or ischiorectal fossa swelling or chronically with primary infertility, endometriosis, pelvic adhesions, or recurrent pregnancy loss.2,3 Rarely, adenocarcinoma of the obstructed side of the uterine cervix and clear cell carcinoma of the obstructed portion of the vagina are also noted. 2 Sometimes a patient continues to have normal menstruation and obstructive symptoms, which are often delayed. Our patient possibly had variant of Type 1.2 HWW syndrome with cervical atresia of one side and had normal menstrual cycles for 2 years before presenting. It needs to be emphasized that dysmenorrhea in young postpubertal females should not be taken lightly as it could point to underlying congenital anomalies. Many times, physician prescribes nonsteroidal anti-inflammatory drugs and oral contraceptive pills for presumed primary dysmenorrhea, which suppresses menstruation further delaying the diagnosis.
Diagnostic imaging plays an important role in diagnosing this rare developmental anomaly. Initial workup consists of ultrasonography, which can help diagnose genitourinary anomalies. Sonographic features include uterine anomalies (didelphic/bicornuate uterus), hematometra, hematocolpos, pelvic fluid collection (often hemoperitoneum), vaginal septum, and ipsilateral renal agenesis with compensatory hypertrophy of the contralateral kidney. 3 However, visualization of vaginal septum is often difficult and requires MRI for better anatomical delineation. 3 Laparoscopy remains the gold standard for diagnosis, though it may not be required all the time if diagnosis is obvious on history, examination, and initial imaging. It is often required to diagnose and treat the associated complications like endometriosis, adhesions, pelvic inflammation, and for fertility restoring procedures. 14
The treatment for OHVIRA syndrome targets at avoiding complications like hematocolpos and hematometra and restoring functionality of genital system to help achieve fertility potential. Surgery is the modality of choice and involves resection of vaginal septum to relieve the obstruction especially for Types 1.1, 2.1, and 2.2.8,11 However, Type 1.2 associated with cervicovaginal atresia is often difficult to treat and surgical interventions like utero-vaginal canalization with drainage of uterus through hysterectomy or partial hysterectomy have been described. 15 Utero-vaginal canalization is recently gaining momentum, with low risk of postoperative complications and normal menstrual and fertility outcomes. However, fertility may be affected if a patient had endometriosis before presentation, postoperative adhesions, restenosis of new cervix, or changes in cervical microenvironment. Surgical resection of the noncommunicating horn of uterus has been suggested to avoid complications of ectopic pregnancies and endometriosis. 15 As our case is a variant of Type 1.2, and being aware of preoperative diagnosis of cervical atresia, surgical resection of right uterine horn was discussed; however, family refused resection and utero-vaginal canalization was done with aim to drain the collection and to make drainage pathway to avoid further collection. Though risk of cervical restenosis and future endometriosis if obstruction develops was again explained. Extensive counselling was done regarding need for close follow-up and possible surgical resection of noncommunicating right horn if restenosis occurs.
Conclusion
Variants of OHVIRA syndrome are one of the less known congenital urogenital anomalies, diagnosis of which is often missed and delayed until complication arises. Delay in diagnosis is due to lack of awareness and understanding of this complex developmental anomaly. It is therefore imperative for radiologists, gynecologists, and pediatricians to familiarize themselves with the complex clinical spectrum, complications, diagnostic keys, and available treatment to catch the diagnosis at the earliest and prevent associated morbidity.
Footnotes
Author Contributions
NG: Contributed to conception; contributed to analysis and interpretation; critically revised manuscript.
DG: Contributed to design; contributed to acquisition; drafted manuscript.
SG: Contributed to acquisition; drafted manuscript.
PG: Contributed to analysis; drafted manuscript.
SL: Contributed to analysis; critically revised manuscript.
YK: Contributed to analysis and interpretation; critically revised manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.