
Abstract
Objective. The purpose of this study is to describe the range and frequency of cutaneous lumbosacral and coccygeal findings encountered during the newborn examination in a population of apparently healthy babies, to determine if the prevalence of these findings is associated with race/ethnicity, and to report the frequency of co-occurrence of low-risk cutaneous findings. Methods. Lumbosacral physical findings of 1121 infants were documented on well newborns at least 35 weeks or greater gestational age under the authors’ care. The overall frequency of each physical finding was tabulated in addition to determining whether frequencies varied by race/ethnicity. Co-occurrence of the most common physical findings was also examined. Results. Of 1096 infants included in the study, 24.8% had deviated or duplicated gluteal creases, 15.6% had dimples, and 24.7% had lumbosacral and/or coccygeal hairiness. All racial/ethnic groups had double to quadruple the risk of lumbosacral hair when compared with Caucasians. A total of 44.1% of study infants had lumbosacral/coccygeal slate-grey patches, which were least common in Caucasians. Seven infants had coccygeal skin tags, and 14 infants had lumbosacral vascular macules. Thirty-one percent had more than 1 cutaneous lumbosacral finding present, 24.8% had 2 findings, and 6.2% had 3 or more findings. Conclusion. Coccygeal dimples, increased lumbosacral and/or coccygeal hair, deviations and/or duplications of the gluteal crease, and lumbosacral slate-grey patches are common in healthy newborns and vary by race/ethnicity. Eleven percent of study infants had 2 or more low-risk cutaneous findings excluding slate-grey patches. Distinction between low-risk and common versus high-risk findings is important when deciding which patients need further evaluation.
Background
The association between cutaneous physical findings in the lumbosacral area and the presence of occult spinal dysraphism (OSD) has been well documented. Since early recognition and appropriate management of occult dysraphism can prevent irreversible neurologic damage, evaluation of the lumbosacral area is a standard component of the newborn physical examination. However, most of the published data concerning cutaneous markers of OSD come from neurosurgery, radiology, or dermatology clinics—completely different populations than the one encountered by general practitioners in the newborn nursery or clinic. In some of these referral populations, cutaneous markers are observed in 51% to 100% of dysraphism patients.1-3
In contrast to this seemingly strong association, our clinical experience in the nursery suggests some of the physical findings identified as markers of spinal dysraphism are common in healthy newborns and would therefore seem to have low positive predictive value for OSD.
The purpose of the current study is to describe the range and frequency of cutaneous lumbosacral and coccygeal findings encountered during the newborn examination in a population of apparently healthy babies, to determine if the prevalence of these findings is associated with race/ethnicity, and to report the frequency of co-occurrence of cutaneous findings.
Methods
Institutional review board approval was obtained. Prior to data collection, both authors reviewed sacral photographs to ensure consistent terminology and interobserver reliability. From February 2, 2015, to December 31, 2015, the lumbosacral area was examined in all neonates 35 weeks or greater estimated gestational age admitted either to the Newborn Nursery or to the Intermediate Intensive Care nursery under the authors’ care. Notation was made of the shape of the gluteal crease as well as any skin findings in the lumbosacral or coccygeal areas.
Gluteal creases were divided into 2 categories: single and duplicated. Single creases were further divided into straight and deviated. Deviated gluteal creases varied in appearance from S-shaped to mostly straight with a superior angulation. Duplicated gluteal creases were classified based on crease appearance above the buttocks. Two main varieties of duplicated gluteal creases were identified: Y-shaped and pitchfork-like. Included in these groups were several variations. Y-shaped creases could be quite distinct with long upper creases or barely visible with short upper creases. They could have a prominent central crease associated with an angulated second or could be composed of angulated creases bilaterally. Duplicated creases were often asymmetric, with one side longer than the other or one/both side(s) present as a discontinuous crease.
Dimples were classified as “simple,” “deep,” or “atypical.” Simple dimples included open, shallow depressions as well as discrete, pinpoint-like pits. Dimples were classified as “deep” if stretching the surrounding skin did not allow identification of the base of the depression. “Atypical” dimples were depressions located above the gluteal crease, in the lumbosacral area.
Lumbosacral hairiness occurred in 3 forms: diffuse lumbosacral hair, coccygeal hair, and a combination of both lumbosacral and coccygeal hair. Lumbosacral hairiness was symmetrically distributed over the lower back in all patients who had it, but the quantity of hair varied. Hair found over the coccyx was seen across a spectrum of intensity. In some patients, coccygeal hair was minimal (approximately 10-20 strands of dark hair); it was more obvious in others (small but easily visible concentration of dark hairs, approximately 50-100 strands). When both lumbosacral and coccygeal hair were present, the 2 areas of hairiness were roughly continuous (Figure 1).

Photographs of commonly noted lumbosacral cutaneous physical examination findings. A. Single, deviated gluteal crease with dimple. B. Duplicated gluteal crease. C. Small but visible concentration of coccygeal hair. D. Notable increase of both sacral and coccygeal hair.
Slate-grey patches were frequently seen in our patients, but only noted for this study if present in the lumbosacral or coccygeal area. All were flat macules or patches ranging in size from very small (<1 cm in diameter) to large (>6 cm). Both single and multiple spots were observed. Intensity of color varied from light grey to dark grey-blue. Midline or midline-crossing lesions were common.
Skin tags were defined as small (<5 mm) raised lesions. The vascular lesions observed were flat red-pink blanchable macules. Some lesions consisted of 1 homogeneous macule in the lumbosacral area; some were a spotty collection of small pink macules.
Imaging of the spine was only ordered if it was clinically indicated in the judgment of any physician caring for the baby during the hospital stay.
Racial and ethnic classification of the newborn was obtained from the medical record and reflected the mother’s self-classification of her own race/ethnicity. If the father’s racial classification was known and different from the mother, the infant was classified as “other.”
Of the 1121 infants examined, detailed descriptions of the lumbosacral area and complete demographic information were available for 1096 infants. Statistical analysis was performed after those with incomplete data were excluded. We examined whether frequencies varied by race/ethnicity, based on Fischer’s exact tests and using log binomial regression to estimate relative risks (RRs) and 95% confidence intervals (CIs) adjusted for infant sex. We examined co-occurrence of the most common physical findings using tetrachoric correlations.
Results
Gender and Race/Ethnicity
Of the 1096 infants included in analysis, 53.7% were male and 46.3% were female. The study population was diverse with respect to race/ethnicity with Hispanic being the most common (Table 1).
Distribution of Lumbosacral Cutaneous Physical Examination Findings by Race-Ethnicity.

Excluding slate-grey macules.
Physical Findings
Several cutaneous lumbosacral and/or coccygeal findings were noted in our cohort: variations of gluteal crease shape, dimples, increased hair, slate-grey patches (Mongolian spots), coccygeal skin tags, and vascular macules (Table 1).
Gluteal Crease Shape
A total of 75.2% of infants had a single, straight gluteal crease. The remaining 24.8% had a deviated or duplicated crease. Deviated single creases were found in 8.3% and duplicated creases were found in 16.3%. None of the patients examined had a deviated crease in association with an underlying mass or obvious abnormality (Figure 1).
All racial/ethnic groups appeared to have a decreased risk for single deviated creases when compared with Caucasians, but the differences were statistically insignificant (Table 2). Only Hispanic infants, whose relative risk of having a single deviated crease was less than half that of Caucasian infants (RR = 0.45), showed a statistically significant difference.

Abbreviations: PI, Pacific Islander; RR, relative risk; CI, confidence interval.
Adjusted for gender.
Coccygeal skin tag data not reported because of small sample size.
Not reported because of small sample size.
Excluding slate-grey patches.
Bold type indicates findings with statistically significant racial differences.
Duplicated gluteal creases similarly showed minimal racial/ethnic difference (Table 2). While African American infants had almost double the risk of a duplicated crease compared with Caucasians (RR = 1.91, 1.03-3.54), the number of infants in this group was small (n = 29). Five infants with duplicated gluteal creases were imaged by sacral ultrasound with normal results (Table 3).
Reported Radiology Results for All Study Infants Who Underwent Ultrasound of Spinal Contents.

Dimples
Dimples were encountered in 15.6% of study patients; 90.9% were simple dimples. All simple dimples were within the gluteal crease and had a visible, skin-covered base; all were <5 mm in size. A few dimples were located in the upper portion of a deviated or Y-shaped crease and were therefore slightly off-midline even though located within the gluteal crease. Deep dimples were noted in 1.5%. Multiple dimples were encountered in 1.4% (n = 15); all but 2 infants had 2 shallow depressions within the gluteal crease. The remaining 2 infants had 2 deep dimples within the gluteal crease. The relative risk of having a dimple was not significantly different between racial/ethnic groups (Table 2). No atypical dimples were found.
Of the 175 newborns with dimples, 8 were referred for ultrasound imaging (Table 3). Four patients with simple dimples had normal ultrasound studies. The 4 remaining patients imaged had deep dimples. Only the infant with 2 deep dimples had an ultrasound finding that may warrant further evaluation.
Hair
In our multiracial population, lumbosacral and/or coccygeal hairiness was encountered in 24.7% of patients. Caucasian infants were least likely to have hair in this area. All other racial/ethnic groups had double to quadruple the risk of lumbosacral hair when compared with Caucasians (Table 2). Faun tail nevus, a distinct triangular patch of abnormally long, coarse hair, was not observed in study patients.
Slate-Grey Patches (Mongolian Spots)
We found lumbosacral/coccygeal slate-grey patches in 44.1% of our patients. As expected, slate-grey patches were uncommon in Caucasians. Of infants born to Caucasian mothers, only 9.6% manifested this cutaneous finding. All other racial/ethnic groups were significantly more likely to have slate-grey patches, with a relative risk at least 5 times higher than Caucasians (Table 2).
Skin Tags
In our patients, skin tags were only found within the gluteal crease over the coccyx. Only 7 of our 1096 patients (0.6%) had coccygeal skin tags. No racial/ethnic differences were noted. One was sent for imaging and had a normal ultrasound (Table 3).
Vascular Lesions
Fourteen of our 1096 patients (1.3%) had vascular macules in the lumbosacral area. All were easily visible on the back, above the superior end of the gluteal crease. None of the lesions were raised or located over the coccyx or within the gluteal crease. Lesion size ranged from 0.5 to 2 cm. No racial/ethnic differences were noted. Ultrasound imaging was performed on 4 infants with vascular macules. One had a slightly low-lying position of the conus; the remaining 3 had normal ultrasounds (Table 3).
Multiple Lumbosacral Findings
A total of 340 of the 1096 infants (31%) had more than 1 cutaneous lumbosacral finding present; 272 (24.8%) had 2 findings; 60 (5.5%) had 3 findings, and 8 (0.7%) had 4 findings. Tetrachoric correlations were done to identify possible relationships between co-occurring physical findings (Table 4). The most notable positive correlation was found between slate-grey patches and increased hair (+0.26). Since slate-grey patches are common in most racial/ethnic groups and have no known association with OSD, we performed further analysis with slate-grey patches excluded. When slate-grey patches were removed from consideration, 111 of the 1096 infants (10%) had 2 findings and 11 (1%) had 3 findings.
Co-Occurrence Between Lumbosacral Physical Examination Findings.
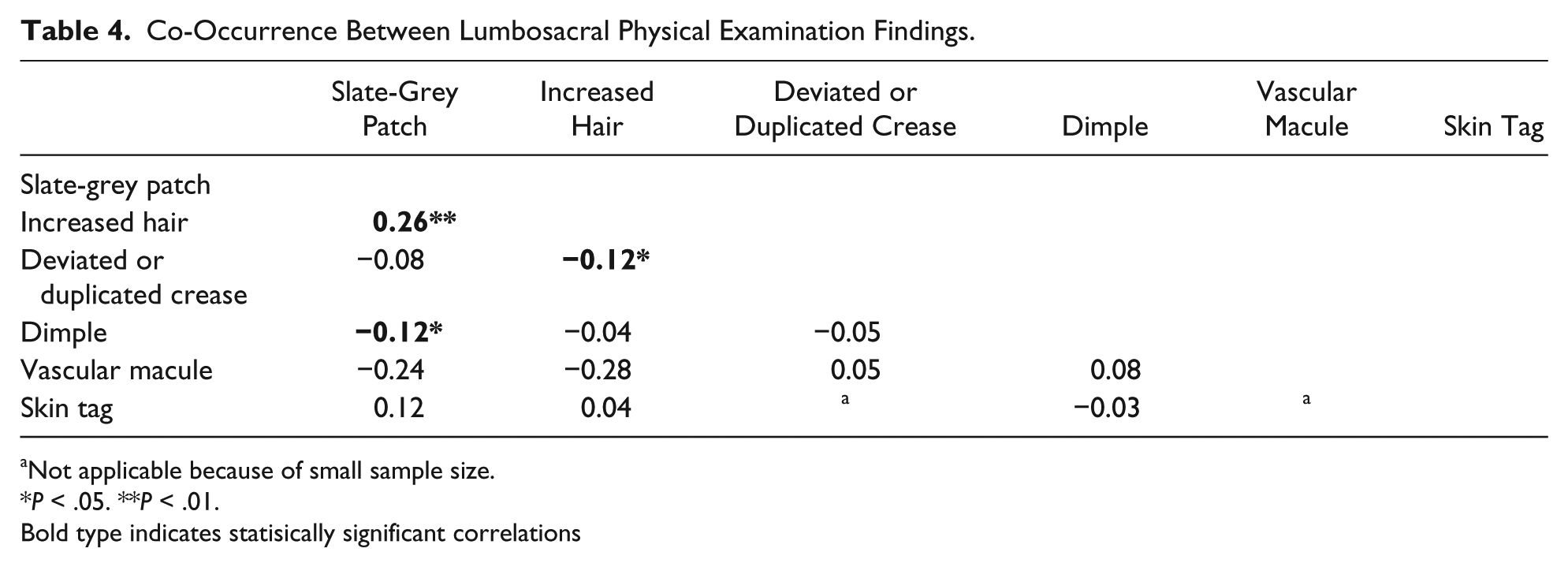
Not applicable because of small sample size.
P < .05. **P < .01.
Bold type indicates statisically significant correlations
A negative correlation was found between vascular macules and increased hair (−0.28). All other correlations were <0.1, suggesting more modest relationships. However, sample sizes for vascular macules and skin tags were small and may have influenced the results.
Discussion
Cutaneous Lumbosacral/Coccygeal Findings Are Common in Healthy Newborns
Two previous studies that focused on the prevalence of lumbosacral findings in healthy newborns have been published.3,4 Both describe dimples in 3% to 7% and skin tags in 0.3% to 0.5%. One also described twisted gluteal folds in 0.8%, pigmented lesions in 0.6%, and lumbosacral hair in 3.3%. 4
Our study found that cutaneous lumbosacral findings are more common in well newborns than previously reported. We found deviated or duplicated gluteal creases in 24.6%, dimples in 16%, increased lumbosacral/coccygeal hair in 24.7%, slate-grey patches in 44.1%, coccygeal skin tags in 0.6%, and flat vascular macules in 1.2%. Broad application of diagnostic labels to our study population allowed for better characterization of subtle variations seen in clinical practice and likely explains our increase in findings.
Racial disparities do exist for some physical findings. Infants of Asian or Hispanic race/ethnicity were significantly more likely than Caucasians to have slate-grey patches and/or increased lumbosacral/coccygeal hair.
Duplicated and Deviated Gluteal Creases Are Common in Healthy Newborns
Almost 25% of our patients had a deviated or duplicated gluteal crease. Our results contrast with several recently published articles, which identify deviated or duplicated gluteal creases as high-risk markers of OSD.5-7 Only recently have authors begun to distinguish isolated deviations and duplications of the gluteal crease (“low-risk”) from deviations and duplications associated with masses or other obviously abnormal physical findings (“high-risk”).8,9
Our data show isolated variations in gluteal crease appearance are common in newborns. In the absence of other concerning findings or symptoms, we believe deviated and duplicated gluteal creases are too common to be useful as markers of OSD.
Simple and Deep Dimples Within the Gluteal Crease Are Common
Historically, much emphasis has been placed on the association of sacral dimples with OSD, but the distinction between “atypical” or high-risk dimples (>2.5 cm above the anus, > 5mm in size, or associated with other high-risk stigmata) and “simple” or low-risk dimples has been made recently. In our cohort, the presence of a dimple was the most common reason for evaluation by ultrasound, with 8 of 14 ultrasounds ordered for this indication. Half of those were done on infants with single, simple dimples. All 4 studies were normal.
Multiple studies have concluded that solitary simple dimples are not useful markers for OSD.1,4,10-12 Although we separated deep dimples from simple dimples in our sample, some now question the necessity of this approach. A 2015 American Academy of Pediatrics Clinical Report categorically dismissed any significance of dimple depth and instead urged examiners to focus primarily on the location of the dimple, using placement above or below the superior edge of the gluteal crease to determine for risk level. 9 All of the deep dimples in our cohort were located below the superior edge of the gluteal crease. Although all 4 patients with deep dimples who underwent ultrasounds had sonographic findings reported, only one had findings (low conus at L3) that may prompt a change in clinical care, so the benefit of having the information remains uncertain.
Lumbosacral and/or Coccygeal Hair Is Common, Particularly in Some Racial/Ethnic Groups
In our multiracial population, hairiness in the lumbosacral/coccygeal area was present in almost one quarter of patients. This cutaneous finding is so familiar to our providers that none of these patients were referred for ultrasound. Others may be less comfortable with visible hair in the lumbosacral area. One recent study found that 10% of infants referred for lumbar ultrasound were sent for concerns related to a “hairy patch.” 13
Recent review articles draw conflicting conclusions about the significance of lumbosacral/coccygeal hair. One considers “hypertrichosis” to be intermediate risk; the other splits patients with hypertrichosis into both high-risk and low-risk groups, depending on the appearance/pattern of the hair.9,14
The lack of agreement with regard to lumbosacral/coccygeal hair is likely due in part to ambiguous terminology used to describe the hair. “Hair tuft,” 15 “hairy patch,” and “hypertrichosis” have all been used as labels for both high-risk and low-risk cutaneous markers.9,14,16 We attempted to clearly describe the nature of the lumbosacral/coccygeal hairiness we encountered in order to distinguish this “low-risk” finding from hair patterns that should rightly be considered “high-risk” markers for OSD.
The Combination of 2 or More “Low-Risk” Cutaneous Findings Is Common
Slate-grey patches have never been associated with OSD. Slate-grey patches were included in this study for 2 reasons: they are commonly found in the lumbosacral area, and they could be misinterpreted as abnormal discoloration of the skin, a “high-risk” marker for OSD. In our cohort, 31% of patients had 2 or more cutaneous findings. The most frequent combination was slate-grey patches + increased hair. When slate-grey patches were excluded, 111 patients (10%) had 2 findings and 11 patients (1%) had 3 findings. Combinations of deviated or duplicated gluteal crease + dimple, deviated or duplicated crease + hair, and dimple + hair were common groupings.
Findings present in 11% of healthy newborns are unlikely to be useful markers for a rare condition like OSD (estimated incidence 0.04%). 6 Therefore, we could consider these patients low risk for having OSD.
The dilemma of whether to image a newborn with 2 or more findings is a common one for primary care providers. One recent review found 25% of newborns sent for spinal ultrasonography were referred for concern over 2 or more findings. 17 Another study found 3.7% of the infants sent for lumbar ultrasound were referred for this reason. 13 Not surprisingly, almost half of those (n = 14) had a dimple + hair combination.
It is critically important to draw a clear distinction between 2 or more “low-risk” markers and 2 or more “high-risk” markers (eg, atypical dimples, lumbar masses, large pedunculated lesions, raised lumbar hemangiomas, highly unusual hair pattern). As our data show, high-risk markers are distinctly unusual. We did not encounter any patients with high-risk markers in this study, making the incidence of these unusual findings in our patient population less than 0.09%. Even one high-risk marker is enough to cause concern. The combination of 2 or more high-risk markers in one patient should certainly prompt further evaluation.
Limitations
Before the study, we reviewed photographs of various cutaneous findings in order to develop standard definitions and nomenclature. However, because we each examined only our own patients, we could not measure the interobserver reliability of our assessments. It is therefore possible that other physicians examining the same cohort of patients would report a different incidence of these various findings.
An inherent problem affecting interobserver reliability is the lack of precise diagnostic criteria for many of the cutaneous markers under discussion. How deep is a deep dimple? Is a depression a dimple? What amount of hair should be considered “increased”? Because of these ambiguities and because there are variations in clinical practice regarding the recognition of these entities, we allowed ourselves to be broad and inclusive in applying these diagnostic labels. We believe this is why our incidence of some cutaneous findings is considerably higher than previously reported. However, we see value in this approach. Clinicians with limited clinical experience may not have the confidence to dismiss equivocal findings as being within the range of normal. The inclusion of these minimally different examination findings is meant to accurately portray the real-life landscape by describing the full spectrum of cutaneous findings that might cause a newborn examiner to have concern.
An observational study cannot answer questions related to positive predictive values or outcomes. One may reasonably conclude that a finding present in 25% of the population would have a poor positive predictive value for OSD, a condition believed to affect 0.04% of the population, but unless all infants are followed prospectively, we cannot know the predictive value of any of these cutaneous findings. Additionally, only a few infants underwent ultrasonography in our study population to exclude OSD.
An obvious limitation of our study was the inability to evaluate the frequency of known “high-risk” cutaneous stigmata. Although we have both encountered such findings previously, they are rare in the healthy newborn population and were not represented in our current sample.
Conclusion
Coccygeal dimples, increased lumbosacral and/or coccygeal hair, deviations and/or duplications of the gluteal crease, and lumbosacral slate-grey patches are all common in healthy newborns. Increased lumbosacral and/or coccygeal hair and slate-grey patches are relatively uncommon in Caucasian infants, but are frequently seen in every other ethnic/racial group.
A combination of 2 or more low-risk cutaneous findings is seen in 11% of newborns. Distinction between low-risk and high-risk findings is important when deciding which patients need further evaluation. Further studies in well newborns are needed to guide optimal clinical management of patients with cutaneous lumbosacral findings.
Footnotes
Acknowledgements
The authors thank Suzan Carmichael and Peiyi (Peggy) Kan (Stanford University) for reviewing our data, providing statistical analysis, and for reviewing our article. The authors also thank Dr. Brandon Rocque (Assistant Professor of Neurosurgery, University of Alabama) for reviewing our abnormal ultrasounds to provide clinical input.
Author Contributions
JA: Contributed to the conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically reviewed the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JLK: Contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically reviewed the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.